Carpal Tunnel Syndrome: A Comprehensive Operative Guide for Advanced Orthopaedic Surgeons
Key Takeaway
Carpal tunnel syndrome (CTS) is the most prevalent compressive neuropathy of the upper extremity, resulting from median nerve entrapment within the fibro-osseous carpal tunnel. This comprehensive guide details the pathophysiology, advanced diagnostic modalities, and step-by-step surgical management of CTS. Tailored for orthopedic surgeons, it provides evidence-based protocols for both open and endoscopic carpal tunnel release, ensuring optimal patient outcomes and minimizing postoperative complications.
Carpal Tunnel Syndrome: Etiology, Diagnosis, and Management
Carpal tunnel syndrome (CTS), ulnar tunnel syndrome, and stenosing tenosynovitis represent a spectrum of common compressive neuropathies and inflammatory conditions affecting the hand and wrist. While each presents with distinct clinical features and management strategies, carpal tunnel syndrome—characterized by median nerve compression within the rigid fibro-osseous carpal tunnel—is arguably the most prevalent and extensively studied peripheral neuropathy. This chapter provides an exhaustive, evidence-based review of carpal tunnel syndrome, tailored specifically for advanced orthopedic residents, hand fellows, and practicing consultant surgeons.
Historical Context and Epidemiology
First described by Sir James Paget in 1854 as "tardy median palsy" following a distal radius fracture, the modern understanding of carpal tunnel syndrome as a primary entrapment neuropathy evolved significantly in the mid-20th century. It predominantly affects individuals between 30 and 60 years of age, demonstrating a bimodal distribution, with a two to three times higher incidence in women.
Epidemiological data suggest that CTS affects approximately 1% to 10% of the global population, representing a massive socioeconomic burden in terms of healthcare costs and lost productivity. Extensive longitudinal studies have identified increased age, female gender, elevated Body Mass Index (obesity), cigarette smoking, and occupational tasks involving high-frequency vibration as significant independent risk factors. The causative effect of light, repetitive activities common in modern office work (e.g., keyboard typing) remains a subject of ongoing biomechanical debate and is currently considered controversial, with genetic predisposition often playing a more dominant role than previously recognized.
Anatomy and Biomechanics of the Carpal Tunnel
The carpal tunnel is a rigid, cylindrical, and highly inelastic fibro-osseous canal connecting the volar forearm to the mid-palm. Its precise anatomical confines are critical to understanding the pathophysiology of median nerve compression and the rationale for surgical decompression.
- Dorsal Boundary (Floor): Formed by the concave transverse arch of the carpal bones, specifically the scaphoid, trapezium, trapezoid, capitate, hamate, triquetrum, and pisiform, stabilized by robust intrinsic carpal ligaments.
- Medial Boundary (Ulnar): Composed of the hook of the hamate, the triquetrum, and the pisiform.
- Lateral Boundary (Radial): Defined by the scaphoid tuberosity, the crest of the trapezium, and the fibro-osseous sheath enclosing the flexor carpi radialis (FCR) tendon.
- Ventral Boundary (Palmar Roof): Primarily constituted by the flexor retinaculum. This complex structure includes the deep investing fascia of the forearm proximally, the thick transverse carpal ligament (TCL) over the radiocarpal joint, and the distal aponeurosis between the thenar and hypothenar musculature.
Figure 1: Anatomical representation of the median nerve and flexor tendons within the carpal tunnel.
Within this tightly confined space, the median nerve is the most ventral (superficial/palmar) structure, rendering it highly susceptible to extrinsic compression. Dorsal (deep) to the median nerve lie the nine flexor tendons: four flexor digitorum superficialis (FDS), four flexor digitorum profundus (FDP), and the flexor pollicis longus (FPL).
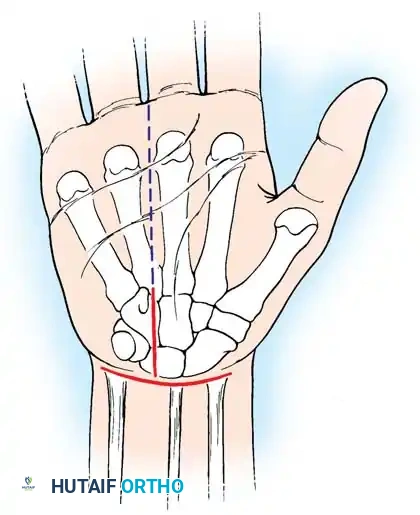
Figure 2: Cross-sectional view of a normal carpal tunnel, illustrating the median nerve (most superficial) and flexor tendons.
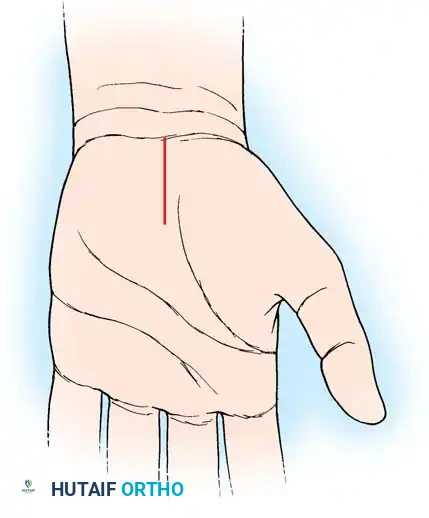
Figure 3: Superficial palmar anatomy highlighting the palmar fascia and its relationship to the underlying transverse carpal ligament.
