Optimizing Perioperative Pain Management in Shoulder Surgery: An Academic Review
Key Takeaway
Optimizing perioperative pain management in shoulder surgery is crucial for enhancing recovery, improving functional outcomes, and boosting patient satisfaction. It significantly reduces opioid consumption, mitigating side effects, and facilitates early, active participation in rehabilitation. A deep understanding of surgical anatomy and regional anesthesia techniques is key to achieving these superior patient-centered results.
Introduction and Epidemiology
Adequate perioperative pain management is a cornerstone of modern shoulder surgery, directly influencing patient recovery trajectories, functional outcomes, and satisfaction. Shoulder pathologies are a significant cause of morbidity, with surgical interventions for conditions such as rotator cuff tears, instability, osteoarthritis, and fractures being increasingly common. The global burden of these conditions underscores the need for optimized surgical and perioperative care pathways.
The historical context of regional anesthesia dates back to William Halsted's pioneering use of cocaine for peripheral nerve blockade in 1885. Over the past three decades, there has been a significant surge in the adoption of peripheral nerve blocks for managing postoperative pain, particularly in orthopedic surgery. This shift is driven by a robust evidence base demonstrating numerous benefits:
* Decreased hospital length of stay, facilitating a transition from traditional inpatient to outpatient surgical models where appropriate.
* Significant reduction in opioid consumption, thereby mitigating the incidence and severity of opioid-related side effects such as nausea, vomiting, constipation, pruritus, and respiratory depression. This also contributes to addressing the broader public health crisis of opioid dependency.
* Enhanced patient participation in crucial early rehabilitation protocols by providing superior baseline analgesia.
* Improved functional recovery and higher patient satisfaction scores.
* Demonstrable cost-effectiveness by reducing overall resource utilization and complication rates.
A comprehensive understanding of surgical anatomy, meticulous patient selection, and a thorough grasp of the indications, contraindications, and potential complications associated with regional anesthesia techniques are paramount for orthopedic surgeons and anesthesiologists collaborating in the perioperative setting. This guide aims to provide a high-yield academic review of optimizing perioperative pain management for shoulder surgery, integrating contemporary evidence and best practices.
The evolution of Enhanced Recovery After Surgery pathways in orthopedic shoulder procedures has further formalized multimodal analgesia. These protocols emphasize preemptive analgesia, intraoperative regional techniques, and opioid-sparing postoperative regimens. As the volume of complex shoulder arthroplasties and massive rotator cuff repairs migrating to ambulatory surgery centers increases, the reliance on sophisticated, long-acting regional anesthetic techniques becomes absolute.
Surgical Anatomy and Biomechanics
A profound understanding of shoulder anatomy, particularly the neurovascular structures, is indispensable for both safe surgical execution and effective regional anesthesia.
Bony Anatomy
The shoulder complex comprises the scapula, humerus, and clavicle. Key bony landmarks include the glenoid, humeral head, greater and lesser tuberosities, bicipital groove, acromion, coracoid process, and spine of the scapula. The congruity of the glenohumeral joint is inherently unstable, relying heavily on soft tissue restraints.
Ligamentous and Capsular Anatomy
The glenohumeral joint capsule, reinforced by the superior, middle, and inferior glenohumeral ligaments, provides static stability. The coracoacromial ligament forms part of the coracoacromial arch, an important structure in subacromial impingement.
Muscular Anatomy
The rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) are critical for dynamic stability and arm rotation. Other significant muscles include the deltoid, pectoralis major, latissimus dorsi, and biceps brachii.
Neurovascular Anatomy
The brachial plexus is the primary neural supply to the shoulder and upper extremity. It is formed by the ventral rami of spinal nerves C5, C6, C7, C8, and T1.
* Roots: C5, C6, C7, C8, T1 merge to form the trunks.
* Trunks: Superior (C5, C6), Middle (C7), Inferior (C8, T1).
* Divisions: Each trunk divides into anterior and posterior divisions, supplying flexor and extensor compartments, respectively.
