Mastering Carpal Fracture Fixation: An Intraoperative Guide to Non-Scaphoid Injuries

Key Takeaway
Welcome to the operating theater, fellows. Today, we're tackling the intricate world of non-scaphoid carpal bone fractures. This masterclass will guide you through precise surgical anatomy, meticulous preoperative planning, and granular, real-time intraoperative execution for fractures of the lunate, triquetrum, pisiform, hamate, capitate, trapezoid, and trapezium, emphasizing reduction, fixation, and complication avoidance.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we delve into the complex, unforgiving, and often underappreciated realm of carpal bone fractures—specifically those excluding the scaphoid. While the scaphoid rightfully commands significant attention due to its high fracture incidence and precarious vascularity, injuries to the remaining carpal bones present unique diagnostic and therapeutic challenges that can humble even the most experienced hand surgeon. These are not simple osseous disruptions; they are catastrophic injuries to the very foundation of hand function. They demand meticulous attention to detail, a profound understanding of carpal biomechanics, and precise, uncompromising surgical execution. Our ultimate objective transcends mere fracture union; we are tasked with the complete restoration of the intricate kinematics of the wrist and hand.
The epidemiology of non-scaphoid carpal fractures reveals a diverse patient demographic, ranging from high-energy polytrauma patients to elite athletes. Fractures of the triquetrum are the second most common carpal fracture after the scaphoid, frequently resulting from a fall on an outstretched hand (FOOSH) causing impingement or avulsion. Conversely, fractures of the hamate, capitate, trapezium, trapezoid, and pisiform are relatively rare, collectively accounting for less than ten percent of all carpal fractures. However, this statistical rarity often breeds clinical complacency. These injuries are notoriously misdiagnosed or missed entirely during initial emergency department evaluations, frequently dismissed as severe wrist sprains until chronic pain and debilitating dysfunction compel further investigation.
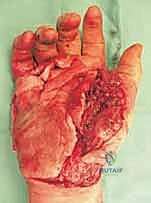
Pathogenetically, these fractures arise from either direct, high-energy focal impacts or indirect, complex rotational forces. Direct trauma frequently manifests as severe crush injuries. When encountering a crushed carpus, the surgeon must maintain an exceptionally high index of suspicion for the development of acute compartment syndrome of the hand. The rigid fascial compartments of the hand are highly intolerant to the edema and hemorrhage associated with direct axial loads. Compressive trauma in the anteroposterior plane can obliterate the normally concave longitudinal and transverse arches of the carpus, resulting in devastating carpal body fractures and axial disruptions. This mechanism frequently produces what is clinically termed the "exploded hand"—a catastrophic constellation of injuries that may include carpometacarpal (CMC) fracture-dislocations, longitudinal metacarpal splits, severe intrinsic muscle contusions, and profound soft tissue degloving.
Indirect trauma, conversely, is characterized by progressive instability patterns driven by extreme rotational and sheer forces. The classic example is the scaphocapitate syndrome, an injury pattern resulting from violent dorsiflexion combined with radial deviation. This mechanism sequentially fractures the scaphoid and then propagates a coronal shear fracture through the capitate neck. In severe iterations, the proximal capitate pole can rotate a full 180 degrees within the midcarpal joint, presenting a profound reconstructive challenge. Understanding these pathomechanical cascades is not merely an academic exercise; it is the fundamental prerequisite for formulating a rational, effective surgical strategy that addresses both the osseous anatomy and the critical stabilizing ligaments.
Detailed Surgical Anatomy and Biomechanics
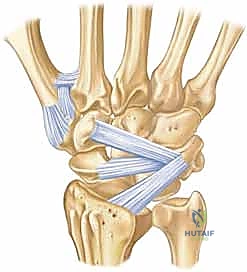
To master carpal fracture fixation, one must first possess an encyclopedic knowledge of carpal anatomy and its dynamic biomechanics. The carpus is an evolutionary marvel of engineering, a complex, intercalated array of eight bones forming two distinct rows, each possessing multiple, highly congruent articular surfaces. The proximal row (scaphoid, lunate, triquetrum) functions as an intercalated segment, lacking any direct tendon insertions. Its movement is entirely dictated by mechanical forces exerted by the surrounding articular contours and the robust intrinsic and extrinsic ligamentous networks. Disruption of any single component within this delicate balance inevitably leads to profound kinematic derangement, asynchronous joint loading, and rapid, progressive cartilaginous degradation.