Critical Neural Anatomy
Surgeons must possess an intimate knowledge of the median nerve's branching patterns to avoid catastrophic iatrogenic injury:
1. Palmar Cutaneous Branch of the Median Nerve (PCBMN): Typically branches 5 cm proximal to the radial styloid, traveling between the FCR and palmaris longus, passing superficial to the TCL to innervate the base of the thenar eminence.
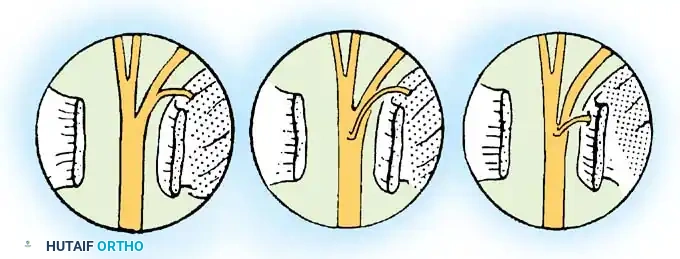
2. Recurrent Motor Branch: Exhibits significant anatomical variance (Lanz classifications). It most commonly branches extraligamentously and recurrently, but can be subligamentous, transligamentous, or originate from the ulnar aspect of the median nerve.
Pathophysiology of Nerve Compression
Carpal tunnel syndrome arises from a pathological elevation of interstitial pressure within the carpal tunnel. Normal resting intracarpal pressure ranges from 2 to 10 mmHg. In CTS, baseline pressures frequently exceed 20 to 30 mmHg.
This sustained pressure gradient impedes epineurial venous return, leading to a cascade of localized venous congestion, nerve ischemia, and impaired axoplasmic transport. Prolonged ischemia induces endoneurial edema, fibroblast proliferation, and ultimately, irreversible myelin thinning and axonal degeneration.

Figure 4: Cross-sectional view demonstrating compression of the median nerve within the carpal tunnel due to increased contents or reduced space.
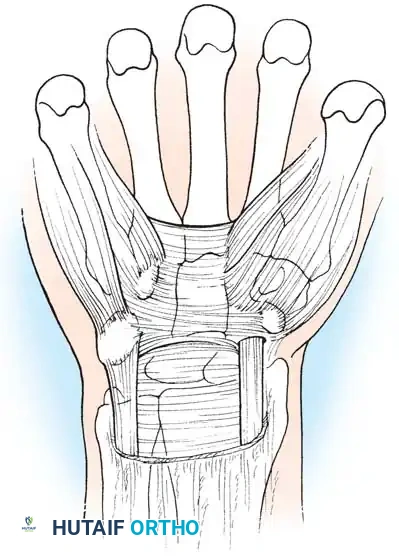
Figure 5: Another cross-sectional illustration highlighting the compressed median nerve and subsequent morphological flattening.
Any condition that alters the volume-to-content ratio of the carpal tunnel can initiate this ischemic cascade:
- Decrease in Carpal Tunnel Capacity:
- Bony abnormalities (e.g., malunited distal radius fractures).
- Dynamic postural changes: Wrist flexion or extension significantly increases intracarpal pressure. Pressure can spike from a neutral 25 mmHg to over 100 mmHg with 90 degrees of wrist flexion or extension.
- Increase in Carpal Tunnel Contents:
- Traumatic: Hematoma, post-traumatic arthritis, perilunate dislocations.
- Space-Occupying Lesions: Ganglion cysts, lipomas, schwannomas, or tophaceous gout.
- Anatomical Variants: Proximal lumbrical muscle belly excursion during finger flexion, persistent median artery.
- Inflammatory/Systemic: Nonspecific tenosynovial hypertrophy (the most common histological finding in "idiopathic" CTS), rheumatoid arthritis, diabetes mellitus, hypothyroidism, and pregnancy-induced fluid retention.
Clinical Presentation
Patients typically present with insidious onset of paresthesia (tingling, numbness, or a "pins and needles" sensation) strictly within the median nerve distribution: the thumb, index, long, and the radial half of the ring finger.
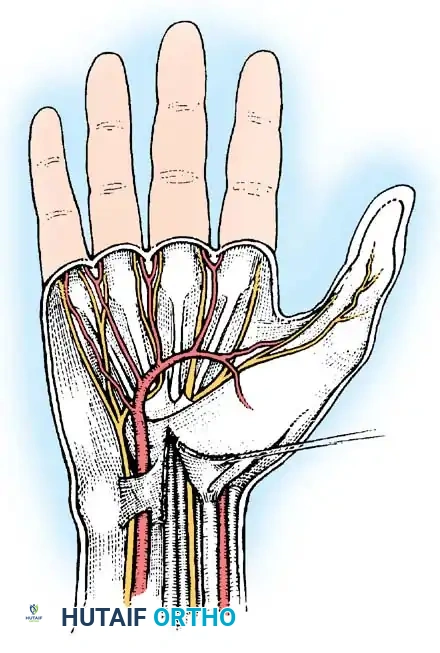
Figure 6: Sensory distribution of the median nerve in the hand.
