Lunate Fractures and Kienböck Disease: Comprehensive Surgical Management

Key Takeaway
Kienböck disease and lunate fractures present complex biomechanical challenges in hand surgery. This comprehensive guide details the vascular anatomy of the lunate, the Lichtman staging system for avascular necrosis, and evidence-based surgical interventions. From joint-leveling procedures like radial shortening osteotomy to metaphyseal core decompression and salvage operations, master the indications, operative techniques, and postoperative protocols required to restore carpal stability and alleviate radiocarpal degeneration.
Comprehensive Introduction and Patho-Epidemiology
The lunate functions as the critical keystone of the proximal carpal row, serving as the primary mechanical link between the radius and the distal carpus. Its unique intercalated position dictates that it must absorb, transmit, and dissipate immense axial loads during routine wrist kinematics. Pathologies affecting the lunate span a broad spectrum, ranging from high-energy acute traumatic fractures to the insidious, progressive osteonecrosis known as Kienböck disease. Managing these conditions demands a profound, nuanced understanding of carpal kinematics, the fragile intraosseous vascular anatomy, and an array of advanced surgical techniques designed to restore biomechanical equilibrium.
Acute fractures of the lunate are relatively rare, accounting for less than 1% to 4% of all carpal fractures. This rarity is largely attributed to the lunate's protected position within the lunate fossa of the distal radius and its robust ligamentous envelope. When acute fractures do occur, they are typically the result of high-energy trauma, such as a fall from a height or a motor vehicle collision, often loading an extended, ulnar-deviated wrist. These injuries are notoriously difficult to detect on standard posteroanterior (PA) and lateral plain radiographs due to the complex superimposition of the radial styloid, scaphoid, and triquetrum. Consequently, a high index of suspicion and advanced cross-sectional imaging are mandatory for any patient presenting with persistent central dorsal wrist pain following trauma.
Conversely, Kienböck disease (avascular necrosis of the lunate) typically presents insidiously, most frequently observed in patients between 15 and 40 years of age. Epidemiological data suggest a strong predilection for the dominant wrist of men engaged in heavy manual labor, pointing toward repetitive microtrauma as a significant etiologic factor. Patients typically present with chronic dorsal wrist pain, localized swelling, progressive loss of grip strength, and a restricted arc of motion. Crucially, the clinical symptoms of Kienböck disease can precede definitive radiographic evidence of osteonecrosis by up to 18 months, making early diagnosis highly dependent on magnetic resonance imaging (MRI).

The pathophysiology of Kienböck disease is widely considered multifactorial, representing a catastrophic intersection of vascular susceptibility and adverse biomechanical loading. When the fragile blood supply of the lunate is compromised—whether by a discrete occult fracture, repetitive shear stress, or microvascular thrombosis—the resulting ischemia weakens the trabecular architecture. Continued biomechanical compressive forces exerted by the capitate exacerbate this ischemia, creating a vicious cycle of microfracture, collapse, and progressive carpal derangement. Understanding this patho-epidemiological cascade is paramount for the orthopedic surgeon, as it dictates the timing and selection of surgical interventions aimed at halting disease progression before pancarpal arthritis ensues.
Detailed Surgical Anatomy and Biomechanics
The vascular anatomy of the lunate is the fundamental anatomic determinant in the pathogenesis of Kienböck disease. Gelberman et al. meticulously delineated the extraosseous and intraosseous vascularity of the lunate through extensive cadaveric microangiographic studies. The extraosseous blood supply is derived from a rich anastomotic network formed by the radiocarpal and intercarpal arches, which feed the lunate via dorsal and volar ligamentous attachments. However, it is the intraosseous vascular pattern that dictates the bone's susceptibility to ischemic necrosis.

