Comprehensive Surgical Guide to DRUJ Arthroscopy and Scaphoid Fracture Management
Key Takeaway
The distal radioulnar joint (DRUJ) and scaphoid present complex biomechanical challenges in hand surgery. This guide details the precise arthroscopic evaluation of the DRUJ, emphasizing safe portal placement to protect the ulnar nerve. Furthermore, it provides an evidence-based approach to scaphoid fractures, covering precarious vascular anatomy, advanced MRI diagnostics, and precise surgical fixation techniques required to prevent nonunion and osteonecrosis in displaced or unstable fracture patterns.
ARTHROSCOPIC EXAMINATION OF THE DISTAL RADIOULNAR JOINT (DRUJ)
The distal radioulnar joint (DRUJ) is a highly complex articulation essential for forearm pronation and supination. Arthroscopic evaluation of the DRUJ has evolved into a critical diagnostic and therapeutic tool for managing ulnar-sided wrist pain, triangular fibrocartilage complex (TFCC) tears, chondral lesions, and subtle instability. Mastery of DRUJ arthroscopy requires a profound understanding of ulnar-sided neurovascular anatomy and precise portal placement.
Patient Positioning and Joint Distension
Proper setup is paramount for safe entry into the DRUJ. The patient is positioned supine with the arm suspended in a traction tower using finger traps (typically on the index and middle fingers) with 10 to 15 pounds of longitudinal traction.
To safely establish portals, the joint must first be adequately distended:
* Position the forearm in supination to best palpate the distal radioulnar interval.
* Insert an 18- or 20-gauge needle into the joint just lateral and dorsal to the ulnar head.
* Inject a small amount of normal saline (typically 2 to 3 mL) to distend the capsule. This step pushes the capsule away from the articular surfaces, minimizing the risk of iatrogenic chondral injury during trocar insertion.
Establishing the Portals
Proximal and distal radioulnar portals, originally described by Whipple, are the standard approaches for DRUJ arthroscopy.
Surgical Pearl: The proximal portal is universally considered safer than the distal portal. It presents significantly less risk to the articular cartilage of the ulnar head and the proximal surface of the triangular fibrocartilage.
Step-by-Step Proximal Portal Placement:
1. Incision: Incise the dorsal skin just proximal to the dorsal prominence of the ulnar head. The incision should be centered precisely between the distal ulna and the medial (ulnar) aspect of the radius.
2. Blunt Dissection: Use a small hemostat to bluntly dissect down to the joint capsule.
* Critical Warning: Sharp dissection must be strictly avoided to prevent catastrophic injury to the extensor carpi ulnaris (ECU) tendon and the dorsal sensory branch of the ulnar nerve (DSBUN), which courses in close proximity to this region.
3. Capsular Entry: Enter the joint capsule bluntly with the hemostat to create a tract.
4. Cannula Insertion: Pass the arthroscopic cannula, equipped with a blunt obturator, from proximal to distal. The trajectory should follow the natural inclination of the joint.
5. Verification: Remove the obturator and insert the arthroscope (typically a 2.7-mm or 1.9-mm 30-degree scope) to confirm intra-articular placement and begin the diagnostic sweep.
Establishing the Working Portal:
A working portal is essential for instrumentation, such as the introduction of probes, forceps, and motorized shavers.
* Locate a site 5 to 10 mm distal to the proximal radioulnar portal.
* Make a small skin incision and bluntly dissect the subcutaneous tissues.
* Pass an 18-gauge needle into the joint under direct intra-articular arthroscopic visualization to confirm the optimal trajectory.
* Once confirmed, dilate the tract and insert the working cannula.
The DRUJ Portal (Distal Approach):
To establish the specific DRUJ portal, make an incision over the interval between the fifth (extensor digiti minimi) and sixth (ECU) extensor compartments. Dissect bluntly to enter the joint just proximal to the triangular fibrocartilage, navigating between the fibrocartilage and the ulnar head. While useful, remember that the proximal portal remains superior for the safe inspection of the lesser sigmoid notch, the ulnar head, and the proximal surface of the TFCC.