* Cords: Lateral, Posterior, Medial, named relative to the axillary artery.
* Terminal Nerves: Major nerves supplying the shoulder and upper limb include the musculocutaneous, axillary, radial, median, and ulnar nerves.

For shoulder surgery, precise targeting of these neural pathways is required to achieve optimal analgesia while minimizing motor blockade and systemic side effects. The sensory innervation of the shoulder joint follows Hilton's Law, which states that the nerves supplying the muscles extending directly across and acting at a given joint also innervate the joint.
The suprascapular nerve (derived from the superior trunk, C5-C6) provides approximately 70 percent of the sensory innervation to the glenohumeral joint, including the posterior and superior capsule, the acromioclavicular joint, and the subacromial bursa. The axillary nerve (derived from the posterior cord, C5-C6) supplies the anterior and inferior joint capsule. The lateral pectoral nerve provides minor contributions to the anterior shoulder joint. Understanding this distribution is critical; blocking the C5 and C6 nerve roots or the superior trunk effectively covers the vast majority of nociceptive input generated during shoulder surgery.
The interscalene groove is the primary anatomical landmark for the most common regional block in shoulder surgery. It is bordered anteriorly by the anterior scalene muscle, posteriorly by the middle scalene muscle, and inferiorly by the first rib. Within this groove, the roots and trunks of the brachial plexus are arranged vertically. The phrenic nerve, derived from C3, C4, and C5, descends obliquely across the anterior surface of the anterior scalene muscle, lying in close proximity to the brachial plexus, which explains the high incidence of hemi-diaphragmatic paresis associated with traditional interscalene blocks.
Indications and Contraindications
Optimizing pain management requires a multimodal approach tailored to the specific surgical intervention, patient comorbidities, and anticipated nociceptive burden. The decision to utilize procedural regional anesthesia versus relying solely on systemic non-operative pain management must be carefully weighed.
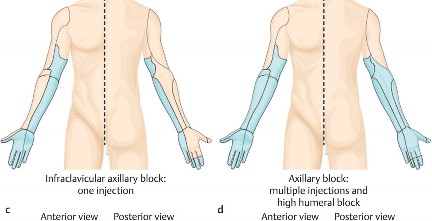
Indications for regional anesthesia, specifically the Interscalene Nerve Block or Superior Trunk Block, include moderate to severely painful procedures such as total shoulder arthroplasty, reverse total shoulder arthroplasty, massive rotator cuff repairs, and stabilization procedures for glenohumeral instability. These blocks provide profound analgesia, allowing for lower volatile anesthetic requirements intraoperatively and facilitating immediate postoperative physical therapy.
Contraindications to peripheral nerve blocks in shoulder surgery can be absolute or relative. Absolute contraindications include patient refusal, active infection at the injection site, and documented allergy to local anesthetics. Relative contraindications require careful risk-benefit analysis and include pre-existing severe pulmonary disease (due to the risk of phrenic nerve blockade), contralateral phrenic nerve palsy, pre-existing neurologic deficits in the operative limb, and severe coagulopathy.
The following table summarizes the indications for interventional regional anesthesia versus systemic multimodal management in the perioperative shoulder setting.
| Modality Category | Primary Indications | Relative Contraindications | Expected Analgesic Duration |
|---|---|---|---|
| Interventional Regional Anesthesia | Total Shoulder Arthroplasty, Rotator Cuff Repair, Fracture Fixation | Severe COPD, Contralateral Phrenic Palsy, Local Infection | 12 to 24 hours |
| Systemic Multimodal Analgesia | Diagnostic Arthroscopy, Minor Debridement, Patient Refusal of Block | Renal Impairment (NSAIDs), Hepatic Failure (Acetaminophen) | Continuous via scheduled dosing |
| Continuous Catheter Block | Complex Revision Arthroplasty, High Opioid Tolerance | Inability to manage pump at home, Coagulopathy | 48 to 72 hours |
| Local Infiltration Analgesia | Subacromial Decompression, Biceps Tenodesis | Local tissue infection | 6 to 12 hours |
Pre Operative Planning and Patient Positioning
The foundation of excellent perioperative pain management is established well before the surgical incision. Preoperative planning involves a comprehensive medical evaluation, optimization of comorbidities, and the initiation of a multimodal analgesic pathway.
