Approaches Posterolateral Surgical: A Guide to Enhanced Hip Surgery

Key Takeaway
Here are the crucial details you must know about Approaches Posterolateral Surgical: A Guide to Enhanced Hip Surgery. The approaches posterolateral surgical technique for total hip arthroplasty provides comprehensive exposure of the proximal femur and acetabulum. This method, used in total hip replacement, aims for reduced tissue trauma, enhanced posterior soft tissue repair, and multimodal pain management. Patients are positioned in lateral decubitus for this effective orthopaedic procedure.
Introduction and Epidemiology
Total hip arthroplasty is universally recognized as one of the most successful and cost-effective surgical interventions in modern medicine, providing reliable pain relief and functional restoration for patients with end-stage hip pathology. The historical evolution of surgical access to the hip joint has seen numerous iterations. Sir John Charnley initially popularized the transtrochanteric approach for his low friction arthroplasty, which, while providing excellent exposure, was fraught with complications related to trochanteric nonunion and hardware failure. Subsequently, various other approaches were introduced and refined, including the anterior (Smith-Petersen), lateral (Hardinge), anterolateral (Watson-Jones), and posterior (Gibson and Moore) approaches.
The posterolateral approach, often associated with the classic Southern approach described by Austin Moore, remains the most widely utilized surgical approach for total hip arthroplasty globally. Its enduring popularity stems from its extensile nature, preservation of the hip abductor mechanism, and excellent visualization of both the proximal femur and the acetabulum. The current trend in arthroplasty emphasizes tissue-sparing techniques; however, visualization of surrounding anatomic landmarks remains paramount for proper spatial orientation and precise component positioning. Attempts to perform surgery through an inadequately small skin incision without proper visualization may lead to component malposition, unrecognized soft tissue damage, and higher complication rates, ultimately compromising the clinical longevity of the procedure.

Epidemiologically, the demand for total hip arthroplasty continues to rise exponentially, driven by an aging population and expanding indications in younger, highly active patients. Osteoarthritis remains the primary indication, accounting for the vast majority of cases, followed by avascular necrosis, inflammatory arthropathies, and post-traumatic arthritis. The posterolateral approach is particularly advantageous in complex primary and revision scenarios due to its extensile utility, allowing for proximal femoral osteotomies or extended trochanteric osteotomies when required.
Surgical Anatomy and Biomechanics
A profound understanding of the posterior hip anatomy is critical for safe execution of the posterolateral approach. Unlike the direct anterior approach, which utilizes a true internervous plane (between the femoral nerve-innervated sartorius/rectus femoris and superior gluteal nerve-innervated tensor fasciae latae), the posterolateral approach does not employ a true internervous plane. Instead, it involves a muscle-splitting dissection through the gluteus maximus, which is innervated by the inferior gluteal nerve.
The superficial dissection splits the fascia lata and the gluteus maximus in line with its fibers. Deep to the gluteus maximus lies the crucial layer of the short external rotators: the piriformis, superior gemellus, obturator internus, inferior gemellus, obturator externus, and quadratus femoris. These structures serve as dynamic stabilizers of the hip joint. The piriformis tendon, inserting on the piriformis fossa of the greater trochanter, is a key anatomical landmark.

The sciatic nerve is the most critical neurovascular structure encountered during this approach. It typically exits the pelvis through the greater sciatic foramen, inferior to the piriformis muscle. However, anatomical variants exist, such as the nerve piercing the piriformis or exiting superior to it. The nerve lies posterior to the short external rotators, which act as a protective buffer during the initial deep dissection. Retractors placed posteriorly must be positioned carefully to avoid compression or traction injuries to the sciatic nerve.

Vascular anatomy demands meticulous attention, particularly the medial circumflex femoral artery. This vessel typically traverses the operative field near the inferior border of the quadratus femoris. While modern techniques often spare the quadratus femoris or only release its superior portion, inadvertent injury to the medial circumflex femoral artery can result in significant postoperative hematoma.