Postoperative Care and Rehabilitation
Following a thorough arthroscopic examination and any necessary debridement or repair, remove all instruments and cannulas. The wounds are typically closed with simple non-absorbable sutures, followed by the application of a compressive dressing and a supportive volar splint.
Postoperative protocols are dictated by the specific pathology addressed:
* Diagnostic/Debridement: The splint is removed, and active mobilization is initiated within the first 7 to 10 days.
* Ligamentous/TFCC Repairs: Immobilization in a long-arm or Muenster cast/splint may be prolonged (4 to 6 weeks), followed by a structured, phased rehabilitation program to restore pronosupination and grip strength.
THE SCAPHOID: ANATOMY, KINEMATICS, AND VASCULARITY
The scaphoid is the critical kinematic link between the proximal and distal carpal rows. It articulates with the radius proximally and with four of the remaining seven carpal bones. Because it bridges the carpal rows, the scaphoid moves with nearly all carpal motions, particularly volar flexion. Any alteration of its articular surface—whether through fracture, dislocation, or subluxation—or any compromise of its stability via ligamentous rupture, inevitably causes severe secondary degenerative changes throughout the entire carpus (e.g., Scaphoid Nonunion Advanced Collapse [SNAC]).
Biomechanics of the Proximal Carpal Articulation
Understanding the load-carrying structures of the wrist is essential for grasping why scaphoid fractures are so prone to displacement. Weber and Chao described the complex force transmission across the radiocarpal joint.


As illustrated in the biomechanical models above, four primary ligamentous components potentially transmit tensile loads when the wrist is in strong dorsiflexion:
1. Radiocollateral ligament complex
2. Radiocapitate ligament
3. Radiolunate ligament
4. Ulnar capsular ligament
During dorsiflexion, dorsal ligamentous structures become lax and are eliminated from load-bearing analysis. The articular surfaces between the radius and scaphoid, and between the radius and lunate, transmit massive compressive forces. These forces are related to a fixed coordinate system and the vector representation of the applied load. The scaphoid, acting as a strut, absorbs a disproportionate amount of this compressive and shear force, explaining its high fracture incidence during falls on an outstretched hand (FOOSH).
The Precarious Blood Supply of the Scaphoid
The vascular anatomy of the scaphoid is notoriously precarious and is the primary determinant of fracture healing and the high incidence of osteonecrosis (avascular necrosis).
Vessels enter the scaphoid from the radial artery via three main routes: laterovolarly, dorsally, and distally. The laterovolar and dorsal systems share the responsibility of supplying the proximal two-thirds of the bone.
Anatomical Fact: Vascularity of the proximal pole and 70% to 80% of the intraosseous circulation are provided through branches of the radial artery entering through the dorsal ridge. These vessels flow in a retrograde fashion. In the distal tuberosity region, 20% to 30% of the bone receives its blood supply from volar branches of the radial artery.
Vascular Distribution Statistics:
* 67% of scaphoid bones have arterial foramina throughout their entire length (distal, middle, and proximal thirds).
* 20% have most of their arterial foramina concentrated in the waist area, with no more than a single foramen near the proximal third.
* 13% have a blood supply predominantly restricted to the distal third.
Consequently, one-third of all scaphoid fractures occurring in the proximal third may be completely devoid of an adequate blood supply. Clinically, this translates to an osteonecrosis prevalence of up to 35% in proximal pole fractures. Fractures in this region take significantly longer to heal and exhibit the highest rates of nonunion.



As demonstrated in the clinical data above, the union of the scaphoid after fracture or bone grafting is influenced significantly by both the anatomical location of the fracture (proximal vs. waist vs. distal) and the amount of initial displacement.
DIAGNOSIS AND ADVANCED IMAGING OF SCAPHOID FRACTURES
A high index of suspicion is required when evaluating patients with radial-sided wrist pain following trauma. While standard radiographs (including scaphoid views with the wrist slightly extended in ulnar deviation) are the first line of diagnosis, non-displaced fractures are frequently occult on initial plain films.
