Master Urinary Tract Stones: 2019 Exam Questions

Key Takeaway
This interactive board review contains 100 randomly selected orthopedic surgery questions with clinical images, immediate feedback, and detailed references.
Master Urinary Tract Stones: 2019 Exam Questions
Randomized Orthopedic Board Review Practice
Welcome to this customized practice session containing 100 randomly selected high-yield multiple-choice questions (MCQs).
These questions have been pulled from our extensive master database of OITE and AAOS board-style questions to provide you with an unpredictable, exam-like simulation.
Features of this Practice Set:
- True Randomization: Questions span across all subspecialties including Spine, Trauma, Arthroplasty, Sports Medicine, and Pediatrics.
- Interactive UI: Switch between Study Mode (immediate feedback and clinical explanations) and Exam Mode (timed simulation with grading).
- Track your progress: Use the question navigator dots to flag difficult questions and review your performance at the end.
Dive into the quiz below to test your orthopedic knowledge!
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Figures 35a and 35b show the radiographs of a 7-year-old patient who has progressive deformity of the right thigh accompanied by a dull persistent pain radiating to the knee. Examination reveals an obvious bulge in the right thigh, with flexion of the hip beyond 50° only if the hip is allowed to externally rotate. Management should consist of
Explanation
REFERENCES: Zionts LE, Ebramzadeh E, Stott NS: Complications in the use of the Bailey-Dubow extensible nail. Clin Orthop 1998;348:186-195.
Luhmann SJ, Sheridan JJ, Capelli AM, Schoenecker PL: Management of lower-extremity deformities in osteogenesis imperfecta with extensible intramedullary rod technique: A 20-year experience. J Pediatr Orthop 1998;18:88-94.
Glorieux FH, Bishop NJ, Plotkin H, Chabot G, Lanoue G, Travers R: Cyclic administration of pamidronate in children with severe osteogenesis imperfecta. N Engl J Med 1988;339:947-952.
Question 2
Which factor has the most negative influence on the success of knee osteochondral allograft transplantation?
Explanation
The images illustrate a large unstable osteochondral lesion of the medial femoral condyle. Radiographs and MR images clearly show deep subchondral bone involvement. The appropriate choice of surgery is OCA transplantation, which is indicated for primary treatment of large cartilage lesions, osteochondral lesions, and salvage procedure from failed prior cartilage surgery. Correction of mechanical axis malalignment, ligamentous insufficiency, and meniscal deficiency should also be addressed. ACI alone or an arthroscopic microfracture procedure would not address the bone defect, leaving an uneven articular surface. Although an osteotomy may be a viable choice, a distal femoral varus osteotomy would increase the contact pressure in the medial compartment and worsen the situation.
The histologic anatomy of articular cartilage is well described. The superficial layer or lamina splendens contains a small amount of proteoglycan with collagen fibrils arranged parallel to the articular surface. In contrast, the deep zone contains the largest-diameter
collagen fibrils, oriented perpendicular to the joint surface, and the highest concentration of proteoglycans.

Video 54 this video is uploaded at
CLINICAL SITUATION FOR QUESTIONS 51 THROUGH 54
Figures 51a and 51b are the radiographs of an 18-year-old football linebacker who was involved in a tackle and fell onto an outstretched left arm. He had immediate pain and deformity of his left elbow.
Question 3
Which of the following factors has been shown to be the strongest predictor of screw cutout of a dynamic compression hip screw used for an intertrochanteric femur fracture?

