Stenosing Tenosynovitis and De Quervain Disease: A Surgical Masterclass
Key Takeaway
Stenosing tenosynovitis of the first dorsal compartment, known as De Quervain disease, involves the abductor pollicis longus and extensor pollicis brevis tendons. Pathological friction at the extensor retinaculum causes debilitating radial-sided wrist pain. While corticosteroid injections provide relief in up to 70% of cases, refractory pathology requires surgical release. Successful operative management demands meticulous identification of anatomical variations, including aberrant tendon slips and septated subcompartments, to prevent persistent postoperative symptoms.
STENOSING TENOSYNOVITIS: PATHOPHYSIOLOGY AND BIOMECHANICS
Stenosing tenosynovitis is a ubiquitous orthopedic pathology that occurs more frequently in the hand and wrist than anywhere else in the human body. The fundamental biomechanical etiology lies in the discrepancy between the volume of a tendon (or tendons) and the unyielding fibro-osseous tunnel through which it must glide.
The stenosis typically manifests at anatomical fulcrums—points where the direction of a tendon changes abruptly. At these critical junctures, a fibrous sheath acts as a biological pulley, maximizing friction during tendon excursion. Although the tenosynovium is designed to lubricate the sheath and facilitate smooth gliding, repetitive mechanical overload, friction, and microtrauma can precipitate a reactive cascade. This is frequently observed in occupations or activities requiring repetitive, forceful gripping, ulnar deviation, or fine motor repetitions (e.g., winding a fine coil of wire, stacking laundry, or prolonged typing).
Histologically, the condition is often more accurately described as a tenovaginitis or tendinosis rather than a pure tenosynovitis. The primary pathological finding is fibrocartilaginous metaplasia and thickening of the extensor retinaculum or flexor pulley, rather than acute inflammatory infiltrates within the synovium.
While the first dorsal compartment is the most famous site of this pathology, stenosing tenosynovitis can affect various regions:
* Flexor Tendons: Resulting in trigger thumb, trigger finger, or snapping finger (stenosis at the A1 pulley).
* Extensor Pollicis Longus (EPL): Occasionally affected at the level of Lister’s tubercle (third dorsal compartment), particularly following distal radius fractures.
* Other Dorsal Compartments: Any tendon passing beneath the dorsal wrist retinaculum is susceptible, including the extensor carpi ulnaris (sixth compartment).
The tenosynovitis that precedes frank stenosis may be idiopathic, but it can also result from subclinical collagen vascular diseases, inflammatory arthropathies (such as rheumatoid arthritis), or recurrent mild trauma. In some clinical histories, a single acute traumatic event may initiate the pathological cascade, whereas in others, the condition develops insidiously over months or years.
Clinical Pearl: Before initiating treatment, particularly corticosteroid injections, the clinician must definitively rule out other causes of tenosynovial inflammation, such as crystalline arthropathies (gout, pseudogout) or atypical mycobacterial infections, which could be catastrophically exacerbated by localized immunosuppression.
DE QUERVAIN DISEASE
When stenosing tenosynovitis affects the extensor pollicis brevis (EPB) and the abductor pollicis longus (APL) tendons within the first dorsal compartment of the wrist, the condition is eponymously named after the Swiss physician Fritz de Quervain, who first described his clinical experience with the disorder in 1895.
Epidemiology and Clinical Presentation
De Quervain disease typically afflicts adults between the ages of 30 and 50 years. There is a striking gender predilection, with women being affected six to ten times more frequently than men. The etiology is almost universally related to cumulative microtrauma and overuse—often associated with new occupational demands or the repetitive lifting of infants (frequently termed "baby wrist" or "mommy thumb" in postpartum women). It is also a common concomitant finding in patients with rheumatoid arthritis.
Patients classically present with insidious or acute-onset pain and tenderness localized to the radial styloid. The pain is exacerbated by thumb motion, particularly combined thumb flexion and ulnar deviation of the wrist. On physical examination, a palpable, firm thickening of the fibrous sheath over the radial styloid is frequently appreciated. In severe cases, a peritendinitis may extend proximal to the extensor retinaculum, causing visible swelling, erythema, and palpable crepitus during tendon excursion.
