Complex Environmental and Ballistic Trauma to the Hand: Shotgun Injuries and Frostbite
Key Takeaway
Shotgun wounds to the upper extremity present complex reconstructive challenges due to clustered shot destruction and wadding contamination. Conversely, frostbite injuries require extreme patience, relying on advanced imaging like Tc-99m bone scans to delineate tissue necrosis before delayed amputation. Both mechanisms demand meticulous, staged surgical protocols, ranging from aggressive early debridement in ballistic trauma to delayed reconstructive interventions for cold-induced physeal arrest in pediatric patients.
COMPLEX TRAUMA OF THE UPPER EXTREMITY: BALLISTIC AND ENVIRONMENTAL INJURIES
The management of severe upper extremity trauma requires a profound understanding of the underlying mechanism of injury, as the energy transfer and physiological insult dictate both the immediate surgical approach and the long-term reconstructive strategy. This chapter comprehensively addresses two distinct but highly destructive mechanisms of hand trauma: close-range shotgun injuries and severe frostbite. While shotgun wounds demand aggressive, immediate surgical intervention to mitigate contamination and stabilize massive tissue disruption, frostbite requires a paradigm of extreme patience, delayed surgical intervention, and meticulous physiological preservation.
SHOTGUN INJURIES TO THE UPPER EXTREMITY
Shotgun injuries represent a unique subset of ballistic trauma. Unlike standard handgun injuries, which typically involve a single projectile, shotgun blasts deliver multiple projectiles (pellets) simultaneously. The severity of a shotgun wound is inversely proportional to the distance between the weapon and the victim.
Ballistics and Pathoanatomy
Shotguns are generally classified as low-velocity weapons (muzzle velocity typically between 1,000 and 1,500 feet per second). However, at close range (less than 3 meters), the clustered shot mass acts as a single, highly destructive projectile. The kinetic energy transfer at close range is massive, resulting in a wound profile that mimics or exceeds that of high-velocity military rifles.
Clinical Pearl: The Sherman and Parrish classification is critical for evaluating shotgun wounds. Type I injuries occur at long range (>7 yards) with scattered pellet penetration and minimal deep tissue damage. Type II injuries (3–7 yards) involve deeper penetration and potential neurovascular injury. Type III injuries (<3 yards) are devastating, characterized by massive tissue avulsion, clustered shot destruction, and severe contamination.
In the upper extremity, Type III close-range injuries are the most common presentation. The clustered shots cause indiscriminate destruction of skin, muscle, tendon, bone, and neurovascular bundles. Furthermore, the skin surrounding the entrance wound is frequently burned by ignited gunpowder and muzzle flash, creating a zone of thermal coagulation that complicates soft tissue viability.
The Danger of Shotgun Wadding
A critical, often overlooked component of shotgun trauma is the introduction of the shotgun shell wadding into the wound bed. The wadding—a cup-like structure usually made of paper, cardboard, or plastic—separates the gunpowder from the pellets within the shell.
At close range, this wadding is propelled directly into the wound tract. It represents a highly dangerous foreign body because it is heavily contaminated with environmental debris, clothing fibers, and skin flora.
Surgical Warning: Shotgun wadding is entirely radiolucent. It will not appear on standard radiographs. The surgeon must maintain a high index of suspicion and meticulously explore the depths of the wound tract to locate and extract the wadding; failure to do so guarantees catastrophic deep space infection.
Surgical Management and Step-by-Step Approach
The management of close-range shotgun injuries to the hand and forearm follows a strict, staged orthopedic trauma protocol.
1. Initial Evaluation and Resuscitation
- Hemorrhage Control: Direct pressure is preferred. Blind clamping in a bloody field is strictly contraindicated due to the high risk of iatrogenic injury to the median, ulnar, or radial nerves.
- Tetanus and Antibiotics: Immediate administration of broad-spectrum intravenous antibiotics (e.g., a first-generation cephalosporin combined with an aminoglycoside) and tetanus prophylaxis.
- Radiographic Assessment: Standard orthogonal views of the affected extremity to assess fracture patterns, joint involvement, and the distribution of radiopaque pellets.
2. Irrigation and Debridement (I&D)
- Tourniquet Control: A pneumatic tourniquet should be applied but inflated only when necessary to identify critical structures or control severe hemorrhage, ensuring the surgeon can accurately assess tissue perfusion.