Pre-emptive analgesia is a critical component of Enhanced Recovery After Surgery protocols. Administering oral agents prior to surgery aims to decrease central sensitization and downregulate the inflammatory cascade. A standard preoperative cocktail often includes oral acetaminophen, a non-steroidal anti-inflammatory drug (such as celecoxib or meloxicam), and a gabapentinoid (such as gabapentin or pregabalin), provided there are no contraindications.
Ultrasound evaluation of the patient's cervical anatomy is increasingly performed in the preoperative holding area. High-frequency linear ultrasound probes allow the anesthesiologist to map the brachial plexus, identify anatomical variants, and assess the depth and trajectory required for the needle. This pre-scan minimizes procedural time and enhances patient comfort.

Patient positioning is critical for both the administration of regional anesthesia and the execution of the surgical procedure. For the administration of an interscalene or superior trunk block, the patient is typically placed in a supine or semi-lateral position with the head turned slightly away from the operative side. The ipsilateral arm is adducted and pulled gently inferiorly to depress the clavicle and open the supraclavicular fossa.
For the surgical procedure, shoulder surgery is predominantly performed in either the beach chair (modified Fowler's) position or the lateral decubitus position.
The beach chair position provides excellent access to the anterior and superior shoulder, facilitating anatomic orientation and allowing for straightforward conversion to an open procedure if necessary. However, it is associated with unique hemodynamic challenges, notably the Bezold-Jarisch reflex—a triad of profound bradycardia, hypotension, and cardiovascular collapse thought to be triggered by venous pooling in the lower extremities and a hypercontractile, underfilled left ventricle. This reflex can be exacerbated by the sympathetic blockade occasionally seen with high-volume interscalene blocks.
Conversely, the lateral decubitus position provides excellent visualization of the glenohumeral joint, particularly for inferior capsular work and labral repairs. It utilizes balanced suspension and traction, which can lead to neurapraxia if excessive force is applied or if the procedure is prolonged. Traction-related nerve injuries can confound postoperative pain assessments, making it difficult to distinguish between surgical pain, block failure, or positioning-related neuropathy.
Detailed Surgical Approach and Technique
While regional anesthesia provides the foundation for pain control, meticulous surgical technique, respect for soft tissue planes, and efficient operative execution are equally critical in minimizing the postoperative nociceptive burden. The degree of surgical trauma directly correlates with the release of inflammatory mediators (prostaglandins, leukotrienes, cytokines) that sensitize peripheral nociceptors.
The Deltopectoral Approach
The deltopectoral approach remains the workhorse for open shoulder surgery, including arthroplasty and fracture fixation. It utilizes a true internervous plane, minimizing denervation and subsequent muscle atrophy.
The incision is made along the line connecting the coracoid process to the insertion of the deltoid on the humerus. Subcutaneous dissection reveals the cephalic vein, which marks the interval between the deltoid (innervated by the axillary nerve) and the pectoralis major (innervated by the medial and lateral pectoral nerves).
The vein is typically retracted laterally with the deltoid to preserve its venous drainage, though medial retraction is preferred by some surgeons. The clavipectoral fascia is incised, exposing the conjoint tendon (short head of the biceps and coracobrachialis). Careful retraction of the conjoint tendon medially and the deltoid laterally exposes the subscapularis and the anterior joint capsule.
From a pain management perspective, excessive retraction forces on the deltoid or conjoint tendon must be avoided to prevent neurapraxia of the axillary or musculocutaneous nerves, respectively. Meticulous hemostasis and anatomical repair of the subscapularis during closure reduce hematoma formation, a known source of postoperative pain and stiffness.