The capitate, acting as the keystone of the distal carpal row and the primary axis of wrist rotation, warrants specific anatomical focus. It articulates with seven surrounding bones, making its geometric restoration paramount. Crucially, the vascular anatomy of the capitate mirrors the precarious nature of the scaphoid. The predominant blood supply enters the distal half of the bone via palmar vessels and flows retrograde toward the proximal pole (the head). Consequently, a fracture through the capitate neck physically severs this intraosseous vascular network, placing the proximal articular fragment at an exceptionally high risk for avascular necrosis (AVN). This anatomical reality dictates that capitate neck fractures must be treated with the utmost urgency and rigid fixation to optimize the potential for revascularization.

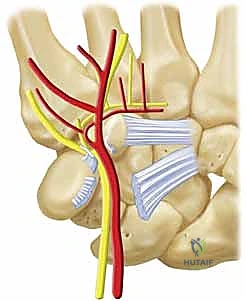
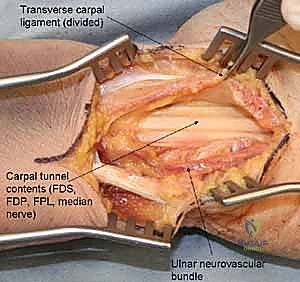
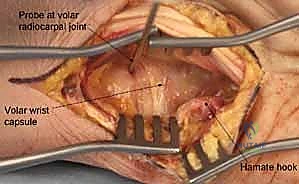
The hamate presents its own unique anatomical complexities, primarily divided into the body and the hook (hamulus). The hamate hook is a slender, volar-projecting osseous prominence that serves as a critical biomechanical pulley for the ulnar flexor tendons of the digits. Furthermore, it acts as the ulnar attachment site for the transverse carpal ligament (forming the roof of the carpal tunnel) and the pisohamate ligament. The hook also forms the radial border of Guyon's canal, intimately associating it with the ulnar nerve and artery. Fractures of the hook, often sustained during racquet sports or golf, not only disrupt this pulley mechanism but also pose a direct mechanical threat to the adjacent ulnar neurovascular bundle, potentially leading to acute neuropathy or vascular thrombosis.
The trapezium and triquetrum similarly possess specialized anatomical features that dictate their fracture patterns and surgical management. The trapezium features a prominent volar ridge, which, akin to the hamate hook, serves as the radial attachment for the transverse carpal ligament. Medial to this ridge lies a deep fibro-osseous groove that houses the flexor carpi radialis (FCR) tendon. Fractures of the trapezial ridge can lead to painful FCR tendinopathy or rupture. The triquetrum, situated on the ulnar aspect of the proximal row, is heavily tethered by the dorsal radiocarpal and dorsal intercarpal ligaments. Extreme wrist flexion and ulnar deviation can cause these robust ligaments to avulse a fragment of the dorsal triquetral cortex, resulting in the most common non-scaphoid carpal fracture. Understanding these specific ligamentous and tendinous associations is critical for interpreting fracture displacement and planning surgical approaches.
Exhaustive Indications and Contraindications
The decision-making process regarding the operative versus non-operative management of non-scaphoid carpal fractures requires a nuanced synthesis of patient factors, fracture morphology, and anticipated functional demands. While isolated, truly non-displaced fractures without associated ligamentous instability may be managed conservatively with rigid immobilization, the threshold for surgical intervention in the modern era of hand surgery is exceedingly low. The overarching philosophy is that the carpus is intolerant of articular incongruity. Even a 1 to 2-millimeter step-off within the highly constrained midcarpal or radiocarpal joints significantly alters contact stresses, inevitably precipitating early, severe post-traumatic osteoarthritis. Therefore, any fracture demonstrating articular displacement, rotational malalignment, or structural destabilization of the carpal arch is an absolute indication for operative reduction and internal fixation.
Specific fracture patterns inherently carry a higher mandate for surgical intervention due to their biological and biomechanical behavior. As previously discussed, capitate neck fractures, given their high propensity for avascular necrosis and nonunion, generally warrant acute surgical stabilization to optimize the biological environment for healing. Similarly, displaced fractures of the hamate body that disrupt the fourth and fifth carpometacarpal joints require rigid fixation to restore grip strength and prevent painful subluxation. Open carpal fractures, regardless of displacement, represent absolute surgical emergencies necessitating immediate, aggressive debridement, copious irrigation, and stabilization to mitigate the devastating risk of deep space infection and osteomyelitis. Furthermore, any carpal fracture associated with acute, progressive neurovascular compromise—such as ulnar nerve compression secondary to a displaced hamate hook fracture—demands urgent surgical decompression and fracture management.
