Flexor Tenolysis After Repair and Grafting: Master Surgical Guide
Key Takeaway
Flexor tenolysis is a complex salvage procedure indicated when restrictive peritendinous adhesions halt functional progression following primary flexor tendon repair or grafting. Success relies on meticulous surgical release of scar tissue while preserving the critical annular pulleys, combined with immediate postoperative active mobilization. Utilizing wide-awake local anesthesia (WALANT) allows intraoperative assessment of active range of motion, ensuring complete release and guiding the necessity for concurrent pulley reconstruction or staged grafting.
INTRODUCTION TO FLEXOR TENOLYSIS
Flexor tenolysis is one of the most demanding and unpredictable procedures in hand surgery. Following primary flexor tendon repair or free tendon grafting, the biological process of tendon healing inevitably involves both intrinsic and extrinsic pathways. When the extrinsic healing response predominates, dense peritendinous adhesions form between the tendon, the fibroosseous sheath, and the surrounding periosteum. These adhesions restrict tendon excursion, leading to a profound discrepancy between passive and active range of motion (ROM).
The primary objective of flexor tenolysis is to meticulously liberate the adherent tendon from surrounding scar tissue, restoring its gliding mechanism without compromising its vascularity or structural integrity. This procedure is strictly indicated as a salvage operation when a patient has reached a definitive plateau in postoperative rehabilitation—typically no earlier than 3 to 6 months following the index surgery.
Clinical Pearl: Tenolysis should never be performed prophylactically or prematurely. The soft tissue envelope must be supple, the scars mature, and the joints mobilized to their maximum passive capacity before surgical intervention is considered. If passive motion is poor, tenolysis will fail; joint contractures must be addressed either prior to or concurrently with the tenolysis.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Assessing Tendon Adherence
A thorough clinical examination is paramount to localize the exact site of adherence. The biomechanical presentation of tendon adhesions is highly predictable based on the anatomical zone of injury:
* Sublimis (Flexor Digitorum Superficialis - FDS) Adherence: The FDS tendon most commonly adheres to the proximal phalanx. This tethers the tendon and creates a persistent flexion contracture of the proximal interphalangeal (PIP) joint.
* Profundus (Flexor Digitorum Profundus - FDP) Adherence: The FDP tendon typically adheres to the middle phalanx, resulting in a flexion contracture of the distal interphalangeal (DIP) joint.
* Extensor Tendon Adherence: While primarily a flexor issue, concurrent extensor adhesions to the metacarpal shaft or proximal phalanx can exacerbate stiffness and must be evaluated.
Adherence to Fracture Sites
Tendon adherence is exponentially more severe when associated with phalangeal fractures. The adherence of a tendon to a fracture site is usually associated with one of four primary factors:
1. Volar Angulation: Poor reduction of a phalangeal fracture with volar apex angulation directly impinges on the flexor apparatus.
2. External Pressure: Improper splinting or external pressure forcing the tendon against the fracture callus during the healing phase.
3. Crush Injuries: Severe soft tissue trauma that obliterates the gliding planes and induces massive fibroblastic proliferation.
4. Laceration of the Tendon Sheath: Disruption of the synovial barrier allows osteoblasts and fibroblasts from the fracture site to directly invade the tendon.
ANESTHESIA AND POSITIONING
The advent of Wide-Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized flexor tenolysis. Utilizing a mixture of lidocaine and epinephrine allows for profound local anesthesia and hemostasis without the need for a pneumatic tourniquet or general anesthesia.
Surgical Warning: If a regional or local block anesthetic is used for the tenolysis, the patient can voluntarily show the amount of motion in the finger intraoperatively. This active participation is invaluable; it provides immediate visual confirmation that the adhesions have been completely released and that the tendon is structurally intact enough to withstand active contraction.
If general anesthesia is utilized, the surgeon must rely on the traction effect by making a separate incision in the distal forearm to pull the proximal tendon, confirming that the finger can be moved through a nearly normal full range of motion.