Historically, the standard of care for a suspected occult scaphoid fracture was immobilization in a cast for 2 weeks followed by repeat radiography. However, modern advanced imaging provides definitive diagnostic information much sooner, preventing unnecessary immobilization and allowing for early surgical intervention when indicated.
Magnetic Resonance Imaging (MRI) and Computed Tomography (CT)
MRI is currently the gold standard for detecting occult scaphoid fractures. Gaebler et al. reported 100% sensitivity and specificity using MRI to diagnose occult scaphoid fractures at an average of merely 2.8 days post-injury.
Furthermore, MRI—especially with gadolinium enhancement—is invaluable in assessing the vascular status of the proximal pole in established fractures or nonunions.
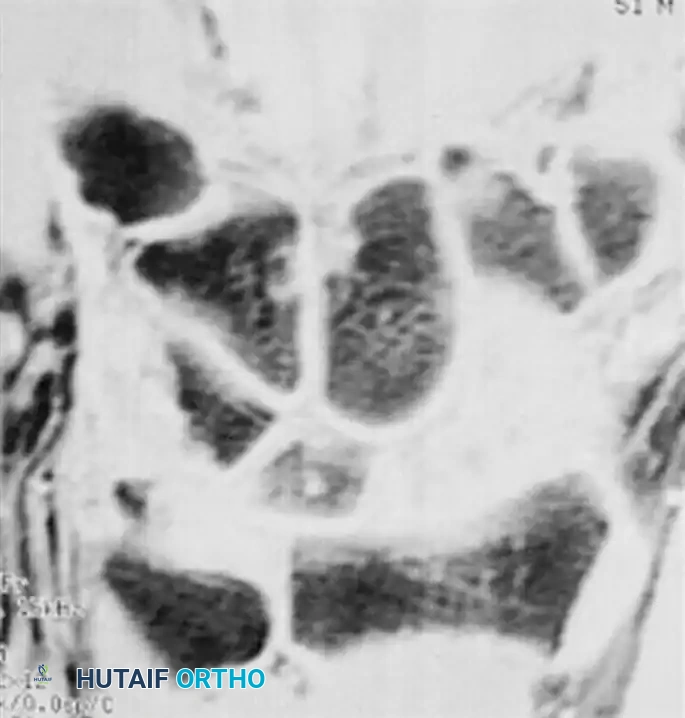

(A) MRI demonstrating an acute, occult scaphoid waist fracture not visible on plain radiographs. (B) Gadolinium-enhanced MRI evaluating the vascularity of the proximal pole, critical for surgical planning.
While MRI is superior for detecting edema and vascularity, Computed Tomography (CT) scans reconstructed in the sagittal and coronal planes of the scaphoid are the imaging modality of choice for assessing fracture displacement, angulation (humpback deformity), and progression of union.
MANAGEMENT OF SCAPHOID FRACTURES
The treatment algorithm for scaphoid fractures is dictated by fracture location, degree of displacement, carpal stability, and patient-specific factors (e.g., athletic demands, occupation).
Nonoperative Management
Acute, strictly non-displaced fractures of the scaphoid waist and distal pole can be managed nonoperatively with a high expectation of success.
Casting Technique:
* Apply a well-molded short-arm thumb spica cast.
* The cast should extend from just below the elbow proximally to the base of the thumbnail and the proximal palmar crease distally.
* Position the wrist in slight radial deviation and neutral flexion.
* The thumb must be maintained in a functional position, leaving the interphalangeal joint and the fingers free to move from the metacarpophalangeal joints distally to prevent stiffness.
Using strict nonoperative casting techniques, the expected rate of union is 90% to 95% within 10 to 12 weeks. During this period, the fracture must be monitored radiographically. In experimental models, displacement of more than 3 mm between fracture fragments can occur during pronation and supination even within a short-arm cast. If collapse, angulation, or displacement occurs during conservative treatment, surgical intervention is mandated.