Gelberman identified three distinct patterns of intraosseous vessels entering the lunate: the Y, I, and X patterns. More importantly, he discovered that approximately 20% of lunates possess a single intraosseous vessel or have only one surface (typically the volar pole) exposed to the blood supply, lacking robust internal anastomoses. This "high-risk" vascular watershed pattern explains why seemingly innocuous wrist sprains or repetitive loading can evolve into devastating osteonecrosis if an occult lunate fracture disrupts this solitary vascular tether.
Biomechanically, the lunate acts as an intercalated segment, meaning it has no direct tendinous insertions to govern its motion. Instead, its kinematics are entirely dictated by the contour of its articular surfaces and the complex tensioning of its capsuloligamentous constraints, primarily the scapholunate (SL) and lunotriquetral (LT) interosseous ligaments. During the functional "dart-thrower's motion" (radial extension to ulnar flexion), the proximal carpal row must dynamically adapt. The lunate normally flexes during wrist radial deviation and extends during ulnar deviation. When structural collapse occurs in advanced Kienböck disease, this synchronous motion is uncoupled, leading to a dorsal intercalated segmental instability (DISI) pattern as the scaphoid flexes unopposed.
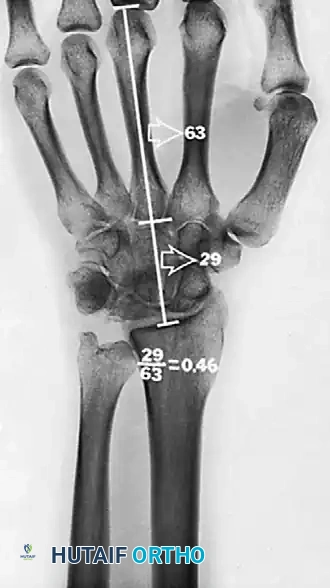
The concept of ulnar variance, first introduced by Hultén, is a critical biomechanical parameter in the evaluation of lunate pathology. Hultén described the "ulna-minus variant" (negative ulnar variance), noting that in 78% of patients with Kienböck disease, the ulna was shorter than the radius at their distal articulation, compared to only 23% in the asymptomatic population. Negative ulnar variance alters the load distribution across the radiocarpal joint, disproportionately increasing the shear and compressive forces transmitted directly from the radius and capitate to the lunate. This concentrated mechanical stress accelerates trabecular fragmentation in an already ischemic bone, forming the biomechanical rationale for joint leveling procedures.
Exhaustive Indications and Contraindications
The surgical management of lunate fractures and Kienböck disease is highly algorithm-driven, relying heavily on the morphological classification of the pathology, the patient's ulnar variance, and the integrity of the adjacent articular cartilage. For acute lunate fractures, nonoperative management is strictly reserved for truly nondisplaced fractures or highly comminuted fractures without articular step-off, provided the patient can comply with 6 to 8 weeks of rigid cast immobilization. Operative intervention (Open Reduction and Internal Fixation - ORIF) is absolutely indicated for fractures demonstrating greater than 1 mm of articular step-off, significant gap formation, or avulsion fractures at the dorsal pole that compromise the dorsal radiocarpal ligamentous complex.
For Kienböck disease, the universally accepted Lichtman classification system dictates surgical indications. Stage I and early Stage II disease (pre-collapse) in the setting of negative ulnar variance are prime indications for joint leveling procedures, primarily radial shortening osteotomy (RSO). If the patient presents with ulnar-neutral or positive variance, RSO is contraindicated due to the risk of inducing severe ulnocarpal impaction. In these neutral/positive variance cases, radial closing wedge osteotomies, metaphyseal core decompression, or vascularized bone grafting (VBG) are indicated to alter load vectors or stimulate angiogenesis without altering relative ulnar length.