Conversely, contraindications to surgical intervention, while rare, must be carefully considered to avoid inflicting iatrogenic harm. Absolute contraindications include active, uncontrolled local soft tissue infections (unless the surgery is specifically for source control and debridement) and severe, systemic medical comorbidities that render the patient unfit for anesthesia. Relative contraindications revolve primarily around the status of the soft tissue envelope. In cases of severe crush injuries with massive soft tissue loss, immediate internal fixation may be contraindicated if adequate soft tissue coverage cannot be achieved. In such scenarios, damage control orthopedics—utilizing external fixation or temporary Kirschner wire stabilization—must be employed until the soft tissue bed is optimized for definitive internal fixation.

Below is a comprehensive table outlining the specific indications and contraindications for the operative management of non-scaphoid carpal fractures.
| Category | Specific Criteria / Condition | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Open Fractures | High risk of osteomyelitis; requires emergent I&D and stabilization. |
| Articular Step-off > 1-2mm | Prevents rapid onset of post-traumatic midcarpal/radiocarpal arthritis. | |
| Associated Carpal Instability | Perilunate fracture-dislocations require restoration of carpal kinematics. | |
| Neurovascular Compromise | E.g., Ulnar nerve compression from hamate hook fracture; requires decompression. | |
| "Exploded Hand" Polytrauma | Requires global restoration of skeletal architecture for functional salvage. | |
| Relative Indications | Capitate Neck Fractures | High risk of AVN; rigid fixation optimizes revascularization potential. |
| Hamate Hook Nonunion | Excision or fixation indicated for chronic pain, grip weakness, or flexor tendon fraying. | |
| Trapezial Ridge Fractures | High rate of symptomatic nonunion with conservative management. | |
| Displaced Triquetral Body | Operative fixation preferred to restore proximal row integrity. | |
| Absolute Contraindications | Active Local Infection | Hardware placement in infected field guarantees chronic osteomyelitis. |
| Medically Unstable Patient | Anesthetic risk outweighs the benefit of acute fracture fixation. | |
| Relative Contraindications | Severe Soft Tissue Degloving | Lack of coverage for hardware; may require temporary spanning external fixation. |
| Advanced Pre-existing Arthritis | Primary fusion or proximal row carpectomy may be preferable to ORIF. | |
| Severely Osteopenic Bone | Inability to achieve adequate screw purchase; may necessitate K-wire or cast management. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the crucible in which successful surgical outcomes are forged. This process begins with an exhaustive patient history, focusing intensely on the exact mechanism of injury. A high-energy axial load, a severe crush mechanism, or a specific athletic maneuver (such as a checked swing in baseball causing a hamate hook fracture) immediately guides the diagnostic algorithm. The physical examination must be meticulous and systematic. When assessing localized pain, the surgeon should deliberately begin palpation away from the suspected injury site, progressively moving toward the epicenter to avoid masking subtle, concomitant injuries. Tactile landmarks are invaluable; for instance, to identify the hamate hook pre-incision, the surgeon can place the interphalangeal joint of their thumb on the patient's pisiform and flex the thumb toward the first web space—the thumb tip will predictably land directly on the hamate hook.

A comprehensive neurovascular assessment is absolutely non-negotiable. Severe crush injuries or high-energy trauma can rapidly evolve into compartment syndrome. Fractures of the pisiform or hamate hook place the ulnar nerve at extreme risk within Guyon's canal. The surgeon must perform a detailed evaluation of the median, radial, ulnar, and digital nerves, documenting two-point discrimination and motor function. Vascular status is assessed via capillary refill, skin color, temperature, and Allen's testing, utilizing handheld Doppler ultrasonography if any ambiguity exists. Furthermore, the concept of the "exploded hand" dictates that observation must extend beyond the immediate zone of injury. A global examination of the entire hand, forearm, and elbow is mandatory to identify occult fracture-dislocations or longitudinal metacarpal splits that frequently accompany severe carpal trauma.