SURGICAL TECHNIQUE: STEP-BY-STEP
1. Incision and Exposure
Make the incision through the existing skin scar to avoid creating new ischemic skin bridges. Bruner zigzag incisions or mid-lateral approaches are standard.
* When elevating the skin flaps, exercise extreme caution to avoid injury to the neurovascular bundles, which are often displaced or encased in scar tissue from the previous trauma.
* Preserve the annular portions of the fibroosseous sheath (specifically the A2 and A4 pulleys) at all costs.
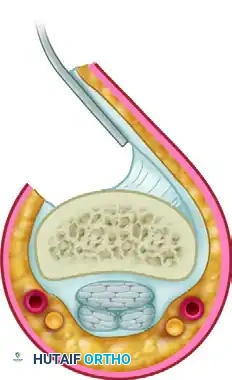
2. Dissection and Tendon Release
Using great care, dissect the scar tissue from the tendon. In severe cases, the tendon and the fibroosseous sheath are visually indistinguishable.
* Begin the dissection in areas of normal anatomy, typically proximal and distal to the zone of maximal injury, and work toward the epicenter of the scar.
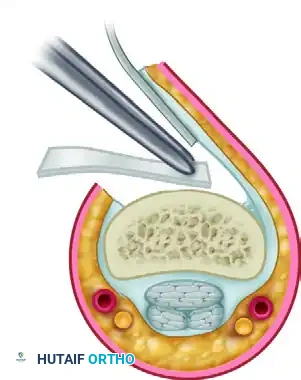
* Use sharp dissection (e.g., a #15 blade) and fine periosteal elevators to free the flexor tendon from the adherent periosteum and fibroosseous sheath.
* Similarly, the tendon sometimes adheres densely to the phalanx, particularly in areas of healed fracture callus. Elevate the tendon off the bone meticulously to avoid fraying the tendon fibers.
3. Management of Irregular Bony Surfaces
Sometimes, especially with comminuted fractures in which irregular bony surfaces are exposed after elevating the tendon, the risk of immediate readherence is exceptionally high. In these specific salvage scenarios, silicone sheeting has been interposed between the tendon and the bone to act as a physical barrier.
This silicone sheeting prevents the raw tendon surface from adhering to the osteogenic fracture callus. It is left in place during the early rehabilitation phase and removed later after satisfactory active motion has been established.
4. Intraoperative Assessment of Motion
Once the tendon appears visually free, its functional excursion must be tested.
* Under WALANT: Ask the patient to actively flex and extend the digit. Observe the tendon gliding beneath the preserved pulleys.
* Under General Anesthesia: After determining that the tendon has been completely released in the digit, make an incision in the distal forearm, identify the appropriate flexor tendon, and show with traction on the proximal tendon that the finger can be moved through a nearly normal full range of motion.
5. Addressing Joint Contractures
If flexion contractures are present at the proximal and distal interphalangeal joints that do not resolve with tenolysis alone, release these by capsulotomy. This is usually achieved by the release of the proximal extensions (checkrein ligaments) of the palmar plate.
6. Contingency Planning: Unsalvageable Tendons
During tenolysis, the surgeon may discover that the tendon is severely attenuated, partially ruptured, or structurally insufficient to withstand active motion.
* If the flexor tendon cannot be salvaged because of extensive injury, or if the flexor tendon graft has ruptured, the tenolysis must be converted to the first stage of a two-stage flexor tendon graft reconstruction.
* Insert a silicone rod (Hunter rod) beneath any remaining or reconstructed pulleys.
* If it can be shown that the annular pulleys are not present, or if the remaining pulleys are insufficient for proper finger function, perform pulley reconstruction over the silicone rod at the time of the index procedure.
7. Contingency Planning: Irreparable Profundus Damage
In cases where the FDS is intact and functioning well, but the FDP is irreparably damaged or ruptured in Zone I/II, restoring DIP joint stability becomes the priority. A tenodesis or arthrodesis of the DIP joint is indicated.