As the disease progresses to Stage IIIA (lunate collapse without fixed scaphoid rotation), joint leveling remains a viable option provided the radiolunate cartilage is pristine. However, once the disease reaches Stage IIIB (fixed DISI deformity and proximal capitate migration), joint leveling and revascularization are absolutely contraindicated. The internal collapse pattern cannot be reversed by altering extra-carpal mechanics. Indications for Stage IIIB shift to salvage procedures, such as Proximal Row Carpectomy (PRC) or Scaphoid-Trapezium-Trapezoid (STT) fusion. Stage IV disease, characterized by secondary pancarpal osteoarthritis, mandates total wrist arthrodesis or wrist arthroplasty, as the articular surfaces are beyond salvage.
| Pathology / Lichtman Stage | Primary Surgical Indications | Absolute Contraindications |
|---|---|---|
| Acute Lunate Fracture | >1mm step-off, displaced avulsions, SL/LT ligament compromise. | Nondisplaced fractures (manage in cast), active local infection. |
| Stage I Kienböck | Core Decompression, Immobilization. | Joint leveling if ulnar positive; salvage procedures. |
| Stage II Kienböck | Radial Shortening Osteotomy (if ulnar minus), VBG, Wedge Osteotomy. | RSO in ulnar positive/neutral variance. |
| Stage IIIA Kienböck | RSO (if ulnar minus), VBG, STT Fusion. | Advanced radiocarpal arthritis, fixed DISI deformity. |
| Stage IIIB Kienböck | Proximal Row Carpectomy (PRC), STT Fusion. | Joint leveling, VBG, PRC if capitate head is arthritic. |
| Stage IV Kienböck | Total Wrist Arthrodesis, Wrist Arthroplasty. | PRC, Partial intercarpal fusions, Joint leveling. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical execution in lunate pathology. Standard posteroanterior (PA), lateral, and oblique radiographs of the wrist are mandatory but frequently insufficient for definitive surgical planning. The PA view must be taken with the shoulder abducted to 90 degrees, elbow flexed to 90 degrees, and forearm in neutral rotation (the "zero PA" view) to accurately assess ulnar variance. Pronation artificially increases ulnar variance, while supination decreases it, potentially leading to erroneous surgical decision-making regarding joint leveling.

Advanced imaging is non-negotiable. Thin-slice computed tomography (CT) with sagittal and coronal reformats is required to definitively identify occult fracture patterns, assess the degree of lunate comminution, and evaluate the precise geometry of the anterior pole. CT is also critical for evaluating the articular cartilage space and the presence of subchondral cysts in the adjacent capitate or radius. Magnetic Resonance Imaging (MRI) remains the gold standard for early diagnosis (Stage I), demonstrating decreased signal intensity on T1-weighted images and increased signal on T2-weighted images (edema) before any sclerotic changes are visible on plain radiographs.

For radial shortening osteotomies, precise pre-operative templating is mandatory. The surgeon must calculate the exact millimeter resection required to achieve neutral or slightly negative (0 to -1 mm) ulnar variance. Over-shortening the radius by even 1 to 2 mm beyond neutral can lead to devastating ulnocarpal impaction syndrome and severe incongruity of the distal radioulnar joint (DRUJ). Templating involves overlaying digital templates of the chosen volar locking or dynamic compression plate to ensure adequate distal purchase without penetrating the radiocarpal joint.
Patient positioning for all lunate and carpal procedures involves placing the patient supine with the operative extremity extended on a radiolucent hand table. A well-padded proximal arm tourniquet is applied. The mini C-arm fluoroscopy unit should be positioned parallel to the table, coming in from the head or the foot of the table to allow unhindered orthogonal imaging without compromising the sterile field. The arm is prepped and draped in standard sterile fashion, ensuring exposure from the fingertips to the mid-arm to allow for potential bone graft harvest from the distal radius or olecranon.
Step-by-Step Surgical Approach and Fixation Technique
Acute Lunate Fracture Fixation and Core Decompression
For acute displaced lunate fractures, a dorsal approach to the wrist is most commonly utilized. A longitudinal incision is centered over the Lister tubercle. The extensor retinaculum is incised over the third extensor compartment, and the extensor pollicis longus (EPL) tendon is transposed radially. The fourth compartment is elevated subperiosteally. A ligament-sparing dorsal capsulotomy (such as a Berger flap) is performed to expose the proximal carpal row. Fracture hematoma is evacuated, and reduction is achieved using 0.045-inch K-wires as joysticks. Fixation is typically secured using multiple small headless cannulated compression screws (1.5 mm or 2.0 mm) buried beneath the articular cartilage.