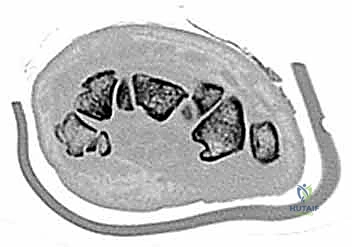
Imaging is the cornerstone of preoperative templating. Routine evaluation begins with high-quality posteroanterior, lateral, and oblique radiographs of the wrist. However, standard views are notoriously inadequate for isolating specific carpal pathology due to osseous overlap. Special radiographic projections are therefore essential. The carpal tunnel view is critical for evaluating the hamate hook and the trapezial ridge. The "papillon view"—a supinated oblique lateral projection with the wrist in radial deviation and the thumb abducted—is highly specific for profiling the hamate hook. Similarly, a 45-degree supinated lateral view optimally visualizes the pisotriquetral articulation.
Despite optimal plain radiography, advanced imaging is frequently required. High-resolution computed tomography (CT) scanning with fine axial, coronal, and sagittal reconstructions has become the gold standard and the imaging modality of choice for complex carpal trauma. CT scans definitively confirm occult fractures, delineate intra-articular comminution, and reveal subtle associated injuries missed on plain films. They allow the surgeon to mentally construct a 3D model of the fracture, facilitating precise preoperative templating of screw trajectories and implant sizes. If dynamic instability is suspected but unconfirmed, an Examination Under Anesthesia (EUA) combined with real-time fluoroscopy (utilizing stress and distraction views) is performed immediately prior to the definitive procedure to finalize the surgical blueprint.

Patient positioning and anesthesia setup must be optimized for surgical efficiency and patient safety. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. Anesthesia is typically achieved via a regional block (e.g., ultrasound-guided axillary or supraclavicular brachial plexus block), which provides excellent intraoperative operating conditions and profound, long-lasting postoperative analgesia. General anesthesia is reserved for polytrauma patients or those with contraindications to regional techniques. A well-padded pneumatic tourniquet is applied to the proximal arm. Prior to inflation, the limb is meticulously exsanguinated using an Esmarch bandage to ensure a bloodless surgical field, which is absolutely critical for identifying delicate carpal anatomy and tiny articular fragments. The fluoroscopy unit (C-arm) is positioned opposite the surgeon, perpendicular to the hand table, allowing for unhindered, dynamic imaging throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Management of Capitate Fractures
The surgical approach to the capitate is predominantly dorsal, given its central location and the risk of injury to palmar vascular structures. A longitudinal dorsal incision is centered over the third metacarpal base, extending proximally towards Lister's tubercle. The extensor retinaculum is incised, typically developing an interval between the third (extensor pollicis longus) and fourth (extensor digitorum communis) extensor compartments. The tendons are carefully retracted, and the posterior interosseous nerve (PIN) is identified and protected, or prophylactically neurectomized to denervate the dorsal capsule and reduce postoperative pain. A ligament-sparing dorsal capsulotomy—often a ligament-splitting or a flap-based approach preserving the dorsal intercarpal and radiocarpal ligaments—is performed to expose the midcarpal joint.
Once exposed, the fracture hematoma is meticulously debrided. In the setting of a scaphocapitate syndrome, the surgeon may encounter the daunting scenario of a capitate head that has rotated 180 degrees. Reduction requires delicate manipulation, often utilizing a dental pick or a small periosteal elevator as a joystick, combined with longitudinal traction. Extreme care must be taken to avoid further stripping of the tenuous palmar soft tissue attachments, which harbor the critical remaining blood supply. Once anatomic reduction is achieved, provisional fixation is secured with multiple 0.045-inch Kirschner wires.
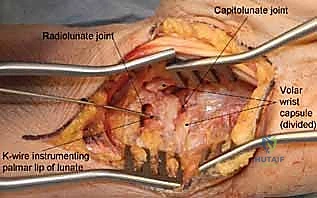
Definitive fixation is optimally achieved using headless compression screws. For capitate neck fractures, an antegrade trajectory (from the dorsal proximal pole directed distally into the body) or a retrograde trajectory (from the dorsal body directed proximally into the head) can be utilized, depending on fracture morphology and fragment size. The screw must be entirely buried beneath the articular cartilage to prevent devastating midcarpal impingement. Intraoperative fluoroscopy is utilized continuously to confirm anatomic reduction, verify screw length, and ensure no hardware penetrates the articular surfaces. If comminution is severe, supplemental K-wire fixation or even a miniature dorsal spanning plate may be required.