Arthroscopic Portal Placement
For minimally invasive procedures, precise portal placement is essential to avoid neurovascular injury and minimize tissue trauma. The standard posterior portal is established in the "soft spot" between the infraspinatus and teres minor. The anterior portal is typically established via an outside-in technique through the rotator interval, bordered by the supraspinatus superiorly, subscapularis inferiorly, and the long head of the biceps laterally. Blind establishment of portals or multiple passes through the musculature increases localized tissue damage and postoperative pain.
Regional Anesthesia Techniques
The execution of the regional nerve block is a highly specialized procedural skill. The Ultrasound-Guided Interscalene Nerve Block is the gold standard.
Using a high-frequency linear transducer placed transversely across the neck at the level of the cricoid cartilage, the sternocleidomastoid muscle is identified. Sliding laterally, the anterior and middle scalene muscles are visualized. Between them lies the brachial plexus, which at this level typically appears as three to five hypoechoic, nodular structures resembling a "stoplight" (the C5, C6, and C7 nerve roots).

An echogenic block needle is advanced in-plane from lateral to medial. The target is the fascial sheath surrounding the nerve roots. Injection of local anesthetic (commonly 0.5 percent bupivacaine or 0.5 percent ropivacaine) should result in anechoic fluid spreading around the nerve roots, separating them from the surrounding musculature. To prolong the duration of the block, adjuvants such as perineural dexamethasone (typically 4 mg) or dexmedetomidine may be added. Liposomal bupivacaine is also utilized in some centers to extend analgesia up to 72 hours, though its superiority over standard bupivacaine with dexamethasone remains a subject of academic debate.
To mitigate the risk of phrenic nerve blockade, the Superior Trunk Block has emerged as a refined alternative. By scanning further distal in the supraclavicular fossa, the C5 and C6 roots are seen merging to form the superior trunk. Blocking the plexus at this more distal location significantly increases the distance between the injection site and the phrenic nerve, drastically reducing the incidence of hemi-diaphragmatic paresis while maintaining equivalent analgesia for shoulder surgery.
Complications and Management
Despite the profound benefits of multimodal analgesia and regional anesthesia, complications can occur. Rapid recognition and protocolized management are essential to prevent long-term morbidity.
Local Anesthetic Systemic Toxicity is a rare but potentially fatal complication resulting from inadvertent intravascular injection or rapid systemic absorption of local anesthetic. Symptoms progress from central nervous system excitation (tinnitus, perioral numbness, metallic taste, agitation) to CNS depression (seizures, coma) and ultimately cardiovascular collapse (arrhythmias, asystole). Management requires immediate cessation of the injection, airway management, seizure control (typically with benzodiazepines), and the prompt administration of 20 percent Intravenous Lipid Emulsion therapy.
Phrenic nerve palsy resulting in hemi-diaphragmatic paresis is a highly predictable side effect of traditional high-volume interscalene blocks, occurring in nearly 100 percent of patients. While well-tolerated in healthy individuals, it can cause acute respiratory failure in patients with severe chronic obstructive pulmonary disease, obesity hypoventilation syndrome, or pre-existing contralateral diaphragmatic dysfunction.
Rebound pain is a significant clinical challenge characterized by a severe, disproportionate increase in pain upon the resolution of the nerve block. It typically occurs 12 to 24 hours postoperatively. Mitigation strategies include transitioning the patient to oral multimodal analgesics well before the anticipated block resolution, utilizing continuous catheter techniques, or employing long-acting adjuvants.