Diagnostic Evaluation
The cornerstone of physical diagnosis is the Finkelstein test. As originally described, the test is performed by "grasping the patient’s thumb and quickly abducting the hand ulnarward." In a positive test, the pain elicited over the radial styloid tip is excruciating.
Diagnostic Pitfall: Although Finkelstein historically stated that this test is "probably the most pathognomonic objective sign," modern orthopedic practice recognizes that it is not strictly diagnostic in isolation. False positives can occur, and the test must be interpreted within the broader clinical context.
A comprehensive differential diagnosis must be systematically evaluated. Similar radial-sided wrist pain can be generated by:
1. Osteoarthritis: Trapeziometacarpal (CMC) joint arthritis or scaphotrapeziotrapezoid (STT) joint arthritis. (Differentiated by a positive CMC grind test and radiographic findings).
2. Intersection Syndrome: Tenosynovitis at the crossing point where the EPB and APL muscle bellies cross over the extensor carpi radialis longus (ECRL) and brevis (ECRB) tendons, typically located 4 to 5 cm proximal to the radial styloid.
3. Wartenberg’s Syndrome: Entrapment or neuritis of the superficial branch of the radial nerve (SRN). (Differentiated by a positive Tinel’s sign over the nerve and dysesthesia in the dorsal web space).
4. Radiocarpal Pathology: Occult ganglia, scaphoid nonunions, or radiocarpal arthritis.
CONSERVATIVE MANAGEMENT
The initial management of De Quervain disease is non-operative, focusing on reducing mechanical friction and suppressing the localized reactive tissue response. Early intervention yields the highest success rates.
Conservative modalities include:
* Immobilization: A forearm-based thumb spica splint that immobilizes both the wrist and the thumb interphalangeal/metacarpophalangeal joints to eliminate tendon excursion.
* Pharmacotherapy: Oral nonsteroidal anti-inflammatory drugs (NSAIDs) may provide symptomatic relief, though they do not alter the underlying mechanical stenosis.
* Corticosteroid Injections: The gold standard of non-operative treatment.
Corticosteroid Injection Technique
Many cases of stenosing tenosynovitis respond highly favorably to a targeted injection of a corticosteroid preparation mixed with a local anesthetic. Initial treatment with a properly placed steroid injection can yield complete, long-lasting pain relief in over 70% of patients.
FIGURE 76-13: Injection technique for De Quervain tenosynovitis. The needle is directed into the first dorsal compartment, taking care to avoid the superficial radial nerve.
Injection Protocol and Patient Counseling:
1. Identify the first dorsal compartment and the borders of the APL and EPB.
2. A 25- or 27-gauge needle is introduced at a shallow angle, directing the injectate into the tendon sheath rather than the tendon substance.
3. If a septation is suspected (e.g., fluid does not flow easily or only one tendon sheath distends), a two-point injection or ultrasound-guided injection may be necessary to ensure both the APL and EPB subcompartments are treated.
4. Patient Warning: Patients must be explicitly warned that pain may temporarily increase during the initial 24 to 48 hours following the dissipation of the local anesthetic effect (steroid flare). It typically requires 3 to 7 days before the anti-inflammatory effect of the steroid becomes clinically apparent.
When conservative measures fail and debilitating pain persists beyond 3 to 6 months, surgical release is the definitive treatment of choice.
SURGICAL ANATOMY AND PATHOLOGICAL VARIATIONS
The surgical management of De Quervain disease is conceptually simple but anatomically treacherous. The primary reason for surgical failure or persistent postoperative pain is the failure to recognize and adequately release anatomical variations within the first dorsal compartment.
The First Dorsal Compartment
The first dorsal compartment is bounded volarly by the radial styloid and dorsally by the extensor retinaculum. It contains the tendons of the Abductor Pollicis Longus (APL) and the Extensor Pollicis Brevis (EPB).
Anatomical variations are the rule rather than the exception. Separate compartments (septations) dividing the APL and EPB have been noted in 21% of anatomical cadaveric specimens. However, in surgical series of patients presenting with De Quervain disease, the incidence of a separate EPB compartment is significantly higher, reported to be between 20% and 58%. This suggests that septation itself may be a predisposing anatomical factor for the development of the disease.