Biomechanically, the posterolateral approach preserves the gluteus medius and minimus, ensuring postoperative abductor strength and minimizing the risk of a Trendelenburg gait. Restoration of femoral offset and leg length is achieved through precise preoperative templating and intraoperative trialing. The primary biomechanical vulnerability of this approach is the disruption of the posterior capsuloligamentous complex, which historically led to higher dislocation rates. This has been largely mitigated by the adoption of enhanced posterior soft tissue repair techniques.
Indications and Contraindications
The posterolateral approach is highly versatile and is indicated for a broad spectrum of hip pathologies. Its extensile nature makes it suitable for both routine primary arthroplasty and complex reconstructions.

Primary indications include end-stage degenerative joint disease, avascular necrosis of the femoral head, displaced femoral neck fractures in the elderly, and developmental dysplasia of the hip. The approach is particularly favored in cases requiring extensive femoral exposure, such as the removal of pre-existing hardware or the management of proximal femoral deformity.

Contraindications are generally related to patient-specific factors rather than the approach itself. However, relative contraindications for the posterolateral approach may include patients with profound neuromuscular disorders (e.g., Parkinson's disease, severe cerebral palsy) or severe cognitive impairment, where compliance with postoperative posterior hip precautions cannot be guaranteed, thereby elevating the risk of posterior dislocation.
| Clinical Scenario | Operative Indication Status | Rationale and Approach Considerations |
|---|---|---|
| Primary Osteoarthritis | Absolute Indication | Standard application of posterolateral approach; allows excellent visualization for standard component placement. |
| Displaced Femoral Neck Fracture | Absolute Indication | Rapid exposure for hemiarthroplasty or total hip arthroplasty; easily extensile if fracture extension is noted. |
| Active Joint Infection | Absolute Contraindication | Eradication of infection via staged procedures is required prior to definitive arthroplasty. |
| Severe Neuromuscular Disease | Relative Contraindication | High risk of posterior dislocation; consider direct anterior approach or use of dual-mobility components if posterolateral is utilized. |
| Hardware Retained in Proximal Femur | Strong Indication | Posterolateral approach provides superior access for hardware removal (e.g., dynamic hip screws) concurrent with arthroplasty. |
Pre Operative Planning and Patient Positioning
Thorough preoperative clinical evaluation and radiographic templating are mandatory. Meticulous preoperative planning is performed on standardized anteroposterior radiographic views of the pelvis and a cross-table lateral view of the affected hip. Templating facilitates the estimation of component sizes, determination of the anatomical center of rotation, assessment of femoral offset, and planning for leg length equalization.

Regional anesthesia, specifically spinal or epidural hypotensive anesthesia, is preferred over general anesthesia. Neuraxial anesthesia minimizes intraoperative blood loss by lowering venous pressure, thereby facilitating visualization, and reduces the risk of postoperative deep vein thrombosis. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within one hour prior to surgical incision. Tranexamic acid is routinely utilized unless contraindicated to further minimize blood loss.
Patient positioning is a critical determinant of surgical success, particularly regarding acetabular component orientation. The patient is placed in the lateral decubitus position with the affected hip facing superiorly on a rigid operating table.

The pelvis must be rigidly secured to prevent shifting during the procedure. This is achieved using padded posts placed anteriorly against the pubic symphysis and posteriorly against the sacrum. The patient's longitudinal axis must be strictly parallel to the operating table, and the coronal plane of the pelvis must be perfectly perpendicular to the floor. Any unrecognized pelvic tilt or roll will directly translate into errors in acetabular cup version and inclination.
All bony prominences, particularly the dependent fibular head and axilla, are meticulously padded to prevent compressive neuropathies. The operating table should allow for intraoperative tilting (airplane function) to facilitate acetabular reaming and component insertion if necessary.

Standard surgical preparation and draping are performed to ensure a wide sterile field, allowing full manipulation of the operative extremity.
Detailed Surgical Approach and Technique
The surgical technique for the posterolateral approach must be executed with precision to optimize exposure while minimizing soft tissue trauma.

The incision is typically curvilinear, centered over the posterior third of the greater trochanter. It extends proximally toward the posterior superior iliac spine and distally along the axis of the femoral shaft. The length of the incision is dictated by patient anatomy (e.g., BMI) and the complexity of the reconstruction, adhering to the principle that adequate visualization supersedes the cosmetic appeal of a small incision.