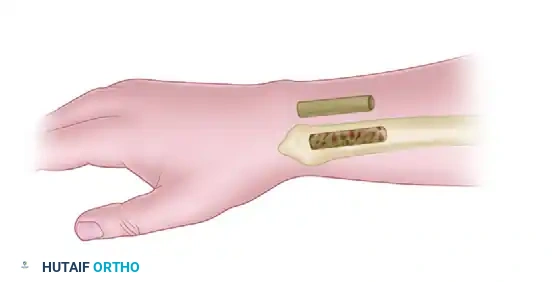
For early-stage Kienböck disease, metaphyseal core decompression is a less invasive alternative aimed at stimulating a regional acceleratory phenomenon (RAP). A small incision is made over the distal radial metaphysis, and a 1 cm cortical window is created. Extensive curettage of the cancellous bone within the distal radius is performed, extending toward the lunate fossa. The cortical window is then replaced, and the wound is closed without internal fixation. This surgical trauma induces a robust local vascular healing response that can revascularize the ischemic lunate without altering gross carpal mechanics.
Radial Shortening Osteotomy (RSO)
Radial shortening is the preferred joint leveling procedure for ulnar-minus variants. A volar Henry approach is utilized to expose the distal radius. The flexor carpi radialis (FCR) sheath is incised, and the artery is protected radially. The pronator quadratus is elevated from its radial border to expose the volar metadiaphysis. A specialized shortening plate with an integrated cutting jig is temporarily affixed to the diaphysis.

A transverse or oblique osteotomy is performed approximately 3 inches (7.6 cm) proximal to the distal articular surface. Using parallel saw blades, the exact templated amount of bone (typically 2 to 3 mm) is resected. The distal radial fragment is then translated proximally, closing the osteotomy gap. The plate is secured distally, and dynamic compression is applied across the osteotomy site using eccentric drilling in the proximal holes. Rigid fixation with a 3.5 mm dynamic compression plate or locking compression plate is mandatory to prevent nonunion.
Salvage Procedures: Proximal Row Carpectomy and Fusions
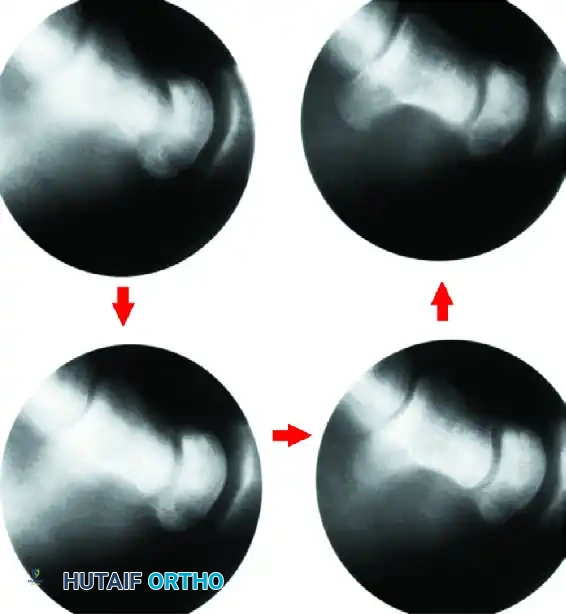
When the lunate has collapsed and the scaphoid has rotated into a fixed DISI pattern (Stage IIIB), Proximal Row Carpectomy (PRC) is a highly reliable salvage procedure. A dorsal approach is utilized. The scaphoid, lunate, and triquetrum are meticulously excised. It is critical to preserve the volar radioscaphocapitate (RSC) ligament to prevent ulnar translation of the remaining carpus. The capitate head is then seated into the lunate fossa of the radius, converting the complex wrist joint into a simple hinge. This procedure requires a pristine capitate head; if capitate arthritis is present, PRC is contraindicated.


Alternatively, Scaphoid-Trapezium-Trapezoid (STT) fusion can be employed to halt the DISI collapse pattern and unload the lunate by transferring forces through the scaphoid column. The articular surfaces of the STT joint are decorticated, cancellous bone graft is interposed, and fixation is achieved with K-wires, staples, or headless screws. For Stage IV pancarpal arthritis, Total Wrist Arthrodesis is the ultimate salvage. A dorsal spanning plate is applied from the radius to the third metacarpal, sacrificing all wrist motion in exchange for reliable, durable pain relief.


