Open Reduction and Internal Fixation of Femoral Neck Fractures: A Master Surgical Guide

Key Takeaway
Open reduction and internal fixation (ORIF) of femoral neck fractures is indicated when closed reduction fails or in young patients requiring anatomic restoration. Utilizing a modified Smith-Petersen approach allows direct visualization of the fracture. Fixation constructs, including cannulated screws, compression hip screws, or proximal femoral locking plates, are selected based on fracture geometry and comminution. Achieving anatomic reduction and length-stable fixation is paramount to minimizing complications such as osteonecrosis and nonunion.
INTRODUCTION TO FEMORAL NECK ORIF
The management of displaced intracapsular femoral neck fractures, particularly in the young, physiologically active patient, remains one of the most formidable challenges in orthopedic trauma. Unlike intertrochanteric fractures, which occur in highly vascularized cancellous bone, femoral neck fractures jeopardize the tenuous retrograde blood supply to the femoral head, primarily derived from the medial circumflex femoral artery (MCFA).
Open Reduction and Internal Fixation (ORIF) is strictly indicated when an anatomic closed reduction cannot be achieved, or in the setting of high-energy trauma in young adults where precise, direct visualization is mandatory to restore the biomechanical integrity of the hip joint. An inadequate closed reduction must never be accepted. In elderly, low-demand patients with displaced fractures, arthroplasty is generally preferred; however, in the young patient, joint preservation through meticulous ORIF is the gold standard.
🚨 Surgical Warning
The tolerance for malreduction in young femoral neck fractures is zero. Failure to achieve an anatomic reduction significantly increases the risk of nonunion, osteonecrosis (AVN), and catastrophic implant failure. If closed reduction is not perfect, immediately transition to an open approach.
PREOPERATIVE PLANNING AND BIOMECHANICS
Fracture Geometry and the Pauwels Classification
The biomechanical environment of the femoral neck is dictated by the orientation of the fracture line. The Pauwels classification remains highly relevant for preoperative planning:
* Pauwels Type I (< 30 degrees): Compressive forces predominate. These are inherently more stable and often amenable to parallel cannulated screw fixation.
* Pauwels Type II (30–50 degrees): Mixed shear and compressive forces.
* Pauwels Type III (> 50 degrees): High shear forces predominate. These vertical fracture patterns are highly unstable. Biomechanical data unequivocally demonstrate that parallel cannulated screws are insufficient for Pauwels III fractures. A fixed-angle device, such as a Compression Hip Screw (CHS) with a derotational screw, or a Proximal Femoral Locking Plate (PFLP), is required to resist vertical shear.
Assessing Comminution
Preoperative advanced imaging (CT scanning) is highly recommended to assess the degree of posterior comminution. Significant posterior comminution compromises the buttress effect of the femoral neck, leading to retroversion and shortening if not adequately stabilized.
Axial CT scan demonstrating a femoral neck fracture with significant posterior femoral neck comminution. This structural deficit necessitates length-stable fixation constructs.
PATIENT POSITIONING AND SETUP
Optimal positioning is critical for both surgical access and high-quality intraoperative fluoroscopy.
- Table Selection: Position the patient supine on either a flat-topped radiolucent table or a dedicated fracture table. A fracture table often facilitates easier and more reproducible lateral fluoroscopy, while a flat table allows for greater freedom in manipulating the limb during open reduction.
- Fluoroscopy: Position the C-arm to allow unimpeded anteroposterior (AP) and cross-table lateral views of the proximal femur. Confirm that true AP and lateral images can be obtained before prepping and draping.
- Preparation: The entire hemipelvis, hip, and lower extremity should be prepped and draped free to allow for dynamic manipulation if a flat table is utilized.
SURGICAL APPROACH: THE MODIFIED SMITH-PETERSEN
While a Watson-Jones (anterolateral) approach can be used, subcapital and transcervical femoral neck fractures are best visualized and most easily reduced through a Modified Smith-Petersen (Anterior) Approach. This utilizes the true internervous plane between the femoral nerve (Sartorius/Rectus Femoris) and the superior gluteal nerve (Tensor Fasciae Latae).
Step-by-Step Dissection
- Incision: Make a longitudinal incision beginning at the anterior superior iliac spine (ASIS) and extending approximately 10 cm distally toward the lateral aspect of the patella.