Pain is frequently described as a deep, aching, or throbbing sensation that may radiate proximally into the volar forearm, elbow, or even the shoulder (retrograde pain).
Clinical Pearl: Nocturnal awakening is a hallmark symptom. Patients frequently report waking in the middle of the night with severe burning and numbness, which is temporarily relieved by vigorously shaking or "wringing out" the hand (the Flick Sign).
Late-stage presentations involve profound sensory loss, dropping objects due to loss of tactile feedback, and visible atrophy of the thenar musculature (abductor pollicis brevis, opponens pollicis), indicating severe axonal loss.
Diagnostic Evaluation
A meticulous clinical history and physical examination remain the gold standard for diagnosing CTS, often supported by electrodiagnostic testing.
Provocative Clinical Testing
- Durkan Carpal Compression Test: Direct manual compression over the transverse carpal ligament for 30 seconds. This is currently recognized as the most sensitive (87%) and specific (90%) provocative maneuver.
- Phalen Maneuver: Unforced, complete palmar flexion of the wrists for 60 seconds. A positive test reproduces paresthesia in the median nerve territory.
- Tinel Sign: Gentle percussion over the median nerve at the wrist crease. While highly specific, it lacks sensitivity compared to the Durkan test.
- Semmes-Weinstein Monofilament Testing: A quantitative assessment of threshold sensibility. It is highly sensitive for detecting early, subtle nerve compression before two-point discrimination becomes abnormal.
Electrodiagnostic Studies (NCS/EMG)
While the diagnosis of CTS is primarily clinical, Nerve Conduction Studies (NCS) and Electromyography (EMG) are invaluable for confirming the diagnosis, quantifying the severity of nerve impairment, and ruling out proximal compression (e.g., cervical radiculopathy, Pronator Teres syndrome).
- NCS: Pathognomonic findings include prolonged distal sensory latencies (>3.5 ms) and prolonged distal motor latencies (>4.5 ms), alongside decreased conduction velocities across the wrist.
- EMG: Evaluates the muscular response to denervation. Findings such as fibrillation potentials, positive sharp waves, and decreased motor unit recruitment in the abductor pollicis brevis indicate advanced, severe compression with axonal loss.
Surgical Warning: Up to 10-15% of patients with clinically classic CTS may have normal electrodiagnostic studies. A normal EMG/NCS does not preclude surgical intervention if the clinical picture is definitive and conservative measures have failed.
Non-Operative Management
Conservative management is the first-line approach for mild to moderate CTS without evidence of motor atrophy or profound sensory loss.
- Volar Wrist Splinting: Immobilization of the wrist in a neutral position (0-5 degrees of extension) maximizes carpal tunnel volume and minimizes intracarpal pressure. Night splinting is particularly effective for resolving nocturnal symptoms.
- Corticosteroid Injections: An injection of a corticosteroid (e.g., methylprednisolone) mixed with local anesthetic into the carpal tunnel provides potent anti-inflammatory effects, reducing tenosynovial edema.
> Pitfall: The needle must be introduced ulnar to the palmaris longus tendon to avoid direct intraneural injection into the median nerve, which can cause devastating, permanent iatrogenic nerve injury. - Activity Modification and Ergonomics: Minimizing repetitive wrist flexion/extension and reducing exposure to vibratory tools.
Operative Management: Carpal Tunnel Release
Surgical decompression—Carpal Tunnel Release (CTR)—is indicated when non-operative modalities fail after 3 to 6 months, or immediately in the presence of severe disease characterized by thenar atrophy, constant numbness, or profound electrodiagnostic abnormalities.
Pre-operative Planning and Anesthesia
Modern carpal tunnel surgery is frequently performed under WALANT (Wide Awake Local Anesthesia No Tourniquet). This technique utilizes a mixture of lidocaine, epinephrine, and sodium bicarbonate injected locally. It eliminates the need for an upper arm tourniquet, avoids the risks of general anesthesia, and allows the surgeon to assess active finger flexion intraoperatively to confirm complete release of the flexor retinaculum.
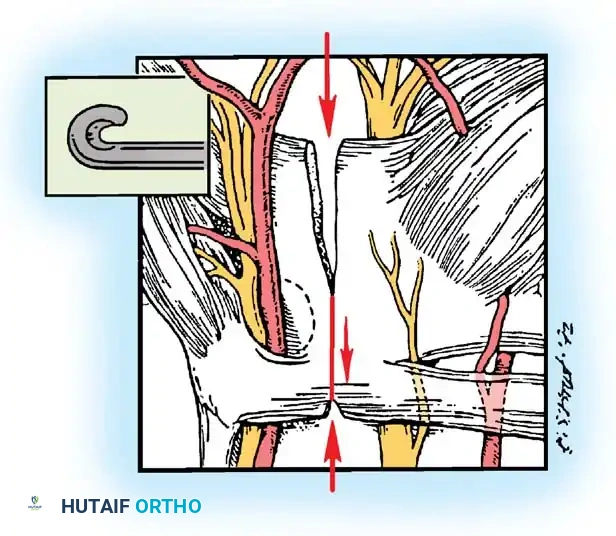
Figure 7: Typical patient positioning for carpal tunnel release, with the arm extended on a hand table.