Subcutaneous tissues are divided in line with the skin incision to expose the fascia lata and the gluteal fascia. The fascia lata is incised distally over the greater trochanter, and this incision is carried proximally to split the fibers of the gluteus maximus bluntly. A Charnley or similar self-retaining retractor is placed to maintain exposure of the deep structures.
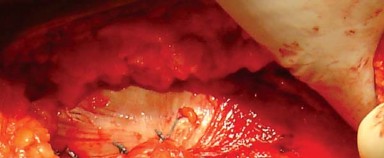
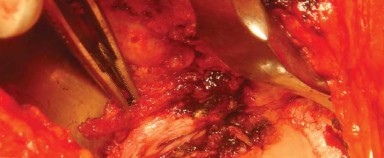
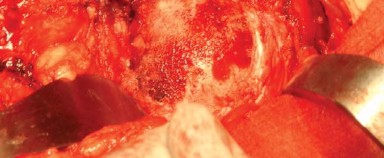
The bursa overlying the greater trochanter and the short external rotators is excised to clearly define the anatomy. The posterior border of the gluteus medius is identified and retracted superiorly and anteriorly. The piriformis tendon and the conjoined tendon of the obturator internus and gemelli are identified.
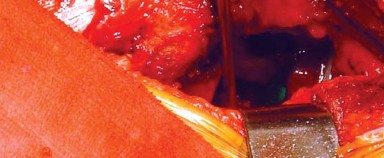
To preserve the vascularity and integrity of the posterior structures for later repair, the short external rotators and the posterior joint capsule are often elevated as a single, continuous full-thickness flap. Stay sutures are placed in this capsulotendinous flap before it is sharply detached from its insertion at the base of the greater trochanter. This flap is then reflected posteriorly, protecting the underlying sciatic nerve from direct trauma and retractor pressure.

Dislocation of the hip is achieved through a combination of flexion, adduction, and internal rotation of the operative limb. Care must be taken to avoid excessive torsional forces that could result in an iatrogenic femoral shaft fracture, particularly in osteoporotic bone.
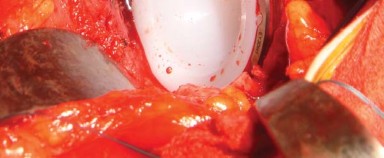
Once dislocated, the femoral neck is exposed, and the planned osteotomy is performed using an oscillating saw. The level and angle of the osteotomy are determined based on preoperative templating and intraoperative landmarks, typically measured from the lesser trochanter.

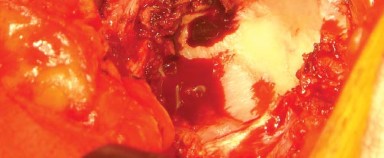
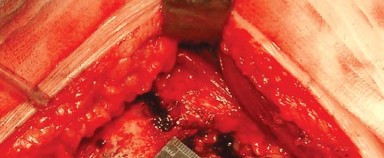
Following removal of the femoral head, attention is directed to the acetabulum. Excellent exposure is paramount. A blunt or Cobra retractor is placed anteriorly over the anterior column, carefully avoiding the femoral neurovascular bundle. A second retractor is placed inferiorly beneath the transverse acetabular ligament, and a third is placed posteriorly to retract the femur anteriorly.

The acetabular labrum and pulvinar are excised to expose the true medial wall (cotyloid fossa). Reaming is initiated with a small reamer directed medially to establish the depth of the center of rotation, followed by sequential reaming to expand the hemisphere.
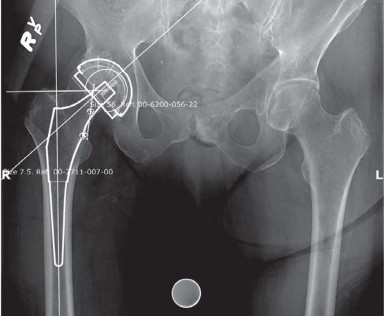
The definitive acetabular component is impacted into place, targeting an inclination of 40 to 45 degrees and an anteversion of 15 to 20 degrees. Adjunctive screw fixation may be utilized depending on the initial press-fit stability and bone quality.
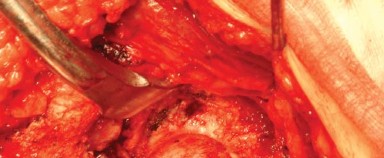
Attention is then returned to the femur. The proximal femur is elevated and supported using a specialized elevator. The femoral canal is accessed using a box osteotome or canal finder, ensuring a lateralized starting point in the piriformis fossa or greater trochanter to prevent varus malposition of the stem.