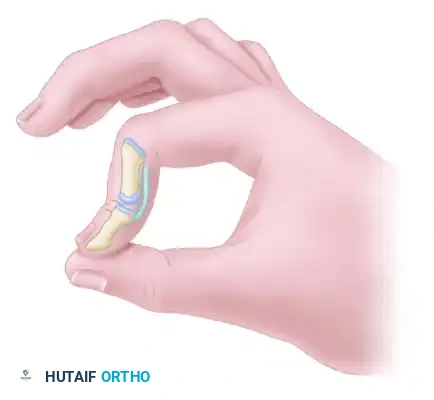
Before tenodesis, the distal interphalangeal joint is unstable and hyperextends during pinch, severely compromising grip strength and fine motor function.
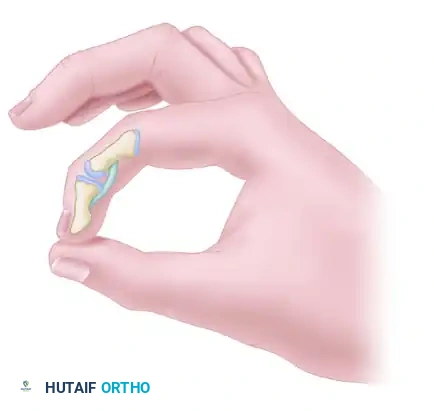
After tenodesis, the joint is stable and remains partially flexed (typically positioned at 10 to 15 degrees of flexion) during pinch, providing a rigid post against which the thumb can oppose.
CONCURRENT EXTENSOR TENDON ADHESIONS
While addressing the flexor surface, the surgeon must remain cognizant of the extensor mechanism. An extensor tendon usually adheres to the metacarpal shaft or proximal phalanx following crush injuries or fractures. Surgery may be indicated when the tendon fails to loosen by active exercise, as determined by measurements of motion of adjacent joints. Techniques such as the Howard technique are employed to free the adherent extensor tendon, ensuring that reciprocal active extension is not blocking the newly restored flexor excursion.
PHARMACOLOGIC ADJUNCTS
The use of pharmacologic agents to prevent adhesion reformation remains controversial.
* Corticosteroids: Usually, corticosteroids are not instilled into the wound bed. While they decrease fibroblastic proliferation, they also severely inhibit intrinsic tendon healing and increase the risk of spontaneous postoperative tendon rupture.
* Pain Control: Indwelling catheters for pain control with local anesthetics rarely are used, although they can be highly helpful in controlling immediate postoperative pain, thereby facilitating early active motion.
POSTOPERATIVE CARE AND REHABILITATION
The success of a flexor tenolysis is entirely dependent on the postoperative rehabilitation protocol. The biological race between restoring tendon glide and the reformation of scar tissue begins immediately in the recovery room.
Immediate Postoperative Phase (Days 1-3)
- A compression dressing is applied in the operating room, usually with the fingers in mild flexion, allowing the thumb metacarpophalangeal and interphalangeal joints to be in extension or only slight flexion.
- Drains usually are unnecessary. Any drains that are placed are removed at approximately 24 hours or when drainage has ceased.
- Postoperative rehabilitation is begun with active motion on the first day after surgery. The patient must be psychologically prepared to push through mild to moderate discomfort to maintain the glide achieved intraoperatively.
Early Mobilization Phase (Weeks 1-3)
- Although an early postoperative mobilization program can be undertaken, it requires strict compliance.
- The tenodesis effect is utilized heavily in therapy: active extension of the wrist can initiate passive flexion of the metacarpophalangeal joint through the adherent tendon. Similarly, active flexion of the DIP joint can be increased by passive flexion of the PIP joint.
- The sutures are removed at 10 to 14 days.
- The initial splint is left in place for approximately 3 weeks, and then gentle active motion is progressed.
Intermediate to Late Phase (Weeks 4-12)
- The thumb (if involved) is protected with an additional removable dorsal splint for another 3 to 4 weeks, and motion exercises are increased.