Technique 1: Open Carpal Tunnel Release (OCTR)
OCTR remains the gold standard, offering direct, unparalleled visualization of the median nerve and surrounding anatomy.
Step 1: Incision Planning
The incision is planned along the longitudinal axis of the radial border of the ring finger. It begins at the intersection of Kaplan's cardinal line (a line drawn from the apex of the interdigital fold between the thumb and index finger toward the ulnar side of the wrist) and extends proximally for approximately 3-4 cm, stopping just distal to the distal wrist crease to avoid crossing the crease perpendicularly.
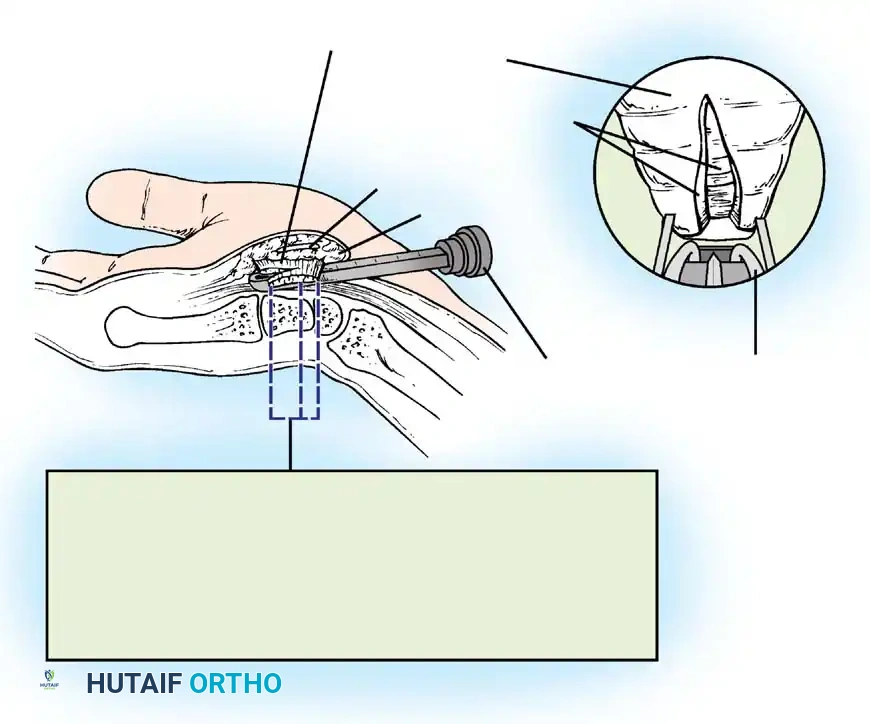
Figure 8: Surface landmarks for open carpal tunnel release. Note the relationship to the distal wrist crease and the axis of the ring finger.
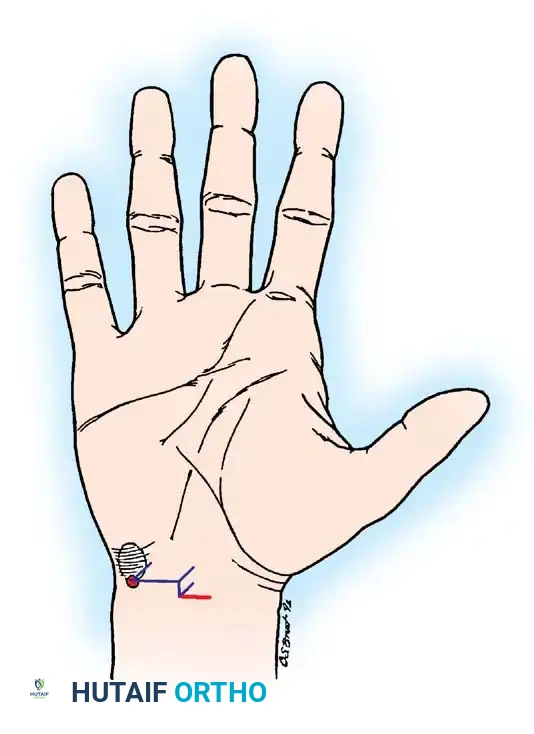
Figure 9: Detailed incision marking intersecting Kaplan's cardinal line, ensuring a safe approach ulnar to the palmar cutaneous branch.
Step 2: Superficial Dissection
The skin and subcutaneous fat are incised. The palmar aponeurosis is identified and longitudinally divided. Care is taken to stay strictly ulnar to the longitudinal axis of the palmaris longus to protect the Palmar Cutaneous Branch of the Median Nerve (PCBMN).