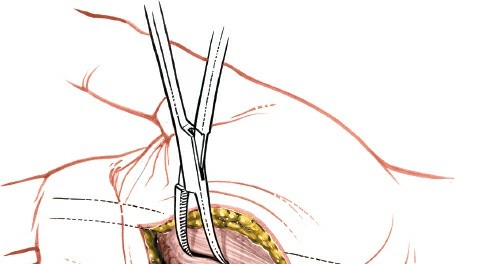
- Wound Extension: The traumatic wound must be extended using standard extensile surgical incisions (e.g., Bruner incisions in the digits) to fully visualize the zone of injury.
- Debridement: All devitalized skin, subcutaneous tissue, and necrotic muscle must be aggressively excised. The "four Cs" of muscle viability (color, consistency, contractility, and capacity to bleed) must be rigorously applied.
- Foreign Body Removal: Meticulous exploration for the radiolucent wadding, clothing fragments, and accessible pellets. Note: It is not necessary to extract every single lead pellet, especially those embedded in vital structures, as the collateral damage of extraction often outweighs the risk of lead retention.
3. Skeletal Stabilization
- Once the wound is adequately debrided, skeletal stability must be restored to protect repaired soft tissues and prevent further neurovascular compromise.
- Depending on the degree of bone loss and contamination, stabilization may be achieved via percutaneous Kirschner wires (K-wires), external fixation, or, less commonly in the acute contaminated setting, internal plate osteosynthesis.
- Spanning external fixators are highly effective for massive segmental bone loss in the forearm or wrist.
4. Soft Tissue Coverage and Postoperative Protocol
- Delayed Primary Closure: The wound should never be closed primarily. It must be packed with sterile dressings or managed with Negative Pressure Wound Therapy (NPWT).
- Second-Look Surgery: The patient must return to the operating room within 48 to 72 hours for a planned second-look debridement.
- Reconstruction: Once the wound bed is pristine, definitive coverage is achieved. Depending on the extent of tissue loss, this may require split-thickness skin grafts, pedicled regional flaps (e.g., radial forearm flap, groin flap), or free tissue transfer (e.g., anterolateral thigh flap).
FROSTBITE INJURIES OF THE HAND
In stark contrast to the immediate, aggressive surgical demands of ballistic trauma, frostbite requires a highly conservative, delayed surgical approach. Frostbite is a severe localized cold-induced injury characterized by tissue freezing and subsequent microvascular collapse.
Pathophysiology of Cold Injury
The destruction of tissue in frostbite occurs via two primary mechanisms:
1. Direct Cellular Toxicity: As tissue temperatures drop below freezing, extracellular ice crystals form. This creates an osmotic gradient that draws water out of the cells, leading to intracellular dehydration, protein denaturation, and cell death.
2. Microvascular Thrombosis: The indirect, and often more devastating, injury occurs during the thawing phase. Endothelial damage leads to the release of inflammatory mediators (such as thromboxane A2 and prostaglandins), causing severe vasoconstriction, platelet aggregation, and ultimately, microvascular thrombosis. This progressive ischemia leads to the demarcation of necrotic tissue over several weeks.
Acute Management and Resuscitation
The initial treatment of frostbite dictates the long-term survival of the affected digits.
* Rapid Rewarming: The core tenet of acute management is rapid rewarming in a circulating water bath maintained precisely between 37°C and 39°C (98.6°F - 102.2°F). Rewarming should continue until the distal capillary bed flushes (usually 15 to 30 minutes).
* Medical Therapy: To combat microvascular thrombosis, patients are typically started on a regimen of systemic ibuprofen (to inhibit the arachidonic acid cascade and thromboxane production) and topical aloe vera (to inhibit local prostaglandin synthesis). In severe cases presenting within 24 hours of injury, intra-arterial thrombolytic therapy (e.g., tPA) may be considered to salvage at-risk digits.
The Principle of Delayed Amputation
Surgical Warning: In contrast to thermal burns, there is absolutely no place for early excision and grafting in the treatment of frostbite. The classic surgical adage remains paramount: "Freeze in January, amputate in July."
Early surgical intervention in frostbite is fraught with complications because the initial clinical appearance of the tissue is highly deceptive. Tissues that appear completely non-viable in the first week may recover, while seemingly healthy tissues may succumb to progressive microvascular thrombosis.