Sequential broaching is performed until rotational stability and appropriate cortical contact are achieved. A trial neck and head are placed, and the hip is reduced.

A comprehensive assessment of stability, offset, and leg length is conducted. Stability is tested dynamically by taking the hip through a full range of motion, specifically checking for impingement in combined flexion, adduction, and internal rotation (the position of instability for the posterior approach).

Once optimal trialing is confirmed, the hip is dislocated, trial components are removed, and the definitive femoral stem and head are implanted.

The final reduction is performed, and the operative site is thoroughly irrigated to remove any particulate debris.

Closure is a critical phase of the posterolateral approach. An enhanced posterior soft tissue repair is mandatory to restore dynamic stability and minimize dislocation risk. The capsulotendinous flap is advanced and repaired to its anatomical insertion site on the greater trochanter using heavy non-absorbable sutures, often utilizing transosseous tunnels or specialized anchors.
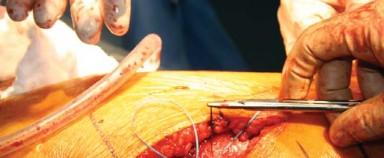
The split in the gluteus maximus and fascia lata is closed meticulously, followed by standard closure of the subcutaneous tissues and skin.
Complications and Management
While total hip arthroplasty via the posterolateral approach is highly successful, specific complications can arise that require prompt recognition and expert management.

Posterior dislocation is historically the most scrutinized complication associated with this approach. The mechanism typically involves excessive flexion, adduction, and internal rotation. The incidence has dramatically decreased with the advent of larger femoral head sizes (32mm, 36mm, and larger) and the routine implementation of enhanced posterior soft tissue repair techniques. Management of a first-time dislocation generally involves closed reduction under conscious sedation, followed by a period of strict adherence to hip precautions. Recurrent instability requires a thorough evaluation of component position, soft tissue tension, and abductor function, often necessitating revision arthroplasty to correct malversion or utilize constrained/dual-mobility liners.

Sciatic nerve palsy is a devastating complication, manifesting primarily as a foot drop (peroneal division involvement). It can result from direct mechanical trauma, excessive retractor pressure, or significant leg lengthening. Intraoperative vigilance regarding retractor placement is essential. If a postoperative palsy is identified, immediate assessment for an expanding hematoma is required. If a hematoma is present, emergent evacuation is indicated. Otherwise, management is supportive with an ankle-foot orthosis (AFO) and physical therapy, with variable rates of spontaneous recovery over 12 to 18 months.
| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Posterior Dislocation | 1% - 3% | Component malposition, failure of posterior repair, non-compliance. | Closed reduction. Revision for recurrent instability (repositioning, dual-mobility). |
| Sciatic Nerve Palsy | 0.5% - 1.5% | Retractor injury, excessive lengthening, hematoma compression. | Remove compressive dressings, rule out hematoma. AFO and observation. |
| Periprosthetic Fracture | 1% - 4% | Osteoporosis, aggressive broaching, press-fit stem impaction. | Intraoperative: cerclage wiring or bypass with longer stem. Postoperative: ORIF or revision. |
| Leg Length Discrepancy | 1% - 5% | Inaccurate templating, failure to reproduce center of rotation. | Conservative: shoe lifts. Operative: revision if severely symptomatic or causing instability. |

Infection and deep vein thrombosis (DVT) are universal risks in arthroplasty. Prophylactic measures, including perioperative antibiotics and multimodal venous thromboembolism (VTE) prophylaxis (e.g., aspirin, low molecular
Clinical & Radiographic Imaging


You Might Also Like