- Superficial Dissection: Incise the fascia of the tensor fasciae latae (TFL) in line with the skin incision. Develop the interval between the TFL laterally and the sartorius muscle medially.
- Vascular Control: As you deepen the interval, you will encounter the ascending branches of the lateral femoral circumflex artery. These vessels cross the surgical field transversely and must be meticulously isolated, clamped, and cauterized or ligated to prevent postoperative hematoma.
- Deep Dissection: Identify and tag the direct head of the rectus femoris. Release it from its origin on the anterior inferior iliac spine (AIIS).
- Capsular Exposure: Reflect the indirect head of the rectus femoris muscle from the anterior hip capsule, along with the iliocapsularis muscle if present. Retract the iliopsoas medially to expose the entire anterior capsule.
💡 Clinical Pearl
The modified Smith-Petersen approach provides unparalleled direct visualization of the anterior femoral neck, making it the approach of choice for anatomic reduction. However, it requires a separate, small lateral incision for the insertion of the fixation hardware (screws or side-plate).
Capsulotomy and Joint Decompression
Perform a formal capsulotomy to expose the fracture and evacuate the fracture hematoma.
* Shape: The capsulotomy can be made in the shape of a T, an inverted-T, or an H. A T-shaped capsulotomy is most frequently utilized.
* Vascular Preservation: The vascular anatomy of the proximal femur must dictate the extent of the capsulotomy. If an inverted-T or H-shaped capsulotomy is chosen, strictly avoid posterior extension of the transverse limb at the base of the femoral neck. The retinacular vessels, branches of the MCFA, run along the posterior-superior neck. Iatrogenic injury to these vessels will guarantee avascular necrosis of the femoral head.
FRACTURE REDUCTION TECHNIQUES
Direct visualization allows for precise manipulation of the fracture fragments. The goal is absolute anatomic reduction.
- Distal Control: Place a 5.0-mm Schanz pin into the proximal femoral diaphysis (distal to the fracture). Attach a T-handle to this pin. This provides a powerful lever to control rotation, translation, and traction of the distal femoral segment.
- Proximal Control (Joysticks): Insert two 2.0-mm threaded Kirschner wires (K-wires) into the femoral head segment. These act as "joysticks" to manipulate the proximal fragment out of varus and retroversion.
- Direct Manipulation: Using Cobb elevators, ball-spike pushers, and the placed joysticks, anatomically align the cortical edges of the anterior femoral neck.
- Compression: Once aligned, a reduction clamp (such as a Farabeuf clamp) can be applied to gain compression across the fracture site prior to definitive fixation.
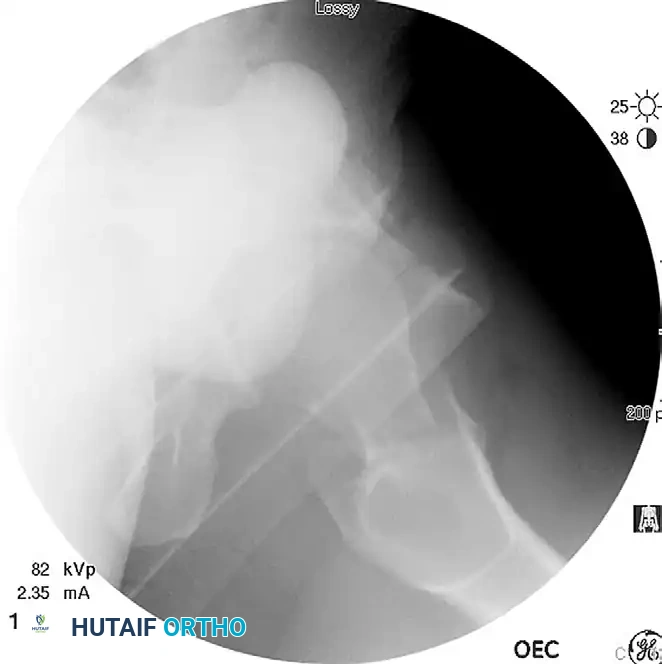
Displaced femoral neck fracture visualized prior to reduction.