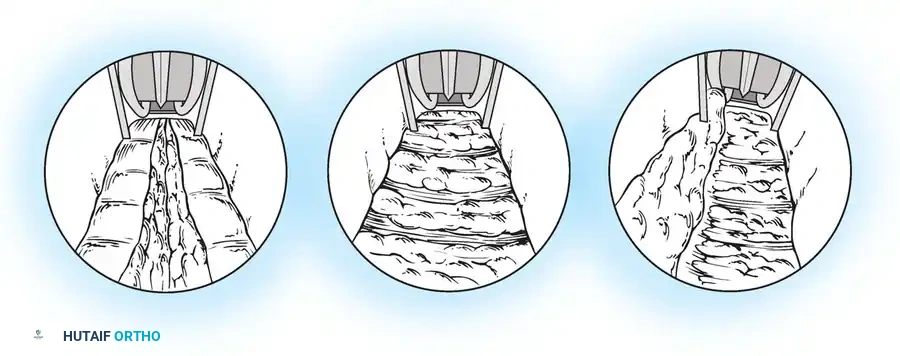
Figure 10: Superficial dissection highlighting the palmar fascia. The PCBMN lies radially and must be protected.
Step 3: Division of the Transverse Carpal Ligament
The distal edge of the TCL is identified. Using a scalpel or specialized scissors, the TCL is divided longitudinally along its extreme ulnar border. Releasing the ligament on the ulnar side prevents injury to the median nerve and its recurrent motor branch.
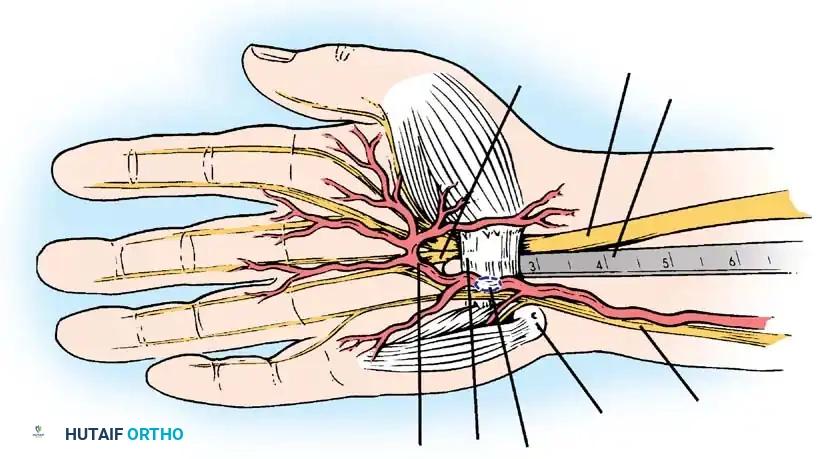
Figure 11: Initial division of the transverse carpal ligament.
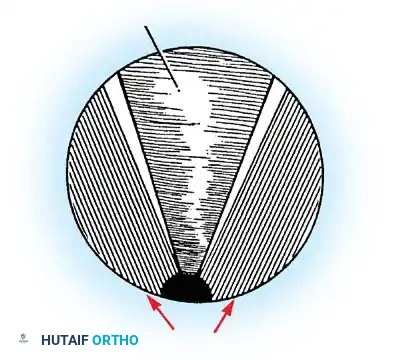
Figure 12: Complete longitudinal division of the TCL, exposing the underlying median nerve and flexor tenosynovium.
Step 4: Deep Exploration and Decompression
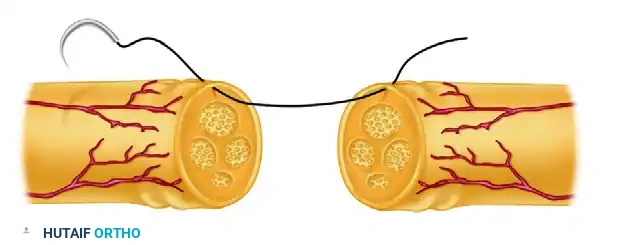
Once the TCL is fully divided, the median nerve is inspected for areas of pseudoneuroma (proximal swelling) or hourglass constriction. The recurrent motor branch is identified to ensure it has not been inadvertently injured or tethered by a transligamentous course.
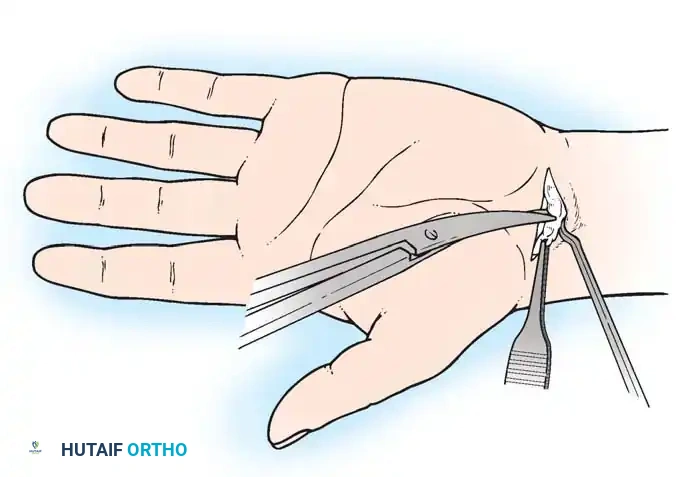
Figure 13: Deep exposure demonstrating the decompressed median nerve. The recurrent motor branch is visualized and protected.