Operative Management: Displaced and Unstable Fractures
A displaced or unstable scaphoid fracture requires a completely different treatment paradigm. Nonoperative management of these injuries leads to unacceptably high rates of nonunion, malunion, and subsequent carpal collapse.
Radiographic Criteria for Instability and Displacement:
Surgical fixation is indicated if any of the following criteria are met:
* Fracture fragment offset greater than 1 mm on any radiographic view (AP, lateral, or oblique).
* Lunocapitate angulation greater than 15 degrees.
* Scapholunate angulation greater than 45 degrees (normal range is 30 to 60 degrees; comparison views of the contralateral wrist are highly recommended).
* Lateral intrascaphoid angle greater than 45 degrees.
* Anteroposterior intrascaphoid angle less than 35 degrees (Amadio et al.).
* Height-to-length ratio of 0.65 or greater (Bain et al.).
Initial Reduction:
Reduction can initially be attempted via closed means using longitudinal traction and slight radial compression of the carpus. If closed reduction is anatomically successful, percutaneous fixation with a cannulated screw or Kirschner wires, followed by a long-arm thumb spica cast, may suffice. If closed reduction fails, open reduction and internal fixation (ORIF) is required.
Surgical Techniques and Fixation Devices
The optimal method of internal fixation depends on the fracture pattern, the presence of comminution, and the surgeon’s expertise. While Kirschner wires can provide adequate fixation in select cases, headless compression screws are the modern gold standard.
Screw Fixation Biomechanics:
Various headless screws are utilized, including the AO cannulated screw, the Herbert differential pitch bone screw, the Herbert-Whipple screw, and the Acutrak fully threaded tapered screw.
* In cadaveric biomechanical studies, the AO screw, Acutrak screw, and Herbert-Whipple screw demonstrated superior resistance to cyclical bending loads compared to the traditional non-cannulated Herbert screw.
* In clinical comparison studies between AO cannulated screws and Herbert-Whipple screws, union rates approached 100% in both cohorts for appropriately selected fractures.
Advantages of Headless Cannulated Screws:
1. Accuracy: The cannulated design allows the screw to be placed precisely over a guide pin under continuous video fluoroscopic control.
2. Compression: Differential pitch or tapered designs generate robust compression directly across the fracture site.
3. Early Mobilization: Rigid internal fixation significantly reduces the required time for external immobilization.
4. No Hardware Prominence: Because the headless screw is buried beneath the articular cartilage, routine hardware removal is unnecessary.
Surgical Pitfall: Contraindications to standard screw fixation include avascular fragmentation of the proximal pole, extensive osteoarthritis involving adjacent carpals or the radial articular surface, and gross carpal collapse. In these scenarios, salvage procedures (e.g., proximal row carpectomy, partial wrist fusion) may be indicated.
Percutaneous vs. Open Fixation
Because prolonged immobilization can lead to joint stiffness, muscle atrophy, and significant socioeconomic downtime, operative intervention is increasingly considered even for non-displaced fractures in high-demand patients (e.g., elite athletes, manual laborers).
Percutaneous Fixation:
Prospective, randomized studies comparing percutaneous screw fixation with cast immobilization for non-displaced waist fractures have shown that surgically treated patients regain range of motion and return to work/sports significantly earlier.
* In one landmark study of 88 patients with non-displaced waist fractures, the 44 patients treated with percutaneous Herbert screw fixation (without postoperative casting) experienced zero nonunions. Conversely, the 44 patients treated with cast immobilization had 10 nonunions at 12 weeks.
* "Limited access," percutaneous, and arthroscopically assisted percutaneous techniques minimize iatrogenic trauma to the volar radiocarpal ligaments and preserve the delicate dorsal blood supply.
Despite these advantages, patients must be thoroughly counseled. Acute, non-displaced scaphoid fractures have a very high probability of healing with simple cast treatment. Percutaneous fixation is a technically demanding procedure with potential complications, including guide wire breakage, articular cartilage damage, and iatrogenic fracture displacement. Preoperative planning, meticulous attention to detail, and precise fluoroscopic imaging are absolute prerequisites for success.
You Might Also Like

