
A patient presents with a deep, complex soft tissue injury of the proximal forearm. Describe the anatomical landmarks and the step-by-step approach required to safely expose the proximal radius and ulna, minimizing the risk of iatrogenic nerve injury.
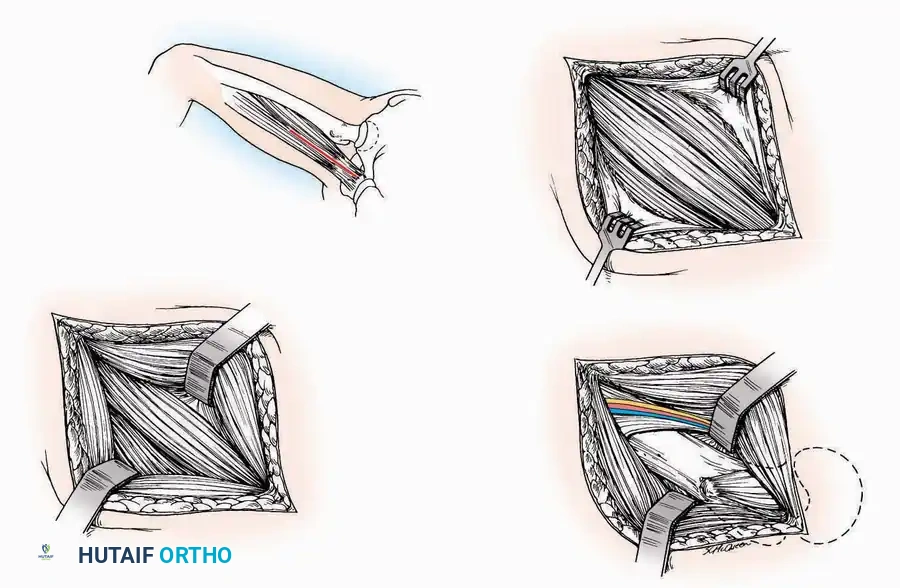
Candidate: I would perform a Boyd or modified Kocher approach. I'd identify the interval between the anconeus and the extensor carpi ulnaris (ECU) to reach the proximal ulna, then proceed to expose the proximal radius. I must be careful of the Posterior Interosseous Nerve (PIN) by keeping the forearm pronated during the radial dissection.
Failing to mention the "Safe Zone" for the PIN (e.g., the proximity of the nerve to the radial neck). Candidates often describe the approach vaguely without defining the specific muscles involved or the risk of supination during radial exposure, which puts the PIN at risk.
I would utilize the Boyd approach. 1. Skin Incision: From the lateral epicondyle towards the ulnar border. 2. Interval: Develop the interval between the anconeus and ECU. 3. Deep Dissection: Reflect the anconeus and supinator ulnarly. 4. PIN Protection: I must subperiosteally elevate the supinator and, crucially, maintain the forearm in full pronation to displace the PIN away from the radial neck, reducing the risk of iatrogenic injury. 5. Closure: Repair the supinator and anconeus meticulously to maintain forearm stability.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding examination-questions-for-grade-2018