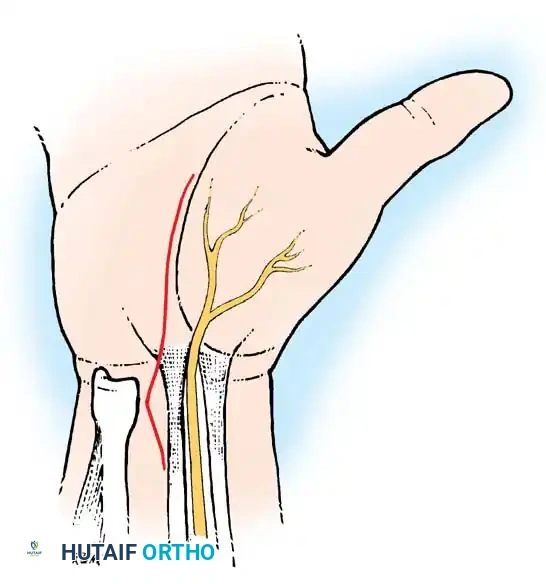
Figure 14: Anatomical variations of the recurrent motor branch of the median nerve (Lanz classification), highlighting the importance of careful distal dissection.
The distal extent of the release is confirmed by visualizing the superficial palmar arch and the fat pad indicating the distal edge of the flexor retinaculum. Proximally, the deep antebrachial fascia is released for 2-3 cm proximal to the wrist crease under direct vision.
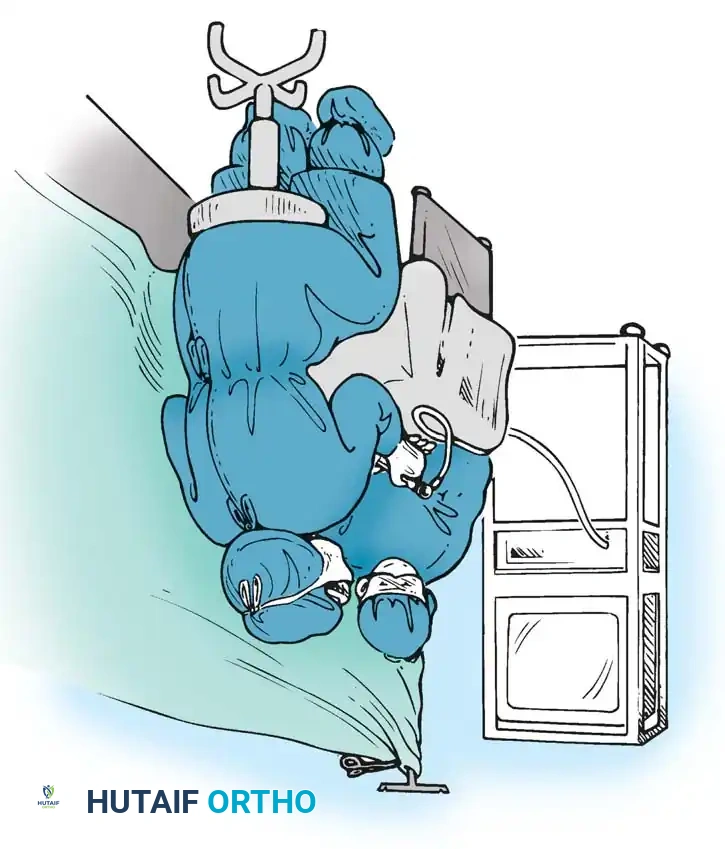
Figure 15: The distal extent of the release, carefully avoiding the superficial palmar arch.
Step 5: Closure
The tourniquet (if used) is deflated, and meticulous hemostasis is achieved. Only the skin is closed using non-absorbable horizontal mattress sutures (e.g., 4-0 Nylon). The TCL and palmar fascia are left open to allow for expansion of the carpal tunnel volume.
Technique 2: Endoscopic Carpal Tunnel Release (ECTR)
ECTR was developed to minimize palmar morbidity, specifically "pillar pain," and accelerate return to work. It can be performed via a single-portal (Agee) or two-portal (Chow) technique.
Step 1: Portal Placement
For the single-portal technique, a small transverse incision is made proximal to the distal wrist crease, between the FCR and FCU tendons.
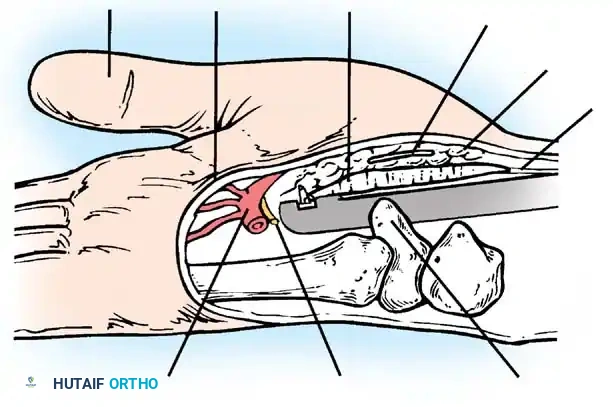
Figure 16: Insertion of the endoscopic trocar assembly through the proximal portal.