The following table outlines common complications associated with perioperative pain management in shoulder surgery, their approximate incidence, and salvage strategies.
| Complication | Approximate Incidence | Clinical Presentation | Salvage Strategy and Management |
|---|---|---|---|
| Phrenic Nerve Palsy | 90-100% (Standard ISB) | Dyspnea, decreased breath sounds at lung base | Supportive care, supplemental oxygen; utilize Superior Trunk Block or low-volume techniques in high-risk patients. |
| Rebound Pain Phenomenon | 30-40% | Severe, sudden onset pain 12-24 hours post-op | Pre-emptive overlapping oral analgesics, continuous nerve block catheters, aggressive multimodal bridging. |
| Horner's Syndrome | 20-30% | Ptosis, miosis, anhidrosis | Reassurance; resolves spontaneously with block dissipation. Caused by sympathetic chain blockade. |
| Peripheral Neuropathy | 0.5-2.0% | Persistent paresthesia, motor deficit beyond block duration | Neurologic exam, EMG/NCS at 3-4 weeks if unresolved; rule out surgical traction injury vs. direct needle trauma. |
| Local Anesthetic Systemic Toxicity | < 0.1% | Tinnitus, perioral numbness, seizures, arrhythmias | Immediate airway support, ACLS, 20% Intravenous Lipid Emulsion (Lipid Rescue protocol). |
Post Operative Rehabilitation Protocols
The ultimate goal of optimizing perioperative pain management is to facilitate early, painless, and effective postoperative rehabilitation. The shoulder is uniquely prone to postoperative stiffness (arthrofibrosis), making early mobilization critical for procedures where immediate motion is permitted, such as arthroplasty or subacromial decompression.
Postoperative rehabilitation is generally divided into distinct phases, which are heavily dependent on the surgical procedure performed and the quality of tissue fixation.
Phase I typically involves passive range of motion. Effective regional analgesia allows the physical therapist to range the shoulder without eliciting muscle guarding or spasms, which can place undue stress on surgical repairs. Continuous peripheral nerve block catheters are particularly advantageous in this phase for complex cases, providing titratable analgesia for up to 72 hours.
Phase II transitions to active-assisted range of motion, requiring the patient to engage their musculature. As the regional block dissipates, the transition to systemic multimodal oral analgesics must be seamless. The reliance on scheduled acetaminophen and NSAIDs, supplemented by short-acting opioids only for breakthrough pain prior to therapy sessions, is the standard of care.
Phase III involves active motion and strengthening. By this stage, surgical inflammatory pain has typically subsided, and pain is more mechanical or related to muscle fatigue. Cryotherapy systems, often applied immediately postoperatively and continued through the rehabilitation phases, serve as an excellent non-pharmacologic adjunct. Continuous cold therapy reduces local tissue metabolism, limits edema, and decreases nerve conduction velocity, providing a synergistic analgesic effect.
Summary of Key Literature and Guidelines
The optimization of perioperative pain management in shoulder surgery is continuously evolving, guided by robust clinical research and societal guidelines.
The American Society of Regional Anesthesia and Pain Medicine (ASRA) provides comprehensive guidelines on the use of regional anesthesia, emphasizing the routine use of ultrasound guidance to improve block success rates and decrease the incidence of vascular puncture and local anesthetic systemic toxicity.
Recent literature has heavily focused on diaphragm-sparing alternatives to the traditional interscalene block. Landmark anatomical and clinical studies comparing the Interscalene Block to the Superior Trunk Block have demonstrated that the STB provides non-inferior analgesia for major shoulder surgery while significantly reducing the incidence of complete hemi-diaphragmatic paresis. This represents a critical paradigm shift, particularly for the ambulatory surgical population and patients with borderline pulmonary reserve.
Furthermore, the PROSPECT (Procedure-Specific Postoperative Pain Management) working group recommendations for shoulder surgery strongly advocate for a procedure-specific, multimodal approach. The guidelines recommend the routine use of preoperative oral analgesics, intraoperative regional techniques as the primary analgesic modality, and the strict minimization of postoperative opioids to facilitate rapid recovery and reduce opioid-related adverse events. Adherence to these evidence-based protocols ensures that orthopedic surgeons and anesthesiologists provide the highest standard of care, optimizing both patient safety and functional outcomes following shoulder surgery.
Clinical & Radiographic Imaging
You Might Also Like