- Because the tendon has been surgically stripped of its vascular adhesions, it undergoes a period of transient avascularity and structural weakness. Therefore, forceful resistance activities are strictly prohibited and are not undertaken for 10 to 12 weeks postoperatively to prevent catastrophic rupture.
Clinical Pearl: The patient must understand that tenolysis is not a "quick fix." It is a reset of the rehabilitation clock. Failure to adhere to the strict active motion protocols, or conversely, applying excessive resistive force too early, will result in either recurrent stiffness or tendon rupture, both of which represent devastating complications.
📚 Medical References
- Flexor tenolysis in children, J Hand Surg 20A:254, 1995.
- Boyer MI, Gelberman RH, Burns ME, et al: Intrasynovial fl exor tendon repair: an experimental study comparing low and high levels of in vivo force during rehabilitation in canines, J Bone Joint Surg 83A:891, 2001.
- Boyer MI, Strickland JW, Engles D, et al: Flexor tendon repair and rehabilitation: state of the art in 2002, Instr Course Lect 52:137, 2003.
- Buscemi MJ, Page BJ: Flexor digitorum profundus avulsions with associated distal phalanx fractures, Am J Sports Med 15:366, 1987.
- Cheung KMC, Chow SP: Closed avulsion of both fl exor tendons of the ring fi nger, J Hand Surg 20B:78, 1995.
- Dobyns RC, Cooney WP, Wood MB: The effect of partial lacerations on canine fl exor tendons, Minn Med 65:27, 1982.
- Drapé JL, Silbermann-Hoffman O, Houvet P, et al: Complications of fl exor tendon repair in the hand: MR imaging assessment, Radiology 198:219, 1996.
- Elliot D, Harris SB: The assessment of fl exor tendon function after primary tendon repair, Hand Clin 19:495, 2003.
- Esplin VS, Tencer AF, Hanel DP, et al: Restoration of function of the thumb fl exor apparatus requires repair of the oblique and one adjacent fl exor tendon pulley, J Orthop Res 14:152, 1996.
- Grewal R, Sotereanos DG, Rao U, et al: Bundle pattern of the fl exor digitorum profundus tendon in zone II of the hand: a quantitative assessment of the size of a laceration, J Hand Surg 21A:978, 1996.
- Hariharan JS, Diao E, Soejima O, et al: Partial lacerations of human digital fl exor tendons: a biomechanical analysis, J Hand Surg 22A:1011, 1997.
- Harris SB, Harris D, Foster AJ, et al: The aetiology of acute rupture of fl exor tendon repairs in zones 1 and 2 of the fi ngers during early mobilization, J Hand Surg 24B:275, 1999.
- Hill BB, Wells MD, Prevel CD: Endoscopic retrieval of severed fl exor tendons: a study of technique using cadaver hands, Ann Plast Surg 38:446, 1997.
- Honnor R: The late management of the isolated lesion of the fl exor digitorum profundus tendon, Hand 7:171, 1975.
- Jobe MT, Caviale P, Milford LW: The digital palmar oblique incision, J Hand Surg 18A:525, 1993.
- Ketchum LD: Suture materials and suture techniques used in tendon repair, Hand Clin 1:43, 1985.
- Kleinert HE: Should an incompletely severed tendon be sutured? The voice of polite dissent, Plast Reconstr Surg 57:236, 1976.
- Kleinert HE, Bennett JB: Digital pulley reconstruction employing the always present rim of the previous pulley, J Hand Surg 3A:297, 1978.
- Kleinert HE, Kutz JE, Cohen MJ: Primary repair zone 2 fl exor tendon lacerations. In American Academy of Orthopaedic Surgeons: Symposium on tendon surgery in the hand, St Louis, 1975, Mosby. Kleinert HE, Meares A: In quest of the solution to severed fl exor tendons, Clin Orthop Relat Res 104:23, 1974.
- Leddy JP: Avulsions of the fl exor digitorum profundus, Hand Clin 1:77, 1985.