Aberrant and Duplicated Tendons
More than half of all patients possess "aberrant" or duplicated tendons, most commonly involving the APL. The APL frequently consists of multiple tendon slips (ranging from two to five).
These aberrant slips often insert more proximally and medially than the standard insertion at the base of the first metacarpal. Common variant insertions include:
* The trapezium.
* The abductor pollicis brevis (APB) muscle.
* The opponens pollicis muscle.
* The surrounding thenar muscle fascia.
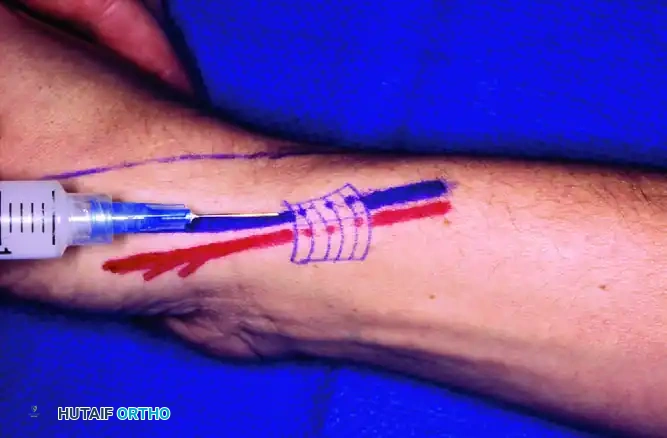
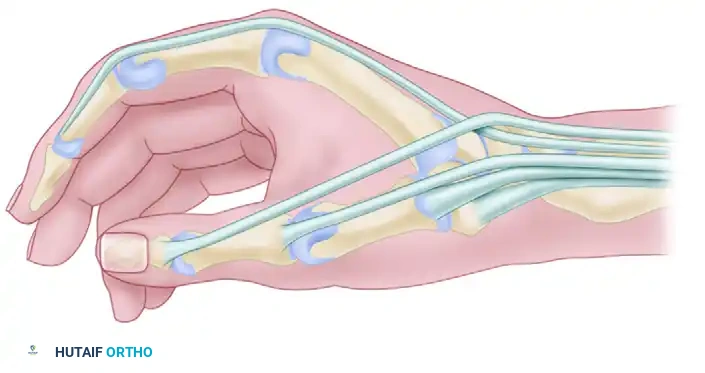
FIGURE 76-14: Often, the abductor pollicis longus inserts on the trapezium and the base of the first metacarpal through two distinct tendons. During surgery for De Quervain disease, at least one aberrant tendon is frequently encountered.
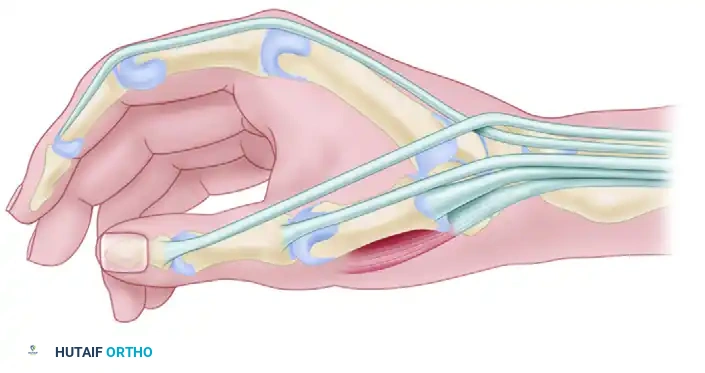
FIGURE 76-15: In rare anatomical variants, a slip of the abductor pollicis longus inserts directly onto the fascia of the abductor pollicis brevis and the base of the first metacarpal.
Conversely, the EPB is considered a "late" tendon phylogenetically and is completely absent in approximately 5% of wrists.
Surgical Warning: The presence of these variations—specifically a separate fibro-osseous tunnel for the EPB—must be actively sought during surgery. Failure to identify and release an isolated EPB compartment is the leading cause of revision surgery in De Quervain disease.