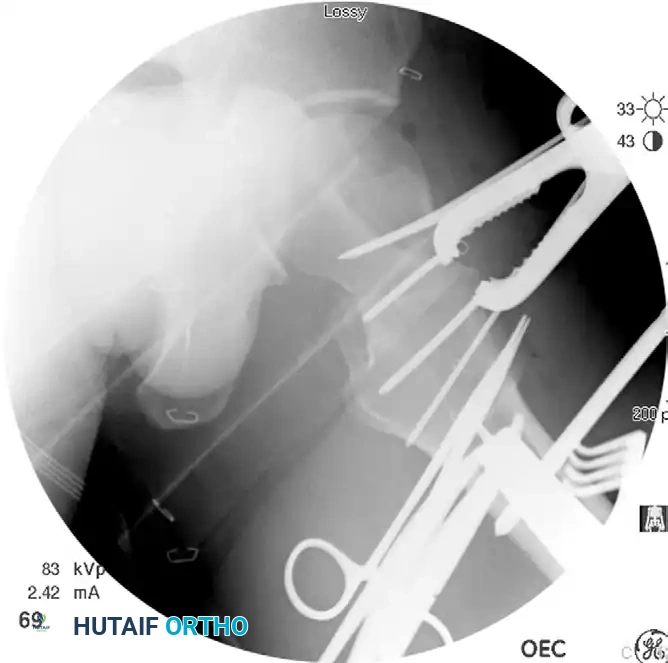
Anatomic reduction achieved. A Farabeuf reduction clamp is utilized to gain and maintain compression across the femoral neck fracture prior to hardware placement.
Confirm the reduction visually through the anterior approach and radiographically via AP and lateral fluoroscopy. The reduction must be perfect before proceeding to fixation.
INTERNAL FIXATION STRATEGIES
The choice of implant depends heavily on the fracture pattern (Pauwels angle), bone quality, and degree of comminution.
1. Cannulated Screw Fixation
Indicated primarily for stable, low-shear fracture patterns (Pauwels I and II) without significant comminution.
- Technique: Through a separate lateral stab incision, insert three partially threaded cannulated screws in an inverted triangle configuration. The inferior screw should rest on the calcar, and the posterior screw should sit adjacent to the posterior cortex to maximize biomechanical stability.
- Washers: Washers must be used whenever possible, particularly in osteopenic bone, as their use has been shown to significantly reduce the risk of screw head punch-out and construct failure.
- Length Maintenance: To prevent shortening, partially threaded screws can be used initially to compress the fracture. Once compressed, they can be sequentially exchanged for fully threaded screws to create a length-stable construct.

Cannulated screw fixation of a displaced femoral neck fracture following successful open reduction.
2. Compression Hip Screw (CHS) with Derotational Screw
Indicated for highly unstable, vertical shear patterns (Pauwels III) or basicervical fractures. Biomechanical studies confirm that a CHS coupled with a derotational screw is significantly stronger than three parallel cannulated screws in resisting vertical shear forces.
- Technique: Place a guide pin perpendicular to the fracture line. Insert a partially threaded cannulated screw superiorly to act as a derotational screw and to provide initial compression.
- Lag Screw Placement: Insert the CHS guide wire centrally into the femoral head. Ream and insert the large-diameter lag screw. In young patients with dense, non-osteoporotic bone, routine tapping is highly recommended to prevent iatrogenic displacement or distraction of the fracture during screw insertion.
- Plate Application: Slide the side plate over the lag screw and secure it to the femoral shaft.

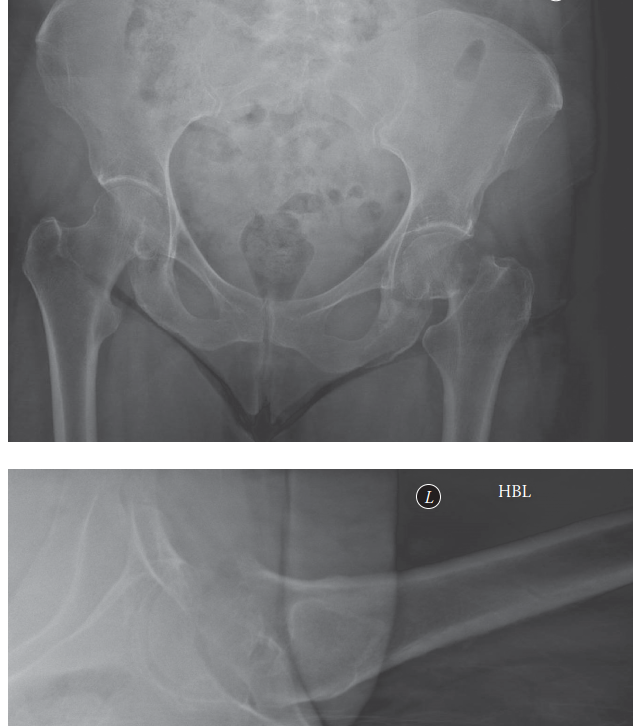
Displaced femoral neck fracture, in this case ipsilateral to a femoral shaft fracture, requiring robust fixed-angle fixation.