- Leddy JP, Packer JW: Avulsion of the profundus tendon insertion in athletes, J Hand Surg 2:66, 1977.
- Lee DH, Robbin ML, Galliott R, et al: Ultrasound evaluation of fl exor tendon lacerations, J Hand Surg 25A:236, 2000.
- Lister G: Indications and techniques for repair of the fl exor tendon sheath, Hand Clin 1:85, 1985.
- Lister G: Pitfalls and complications of fl exor tendon surgery, Hand Clin 1:133, 1985.
- Lister GD: Reconstruction of pulleys employing extensor retinaculum, J Hand Surg 4A:461, 1979.
- Lister GD, Kleinert HE, Kutz JE, et al: Primary fl exor tendon repair followed by immediate controlled mobilization, J Hand Surg 2A:441, 1977.
- Littler JW: The severed fl exor tendon, Surg Clin North Am 39:435, 1959.
- Luo J, Mass DP, Phillips CS, et al: The future of fl exor tendon surgery, Hand Clin 21:267, 2005.
- Manske PR: History of fl exor tendon injury, Hand Clin 21:123, 2005.
- Matev I, Karancheva S, Trichkova P, et al: Delayed primary suture of fl exor tendons cut in the digital theca, Hand 12:158, 1980.
- Mautloub HS, Dzwierzynski WW, Erickson S, et al: Magnetic resonance imaging scanning in the diagnosis of the zone II fl exor tendon rupture, J Hand Surg 21A:451, 1996.
- Mehta V, Phillips CS: Flexor tendon pulley reconstruction, Hand Clin 21:245, 2005.
- Messina A, Messina JC: The direct midlateral approach with lateral enlargement of the pulley system for repair of fl exor tendons in fi ngers, J Hand Surg 21B:463, 1996.
- Moiemen NS, Elliot D: Primary fl exor tendon repair in zone 1, J Hand Surg 25B:78, 2000.
- Murphy BA, Mass DP: Zone I fl exor tendon injuries, Hand Clin 21:167, 2005.
- Naam NH: Intratendinous rupture of the fl exor digitorum profundus tendon in zones II and III, J Hand Surg 20A:478, 1995.
- Nunley JA, Levin LS, Devito D, et al: Direct end-to-end repair of fl exor pollicis longus tendon lacerations, J Hand Surg 17A:118, 1992.
- Papandrea R, Seitz WH, Shapiro P, et al: Biomechanical and clinical evaluation of the epitenon-fi rst technique of fl exor tendon repair, J Hand Surg 20A:261, 1995.
- Parkes A: The “lumbrical plus” fi nger, J Bone Joint Surg 53B:236, 1971.
- Pulvertaft RG: Problems of fl exor-tendon surgery of the hand, J Bone Joint Surg 47A:123, 1965.
- Reynolds B, Wray RC Jr, Weeks PM: Should an incompletely severed tendon be sutured? Plast Reconstr Surg 57:36, 1976.
- Schlenker JD, Lister GD, Kleinert HE: Three complications of untreated partial laceration of fl exor tendon, J Hand Surg 6A:392, 1981.
- Schneider LH, Hunter JM, Norris TR, et al: Delayed fl exor tendon repair in no man’s land, J Hand Surg 2A:452, 1977.
- Silfverskiöld KL, May EJ, Oden A: Factors affecting results after fl exor tendon repair in zone II: a multivariate prospective analysis, J Hand Surg 18A:654, 1992.
- Silfverskiöld KL, May EJ, Törnvall AH: Gap formation during controlled motion after fl exor tendon repair in zone II: a prospective clinical study, J Hand Surg 17A:539, 1992.
- Silva MJ, Hollstien SB, Fayazi AH, et al: The effects of multiplestrand suture techniques on the tensile properties of repair of the fl exor digitorum profundus tendon to bone, J Bone Joint Surg 80A:1507, 1998.
- Soejima O, Diao E, Lotz JC, et al: Comparative mechanical analysis of dorsal versus palmar placement of core suture for fl exor tendon repairs, J Hand Surg 20A:801, 1995.