Complications, Incidence Rates, and Salvage Management
Surgical intervention for lunate pathology is fraught with potential complications, primarily due to the tenuous vascularity of the carpus and the precise biomechanical tolerances of the wrist joint. Following radial shortening osteotomy, the most devastating complication is nonunion of the radial diaphysis, which occurs in approximately 2% to 4% of cases, often necessitating revision ORIF with structural bone grafting. Over-shortening of the radius is a catastrophic technical error that leads to iatrogenic ulnocarpal impaction syndrome and DRUJ incongruity, presenting with severe ulnar-sided wrist pain and limited forearm rotation.
Despite successful execution of joint leveling or revascularization procedures, the unpredictable natural history of Kienböck disease means that progressive lunate collapse occurs in up to 20% of patients over a 10-year follow-up period. Patients must be counseled pre-operatively that these procedures are often "time-buying" operations designed to delay, rather than permanently prevent, the onset of carpal arthritis. If progression to Stage IIIB or IV occurs, the surgeon must be prepared to transition to salvage management.
Complications following salvage procedures are also significant. Proximal Row Carpectomy relies on the articulation between the capitate head and the lunate fossa. Over time, radiocapitate arthritis develops in approximately 15% to 20% of patients, leading to recurrent pain. Limited intercarpal fusions (such as STT fusion) carry a nonunion rate of 5% to 10% and frequently result in hardware impingement or adjacent segment disease at the radiocarpal joint due to altered kinematics.
| Procedure | Primary Complications | Estimated Incidence | Salvage Management |
|---|---|---|---|
| Radial Shortening Osteotomy | Nonunion, DRUJ incongruity, Ulnocarpal impaction. | 2% - 5% | Revision ORIF + graft, Ulnar shortening osteotomy. |
| Vascularized Bone Grafting | Graft failure, Progressive lunate collapse. | 15% - 20% | PRC, STT Fusion, Total Wrist Arthrodesis. |
| Proximal Row Carpectomy | Radiocapitate arthritis, Weak grip strength. | 15% - 20% (long-term) | Conversion to Total Wrist Arthrodesis. |
| STT Fusion | Nonunion, Adjacent segment arthritis, Hardware pain. | 5% - 10% | Revision fusion, Hardware removal, Total Wrist Fusion. |
| Total Wrist Arthrodesis | Plate fracture, Nonunion of CMC joint, Tendon irritation. | 3% - 8% | Revision plating, Hardware removal post-union. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation protocol must be meticulously tailored to the specific surgical procedure performed, balancing the need for rigid immobilization to achieve osseous union with the imperative to prevent debilitating carpal stiffness. Phase 1 (0 to 2 weeks post-operatively) focuses universally on strict immobilization, edema control, and immediate active range of motion of the digits. Patients are placed in a bulky surgical dressing and a volar orthosis. Elevation and digital tendon gliding exercises are initiated on post-operative day one to prevent extensor lag and flexor tendon adhesions.
Phase 2 (2 to 6 weeks) marks the divergence in protocols. For patients who underwent ORIF of an acute lunate fracture or a limited intercarpal fusion (STT), strict cast immobilization (typically a short-arm thumb-spica cast) is maintained to protect the fragile intra-articular fixation or arthrodesis site. Conversely, for patients who underwent a rigidly plated radial shortening osteotomy or a proximal row carpectomy, the cast is transitioned to a removable thermoplastic splint at the 2-week mark. Gentle, therapist-directed active range of motion (AROM) of the radiocarpal and midcarpal joints is initiated, strictly avoiding passive stretching or loading.
Phase 3 (6 to 12 weeks) is dictated by radiographic evidence of clinical union. Once bridging trabeculae are visible at the osteotomy or fusion site, the removable splint is progressively weaned. Active-assisted range of motion (AAROM) and passive range of motion (PROM) are introduced to address residual capsular contractures. Isometric strengthening of the forearm musculature begins, gradually progressing to isotonic grip strengthening exercises. For PRC patients, maximizing the arc of motion is prioritized over heavy strengthening, as the altered radiocapitate articulation cannot withstand massive axial loads.
Phase 4 (3 to 6 months) focuses on return to occupational and recreational activities. Work hardening programs are implemented for manual laborers. It is crucial to manage patient expectations during this phase; regardless of the surgical intervention, patients will likely experience a permanent 20% to 40% reduction in their arc of motion and a 10% to 20% deficit in grip strength compared to the contralateral uninjured wrist. Long-term surveillance with annual radiographs is recommended to monitor for hardware failure or progressive carpal collapse.
Summary of Landmark Literature and Clinical Guidelines
The modern surgical management of lunate fractures and Kienböck disease is built upon a foundation of landmark anatomical and biomechanical studies. Gelberman's seminal microangiographic studies in the 1980s remain the