Amputation must be delayed until there is a definitive, undeniable line of demarcation between viable and necrotic tissue. This process often requires several weeks to a few months. During this waiting period, the necrotic tissue will mummify. The patient must be managed with frequent, gentle washings (whirlpool therapy), meticulous local wound care to prevent secondary bacterial infection, and an organized program of hand therapy to maintain joint mobility in the uninjured proximal segments.
Advanced Imaging for Tissue Demarcation
While clinical observation is the gold standard for determining the final level of amputation, advanced radiographic techniques can be highly beneficial in predicting tissue viability and planning reconstructive procedures.
- Technetium-99m (Tc-99m) Bone Scanning: A Tc-99m–labeled methylene diphosphonate bone scan performed 48 to 72 hours post-injury is highly sensitive for assessing microvascular perfusion. Areas devoid of uptake correlate strongly with eventual tissue necrosis.
- Magnetic Resonance Imaging (MRI) and Magnetic Resonance Angiography (MRA): These modalities provide high-resolution mapping of the vascular tree and soft tissue viability, aiding the surgeon in identifying the exact level of demarcation prior to surgical intervention.
Soft Tissue Reconstruction
When demarcation is complete and surgical amputation is performed, the goal is to preserve maximal functional length of the digits. If there is extensive soft tissue loss but viable underlying bone and tendon, complex coverage may be required. This can include:
* Skin Grafts: For superficial defects with a healthy, vascularized wound bed.
* Pedicle Skin Flaps: Cross-finger flaps or thenar flaps for exposed bone or tendon in the digits.
* Free Tissue Transfer: For massive soft tissue deficits requiring robust, vascularized coverage to salvage functional length.
PEDIATRIC CONSIDERATIONS: FROSTBITE AND PHYSEAL ARREST
Frostbite in the pediatric population presents a unique and devastating complication: premature physeal arrest. The epiphyseal growth plate (physis) is exquisitely sensitive to cold injury, far more so than the surrounding skin, muscle, or mature bone.
Pathoanatomy of Cold-Induced Physeal Arrest
In children, severe frostbite can cause direct chondrocyte necrosis within the physis, leading to premature closure of the growth plate. This complication has a distinct anatomical predilection:
* The index and little fingers are involved most frequently.
* The middle and ring fingers are involved less frequently.
* The thumb is involved least of all, likely due to its protected position clutched within the palm during cold exposure.
The disturbance in longitudinal growth does not manifest immediately; rather, it develops gradually over months to years as the child grows. The affected digits become progressively shortened, and asymmetric physeal closure can lead to severe angular deformities (clinodactyly). Radiographically, the epiphyses may appear fragmented, sclerotic, or completely destroyed, often resulting in premature fusion and cone-shaped epiphyses.

Clinical Radiograph: Deformities of the fingers in a 12-year-old girl caused by severe frostbite incurred at age 2 years. Note the profound destruction of the epiphyses of the middle and distal phalanges across all fingers, and the severe angular deformity of the epiphysis of the proximal phalanx of the little finger. The osseous changes demonstrate the classic delayed manifestation of cold-induced physeal arrest.
Long-Term Management of Pediatric Deformities
The management of cold-induced physeal arrest requires long-term, longitudinal follow-up.
Clinical Pearl: Corrective surgical procedures for angular deformities or digit lengthening should be delayed as long as possible, ideally until the child approaches skeletal maturity. Early osteotomies carry a high risk of recurrence as the surrounding normal tissues continue to grow.
When surgical intervention is ultimately indicated, procedures may include:
* Corrective Osteotomies: To realign angular deformities and restore the mechanical axis of the digit.
* Distraction Osteogenesis: Utilizing miniature external fixators to gradually lengthen the severely shortened phalanges, thereby improving both the functional span of the hand and its cosmetic appearance.
* Epiphysiodesis: In rare cases of severe asymmetry, surgical arrest of the contralateral or adjacent normal growth plates may be considered to achieve digital symmetry, though this is generally avoided in the hand where length is critical for grip mechanics.
Conclusion
Whether managing the acute, chaotic destruction of a close-range shotgun blast or the insidious, progressive necrosis of severe frostbite, the orthopedic surgeon must rely on a foundation of strict physiological principles. Shotgun injuries demand immediate, aggressive debridement and a high suspicion for radiolucent foreign bodies. Conversely, frostbite requires immense patience, reliance on advanced perfusion imaging, and a delayed approach to amputation. In both scenarios, the ultimate goal remains the preservation of maximal functional anatomy and the meticulous restoration of the complex biomechanics of the human hand.
You Might Also Like