- Stahl S, Goldberg JA, Lerner A: Flexor tendon lengthening in zone II injuries, Ann Plast Surg 43:265, 1999 . Stamos BD, Leddy JP: Closed tendon disruption in athletes, Hand Clin 16:359, 2000.
- Stefanich RJ, Putnam MD, Peimer CA, et al: Flexor tendon lacerations in zone V, J Hand Surg 17A:284, 1992.
- Stern JD, Mitra A, Spears J: Isolated avulsion of the fl exor digitorum superfi cialis tendon, J Hand Surg 20A:642, 1995.
- Stone JF, Davidson JSD: The role of antibiotics and timing of repair in fl exor tendon injuries of the hand, Ann Plast Surg 40:7, 1998.
- Strickland JW: Management of acute fl exor tendon injuries, Orthop Clin North Am 14:841, 1983.
- Strickland JW: Flexor tendon repair, Hand Clin 1:55, 1985.
- Strickland JW: Flexor tenolysis, Hand Clin 1:121, 1985.
- Strickland JW: Opinions and preferences in fl exor tendon surgery, Hand Clin 1:187, 1985.
- Strickland JW: Results of fl exor tendon surgery in zone II, Hand Clin 1:167, 1985.
- Strickland JW: Flexor tendon injuries: III. Free tendon grafts, Orthop Rev 16:56, 1987.
- Strickland JW: Flexor tendon injuries: IV. Staged fl exor tendon reconstruction and restoration of the fl exor pulley, Orthop Rev 16:78, 1987.
- Strickland JW: Flexor tendon injuries: V. Flexor tenolysis, rehabilitation and results, Orthop Rev 16:137, 1987.
- Strickland JW: Flexor tendon injuries: I. Foundations of treatment, J Am Acad Orthop Surg 3:44, 1995.
- Strickland JW: Flexor tendon injuries: II. Operative techniques, J Am Acad Orthop Surg 3:55, 1995.
- Strickland JW: 25th anniversary presentation. Development of fl exor tendon surgery: twenty-fi ve years of progress, J Hand Surg 25A:214, 2000.
- Tang JB: Flexor tendon repair in zone 2C, J Hand Surg 19B:72, 1994.
- Thurman RT, Trumble TE, Hanel DP, et al: Two-, four-, and six-strand zone II fl exor tendon repairs: an in situ biomechanical comparison using a cadaver model, J Hand Surg 23A:1998.
- Tsuge K, Ikuta Y, Matsuishi Y: Intra-tendinous tendon suture in the hand: a new technique, Hand 7:250, 1975.
- Urbaniak JR: Repair of the fl exor pollicis longus, Hand Clin 1:69, 1985.
- Verdan CE: Practical considerations for primary and secondary repair in fl exor tendon injuries, Surg Clin North Am 44:951, 1964.
- Winters SC, Gelberman RH, Woo SL, et al: The effect of multiple-strand suture methods on the strength and excursion of repaired intrasynovial fl exor tendons: a biomechanical study in dogs, J Hand Surg 23A:97, 1998.
- Wray RC Jr, Holtman B, Weeks PM: Clinical treatment of partial tendon lacerations without suturing and with early motion, Plast Reconstr Surg 59:231, 1977.
- Extensor Tendons Aiache A, Barsky AJ, Weiner DL: Prevention of the boutonniere deformity, Plast Reconstr Surg 46:164, 1970.
- Araki S, Ohtani T, Tanaka T: Acute dislocation of the extensor digitorum communis tendon at the metacarpophalangeal joint, J Bone Joint Surg 69:616, 1987.
- Aulicino PL: Acute injuries of the extensor tendons proximal to the metacarpophalangeal joints, Hand Clin 11:403, 1995.
- Baratz ME, Schmidt CC, Hughes TB: Extensor tendon injuries. In Green DP, Hotchkiss RN, Pederson WC, Wolfe SW, eds: Green’s
You Might Also Like