Step 2: Instrumentation and Visualization
A synovial elevator is used to clear the undersurface of the TCL. The endoscope/blade assembly is introduced into the carpal tunnel, hugging the deep surface of the TCL to remain superficial to the median nerve.
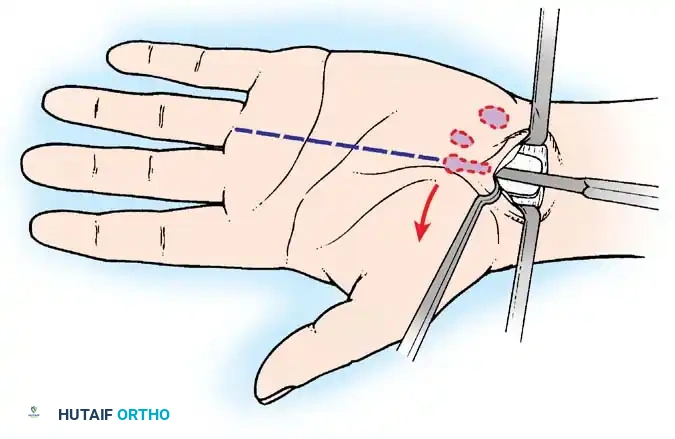
Figure 17: Cross-sectional diagram illustrating the endoscopic device positioned safely beneath the TCL and above the median nerve.
Step 3: Ligament Release
The distal edge of the TCL is identified endoscopically. The retrograde blade is deployed, and the ligament is divided from distal to proximal under direct video visualization.
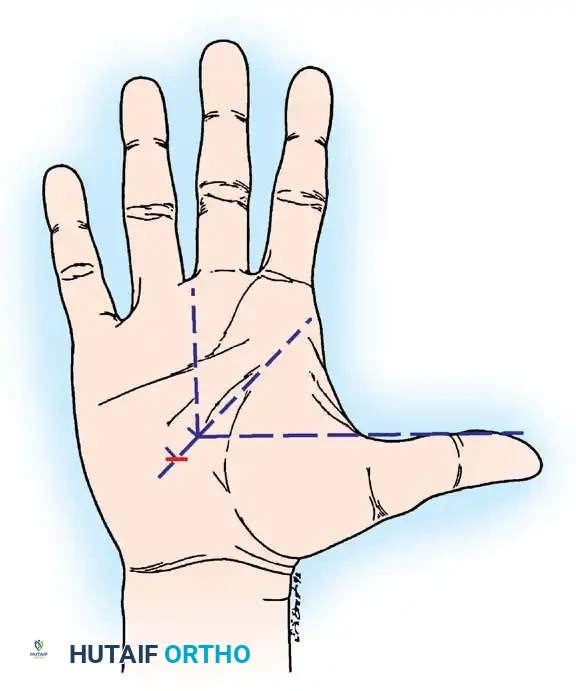
Figure 18: Endoscopic view of the blade deployed against the undersurface of the transverse carpal ligament.
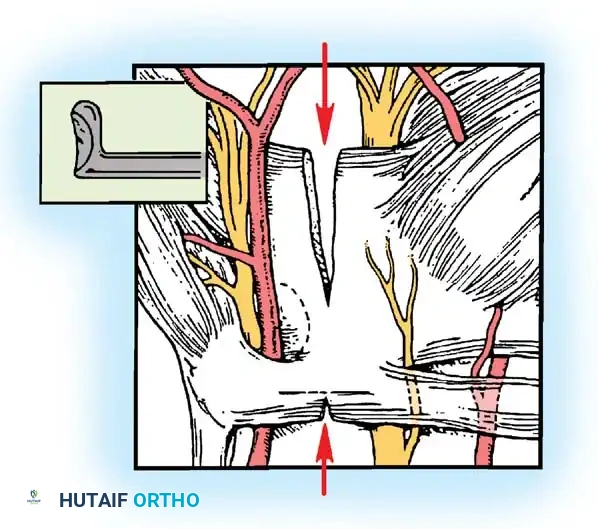
Figure 19: The blade dividing the TCL as the assembly is withdrawn proximally.
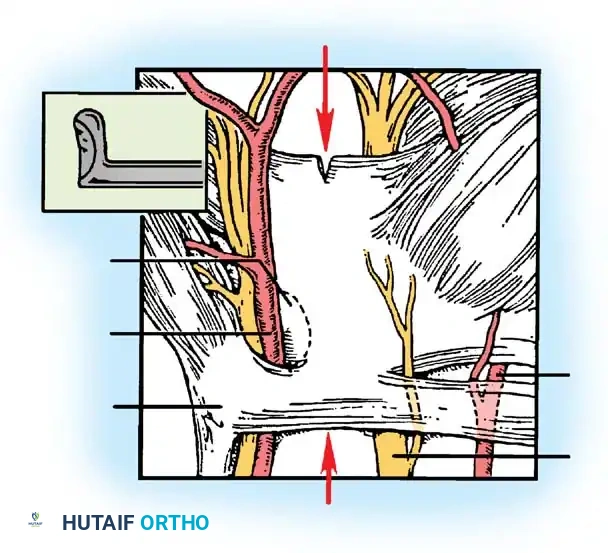
Figure 20: Endoscopic confirmation of the completely divided transverse carpal ligament, showing the separated edges.