SURGICAL TECHNIQUE: FIRST DORSAL COMPARTMENT RELEASE
Surgical release of the first dorsal compartment is typically performed on an outpatient basis under local anesthesia (WALANT - Wide Awake Local Anesthesia No Tourniquet) or regional block with a proximal tourniquet. WALANT is highly advantageous as it allows the surgeon to ask the patient to actively move their thumb intraoperatively, confirming complete release of all tendon slips.
Step 1: Incision and Superficial Dissection
The skin incision can be made either transversely or longitudinally.
* Transverse Incision: Follows Langer’s lines, providing superior cosmesis and reducing the risk of a hypertrophic scar. However, it limits proximal-distal exposure.
* Longitudinal Incision: Provides excellent exposure of the retinaculum but crosses skin creases, increasing the risk of scar contracture.

FIGURE 76-16 A: A transverse or slightly oblique skin incision is made over the first dorsal compartment, carefully positioned to avoid major branches of the superficial radial nerve.
Following skin incision, blunt dissection is strictly utilized in the subcutaneous tissues. The superficial branch of the radial nerve (SRN) arborizes directly over the first dorsal compartment. Injury to the SRN, either via direct transection or aggressive traction causing a neuropraxia/neuroma, is a devastating complication that can leave the patient with chronic, intractable neuropathic pain far worse than the original De Quervain disease. The nerve branches must be identified, gently mobilized, and protected with blunt retractors.
Step 2: Exposure of the Extensor Retinaculum
Once the subcutaneous tissues and nerve branches are safely retracted, the thickened extensor retinaculum (dorsal carpal ligament) overlying the first compartment is exposed.

FIGURE 76-16 B: The superficial radial nerve branches are protected, and the thickened dorsal carpal ligament (extensor retinaculum) is fully exposed.
Step 3: Incision of the Compartment
The retinaculum is incised longitudinally.
Surgical Pearl: The incision through the retinaculum should be made along its dorsal (ulnar) margin. If the retinaculum is incised too volarly, the APL and EPB tendons may subluxate volarly over the radial styloid during wrist flexion and thumb abduction, creating a painful snapping sensation postoperatively.

FIGURE 76-16 C: The first dorsal compartment has been opened longitudinally on its ulnar (dorsal) side to prevent postoperative volar tendon subluxation.
Step 4: Exploration for Septations and Aberrant Tendons
Once the main compartment is opened, the surgeon must meticulously inspect the contents. The APL (usually multiple slips, larger, and more volar) and the EPB (usually a single slip, smaller, and more dorsal) must be individually identified.
The surgeon must actively search for a pale, fibrous septum separating the EPB from the APL. If a septum is found, it must be completely excised to unroof the EPB subcompartment.
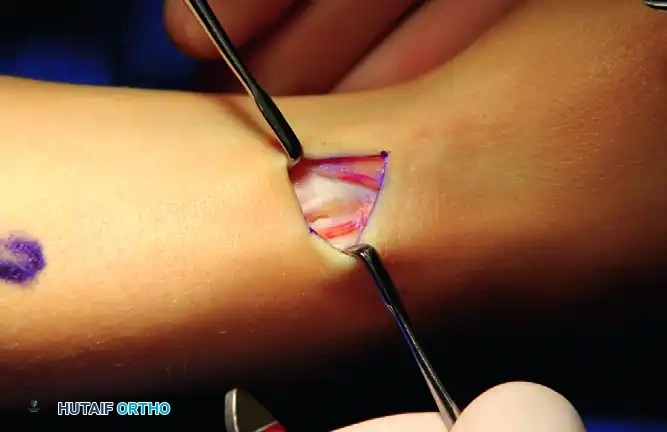
FIGURE 76-16 D: Exploration reveals separate compartments. The septum between the extensor pollicis brevis and the abductor pollicis longus tendons must be identified and excised to ensure complete decompression.