The same fracture fixed rigidly with a compression hip screw (CHS) and a superior derotational screw to resist shear and rotational forces.
3. Proximal Femoral Locking Plate (PFLP)
Indicated for fractures with severe femoral neck comminution where length-stable fixation is paramount.
Recent biomechanical data suggest that a PFLP may be superior to both cannulated screws and a CHS in a Pauwels type III model with comminution. The locking construct acts as an internal fixator, preventing the femoral neck from collapsing into varus and retroversion.

Anteroposterior (AP) radiograph at union of a displaced femoral neck fracture with significant comminution, treated successfully with a proximal femoral locking plate.

Lateral radiograph of the same patient, demonstrating maintenance of alignment and length via the fixed-angle locking construct.
💡 Clinical Pearl: The Importance of Femoral Neck Length
Maintaining femoral neck length is critical for functional outcomes. Zlowodzki et al. demonstrated that femoral neck shortening of > 5 mm occurs in up to 66% of healed fractures treated with standard sliding screws. This shortening directly correlates with lower SF-36 physical functioning scores and altered abductor mechanics. Utilizing length-stable implants (fully threaded screws or locking plates) in anatomically reduced fractures is essential to preserve the "abductor lever arm."
POSTOPERATIVE CARE AND REHABILITATION
Postoperative weight-bearing protocols must be tailored to the patient's age, bone quality, and the stability of the fixation construct.
- Young, High-Energy Trauma Patients: Restricted to touch-down weight bearing (TDWB) or flat-foot weight bearing (weight of the leg only) for 10 to 12 weeks to protect the fixation while biologic healing occurs.
- Elderly Patients (if ORIF was performed): Allowed protected weight bearing as tolerated with a walker, provided their balance and medical comorbidities permit. Early mobilization is critical in this demographic. Patients who cannot safely ambulate must be aggressively mobilized to a chair to minimize pulmonary complications, deep vein thrombosis (DVT), and decubitus ulcers.
COMPLICATIONS: OSTEONECROSIS AND NONUNION
Despite meticulous surgical technique, intracapsular femoral neck fractures carry a notoriously high complication rate, frequently leading to revision surgery (often conversion to Total Hip Arthroplasty).
Osteonecrosis (Avascular Necrosis - AVN)
The retrograde blood supply to the femoral head is highly susceptible to disruption at the time of injury.
* Incidence: In meta-analyses of young patients (ages 15 to 50), the overall incidence of osteonecrosis is approximately 23%. It develops in 27% of displaced fractures and up to 14% of nondisplaced fractures.
* Capsulotomy Debate: The role of routine capsulotomy remains controversial. Higher intracapsular pressures (tamponade effect) have been demonstrated in nondisplaced fractures compared to displaced fractures (where the capsule is often torn). While capsulotomy relieves this pressure, meticulous care must be taken not to iatrogenically injure the remaining retinacular vessels during the approach.
Nonunion
Failure of the fracture to heal is driven by mechanical instability, poor biology, or a combination of both.
* Incidence: The nonunion rate ranges from 8% to 16%, with higher rates seen in Pauwels Type III fractures due to the difficulty in neutralizing vertical shear forces.
* Prevention: The primary defense against nonunion is an absolute anatomic reduction and the selection of a biomechanically appropriate, length-stable implant. Initial fracture displacement and the quality of the intraoperative reduction are the two most significant independent predictors of both nonunion and osteonecrosis.
By adhering to strict biomechanical principles, utilizing the modified Smith-Petersen approach for direct visualization, and selecting the appropriate fixation construct, the orthopedic surgeon can maximize the probability of joint preservation and functional recovery in these challenging injuries.
You Might Also Like