Step 4: Verification
The endoscope is re-inserted to verify complete division of the ligament. Any remaining distal or proximal fascial bands are meticulously cut.
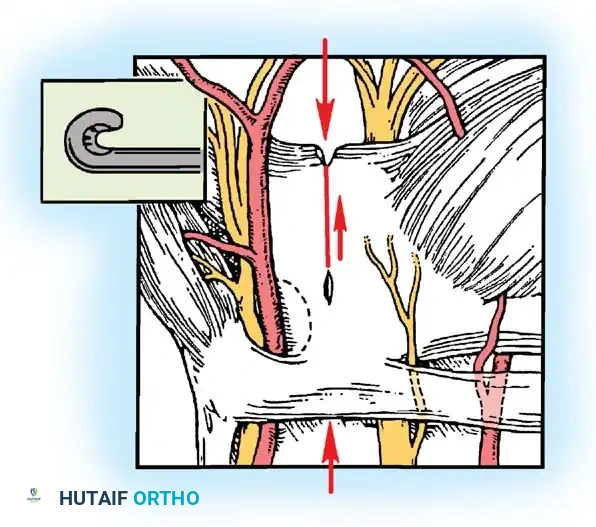
Figure 21: Final endoscopic inspection to ensure no residual fascial bands remain across the median nerve.
Postoperative Protocol and Rehabilitation
Postoperative management focuses on early mobilization to prevent tendon adhesions and nerve tethering.
* Days 1-14: A bulky soft dressing is applied. Patients are instructed to perform immediate, active composite finger flexion and extension exercises, as well as nerve gliding protocols. Rigid wrist immobilization is generally avoided as it promotes stiffness.
* Weeks 2-4: Sutures are removed at 10-14 days. Scar massage and desensitization techniques are initiated.
* Weeks 4-6: Progressive strengthening of the grip and pinch mechanisms. Most patients return to heavy manual labor by 4 to 6 weeks, though maximal grip strength may take up to 3 months to fully recover.
Complications and Surgical Pitfalls
While highly successful, carpal tunnel release carries specific risks that the advanced surgeon must anticipate:
- Incomplete Release: The most common cause of persistent postoperative symptoms. It typically occurs at the distal extent of the TCL or the proximal deep antebrachial fascia.
- Pillar Pain: A deep, aching pain in the thenar and hypothenar eminences following surgery. It is more common in open releases and typically resolves spontaneously within 3 to 6 months.
- Nerve Injury:
- PCBMN Injury: Results in painful neuromas and numbness over the thenar eminence. Prevented by keeping the incision ulnar to the palmaris longus axis.
- Recurrent Motor Branch Injury: Results in catastrophic loss of thumb opposition. Prevented by releasing the TCL on its extreme ulnar border.
- Digital Nerve Injury: The common digital nerve to the 3rd web space is at risk during blind distal dissection.
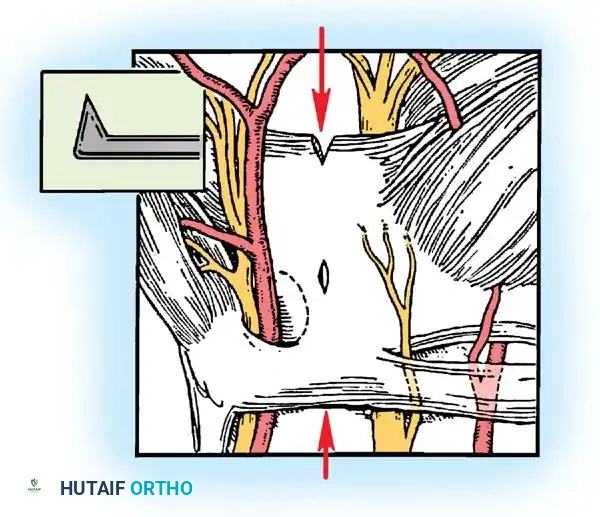
Figure 22: Anatomical diagram emphasizing the "safe zones" for incision and dissection to prevent iatrogenic injury to the median nerve branches and superficial palmar arch.
Conclusion
Carpal tunnel syndrome requires a nuanced understanding of wrist biomechanics, peripheral nerve pathophysiology, and precise surgical anatomy. Whether utilizing a classic open approach or an advanced endoscopic technique, the paramount goals remain the complete, safe decompression of the median nerve and the rapid restoration of hand function. Mastery of these techniques, combined with rigorous patient selection and meticulous postoperative care, ensures excellent, reproducible outcomes in the management of this ubiquitous compressive neuropathy.
You Might Also Like