To confirm complete release, the surgeon should apply traction to the individual tendons. Traction on the EPB should produce isolated extension of the thumb metacarpophalangeal (MCP) joint. Traction on the APL slips should produce abduction of the thumb carpometacarpal (CMC) joint. If WALANT anesthesia is used, the patient is asked to actively flex and extend the thumb to confirm smooth, unhindered gliding of all tendon slips.
Step 5: Closure
The wound is thoroughly irrigated. The retinaculum is left open; it is never repaired, as doing so would recreate the stenosis. Only the skin is closed using non-absorbable monofilament sutures (e.g., 5-0 or 6-0 nylon) or absorbable sutures depending on surgeon preference. A bulky, soft compressive dressing is applied, leaving the thumb interphalangeal joint free.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Postoperative management focuses on minimizing edema, preventing adhesions, and restoring normal kinematics to the thumb and wrist.
- Immediate Postoperative Phase (Days 0-10): The wrist is supported in a soft dressing or a removable volar splint. Patients are strongly encouraged to begin immediate, gentle active range of motion (ROM) of the thumb and fingers to prevent tendon adhesions and stiffness. Elevation and ice are utilized to control edema.
- Suture Removal (Days 10-14): Sutures are removed. Scar massage is initiated to prevent tethering of the skin to the underlying tendons or the superficial radial nerve.
- Strengthening Phase (Weeks 3-6): Progressive strengthening of the thumb and wrist is introduced. Most patients return to full, unrestricted activities by 4 to 6 weeks postoperatively.
Complications
While surgical release is highly successful, complications can occur and must be discussed during preoperative informed consent:
* Superficial Radial Nerve Injury: The most severe complication, leading to painful neuromas and complex regional pain syndrome (CRPS).
* Incomplete Release: Failure to recognize a septated EPB compartment leads to persistent pain and necessitates revision surgery.
* Tendon Subluxation: Caused by excessive volar release of the retinaculum. If symptomatic, it may require complex retinacular reconstruction using a slip of the extensor retinaculum or local fascia.
* Hypertrophic Scarring: More common with longitudinal incisions crossing the wrist creases.
By adhering to strict anatomical principles, respecting the superficial radial nerve, and meticulously identifying all tendon slips and septations, the orthopedic surgeon can achieve excellent, reproducible outcomes in the management of De Quervain stenosing tenosynovitis.
📚 Medical References
- de Quervain Disease Abe Y, Tsue K, Nagai E, et al: Extensor pollicis longus tenosynovitis mimicking de Quervain’s disease because of its course through the fi rst extensor compartment: a report of 2 cases, J Hand Surg 29A:225, 2004.
- Alexander RD, Catalano LW, Barron OA, et al: The extensor pollicis brevis entrapment test in the treatment of de Quervain’s disease, J Hand Surg 27A:813, 2002.
- Christie BGB: Local hydrocortisone in deQuervain’s disease, BMJ 1:1501, 1955.
- Finkelstein H: Stenosing tendovaginitis at the radial styloid process, J Bone Joint Surg 12:509, 1930.
- Harvey FJ, Harvey PM, Horsley MW: de Quervain’s disease: surgical or nonsurgical treatment, J Hand Surg 15A:83, 1990.
- Kay NR: de Quervain’s disease: changing pathology or changing perception? J Hand Surg 25B:65, 2000.
- Keon-Cohen B: de Quervain’s disease, J Bone Joint Surg 33B:96, 1951.
- Lane LB, Boretz RS, Stuchin SA: Treatment of de Quervain’s disease: role of conservative management, J Hand Surg 26B:258, 2001.
- Lapidus PW, Guidotti FP: Stenosing tenovaginitis of the wrist and fi ngers, Clin Orthop Relat Res 83:87, 1972.
- Leão L: De Quervain’s disease: a clinical and anatomical study, J Bone Joint Surg 40A:1063, 1958.
- Littler JW, Freedman DM, Malerich MM: Compartment reconstruction for de Quervain’s disease, J Hand Surg 27B:242, 2002.
- McMahon M, Craig SM, Posner MA: Tendon subluxation after de Quervain’s release: treatment by brachioradialis tendon fl ap, J Hand Surg 16A:30, 1991.
- Moore JS: de Quervain’s tenosynovitis:
You Might Also Like