Hamate Hook Excision and Open Reduction Internal Fixation
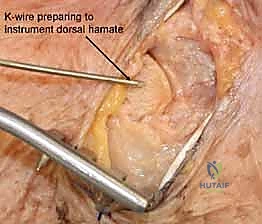
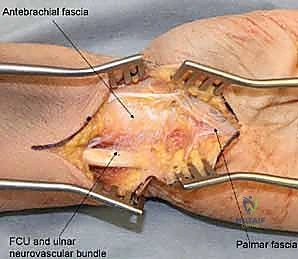
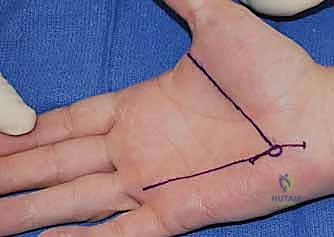
Surgical intervention for the hamate hook is dictated by the chronicity of the injury and the size of the fracture fragment. For acute, large-fragment fractures at the base of the hook, Open Reduction and Internal Fixation (ORIF) is preferred to restore the biomechanical pulley of the flexor tendons. A volar approach is utilized, initiating the incision along the proximal thenar crease and extending it proximally across the wrist flexion creases in a zig-zag fashion to prevent scar contracture. The superficial palmar fascia is incised, and Guyon's canal is systematically explored. The ulnar nerve and artery are meticulously identified, mobilized, and protected with vessel loops throughout the procedure.
For ORIF, the fracture site is exposed by carefully elevating the hypothenar musculature originating from the hook. The fracture is reduced and provisionally held with a K-wire. A cannulated headless compression screw (typically 2.0mm or 2.4mm) is then advanced over a guidewire from the tip of the hook down into the body of the hamate. Fluoroscopy is critical to ensure the screw does not penetrate the articular surface of the hamate body or impinge upon the CMC joints.

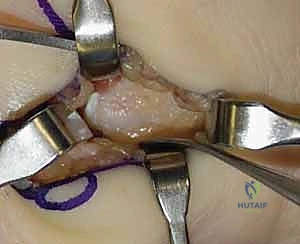
More commonly, surgeons encounter symptomatic nonunions of the hamate hook. In these chronic cases, excision of the ununited fragment is the gold standard, offering reliable pain relief and a rapid return to function without significant biomechanical compromise. Utilizing the same volar approach, the ununited hook fragment is identified. Dissection must stay strictly subperiosteal on the hook to avoid injury to the deep motor branch of the ulnar nerve, which curves intimately around its base. The transverse carpal ligament and the pisohamate ligament are sharply detached from the fragment. The fragment is then excised, and the remaining base on the hamate body is smoothed with a rongeur or a high-speed burr to prevent future flexor tendon fraying or rupture.
Triquetrum and Trapezium Management Strategies
Triquetral body fractures, while less common than dorsal avulsions, demand rigid fixation when displaced to restore the integrity of the proximal row. A dorsal longitudinal approach is utilized, entering between the fourth and fifth extensor compartments. The dorsal radioulnar and radiocarpal ligaments are incised to expose the triquetrum. Following reduction, fixation is typically achieved with small headless compression screws or multiple K-wires. Conversely, the ubiquitous dorsal triquetral avulsion fractures are almost universally managed non-operatively with a short period of immobilization. Surgical excision of the avulsed fragment is reserved strictly for cases of recalcitrant, chronic dorsal ulnar-sided wrist pain that fails months of conservative therapy.

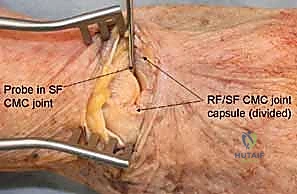
Trapezial fractures are divided into ridge and body fractures, each requiring a distinct approach. Trapezial ridge fractures, analogous to hamate hook fractures, are approached volarly. The incision is made over the FCR tendon, which is carefully retracted. The fracture is exposed, and depending on fragment size, it is either excised (if small and comminuted) or fixed with a mini-fragment screw (if a large, acute basal fragment). Trapezial body fractures, particularly those involving the highly mobile thumb CMC joint, require precise anatomic reduction to prevent early, debilitating arthritis. A dorsal-radial approach is employed, centered over the CMC joint. The radial artery must be identified and protected within the anatomic snuffbox. Fixation is achieved using 1.5mm or 2.0
Clinical & Radiographic Imaging Archive