Explanation
Baumgaertner et al reported that he had no screws cut out if the tip-apex distance was less than 25mm. Tip-apex distance was the strongest predictor of cutout. Increasing age of the patient, poor reduction, use of a high angle sideplate, and unstable fracture were weaker predictors of cutout.
Kyle et al demonstrated that obtaining an anatomic reduction when using a sliding hip screw with intertrochanteric fractures leads to the best radiographic and clinical outcomes.
Question 4
Deep venous thromboses are primarily composed of red blood cells and fibrin. What is fibrin?
Explanation
Question 5
With the increasing availability of total hip arthroplasty (THA) to younger patients with hip osteoarthritis, there has been increased use of alternative bearing surfaces. Compared to a ceramic-on-ceramic articulation, which of the following is a specific advantage of a metal-on-metal bearing surface?
Explanation
REFERENCES: Heisel C, Silva M, Schmalzried TP: Bearing surface options for total hip replacement in young patients. Instr Course Lect 2004;53:49-65.
D’Antonio J, Capello W, Manley M, et al: New experience with alumina-on-alumina ceramic bearings for total hip arthroplasty. J Arthroplasty 2002;17:390-397.
Question 6
A 55-year-old woman with a history of untreated idiopathic scoliosis has had neurogenic claudication for the past several months. MRI reveals spinal stenosis at L2-L3, L3-L4, and L4-L5. Radiographs show a 45° lumbar curve from T10 to L4, with a degenerative spondylolisthesis at L4-L5. Laminectomy at the stenotic levels and stabilization of the deformity are planned. Which of the following is NOT considered an absolute indication for extending the fusion to the sacrum, rather than stopping at L5?
Explanation
REFERENCES: Bradford DS, Tay BK, Hu SS: Adult scoliosis: Surgical indications, operative management, complications, and outcomes. Spine 1999;24:2617-2629.
Bridwell KH: Where to stop the fusion distally in adult scoliosis: L4, L5, or the sacrum? Instr Course Lect 1996;45:101-107.
Edwards CC II, Bridwell KH, Patel A, et al: Long adult deformity fusions to L5 and the sacrum: A matched cohort analysis. Spine 2004;29:1996-2005.
Question 7
1 and 2 demonstrate the radiographs obtained from a year-old woman with end-stage debilitating osteoarthritis of the right hip. She is contemplating total hip arthroplasty (THA). She has a history of right hip dysplasia and underwent hip osteotomy as an adolescent. Over the years, nonsurgical treatment, including weight loss, activity modifications, and intra-articular injections, has failed. Her infection work-up reveals laboratory findings within defined limits.The patient undergoes successful primary THA with a metal-on-metal bearing. At year follow-up, she reports no pain and is highly satisfied with the procedure. However, 3 years after the index procedure, she reports atraumatic right hip pain that worsens with activities. Radiographs reveal the implants in good position with no sign of loosening or lysis. An initial laboratory evaluation reveals a normal sedimentation rate and C-reactive protein (CRP) level. The most appropriate next diagnostic step is
Explanation
THA has proven to be durable and reliable for pain relief and improvement of function in patients with end-stage arthritis. Appropriate bearing selection is critical to minimize wear and hip complications. A
metal-on-metal articulation is associated with excellent wear rates in vitro. Because it offers a low wear rate with large femoral heads, it is an attractive bearing choice for THA. However, local soft-tissue reactions, pseudotumors, and potential systemic reactions—including renal failure, cardiomyopathy, carcinogenesis, and potential teratogenesis after the possible transfer of metal ions across the placental barrier—make metal-on-metal bearings less desirable and relatively contraindicated for younger women of child-bearing age.The work-up of a painful metal-on-metal hip arthroplasty necessitates a systematic approach. Several algorithms have been proposed. Routine laboratory studies including the erythrocyte sedimentation rate, C-reactive protein (CRP) level, and serum cobalt and chromium ion levels should be obtained for all patients with pain. Advanced imaging, including MRI with MARS, should be performed to evaluate for the presence of fluid collections, pseudotumors, and abductor mechanism destruction. Infection can coexist with metal-on-metal reactions, so when indicated (if the CRP level is elevated), a hip arthrocentesis should be obtained. However, in this setting, a manual cell count and differential should be obtained because an automated cell counter may provide falsely elevated cell counts. The results of revision surgery for a failed metal-on-metal hip prosthesis can be variable. The amount of local tissue destruction and the integrity of the hip abductor mechanism can greatly influence outcomes. Instability is the most common complication following a revision of failed metal-on-metal hip replacements.
Question 8
- Which of the following radiographic findings would be characteristic of the knee joints of a patient with neuropathic osteoarthropathy of the knee?
Explanation
The loss of sensation to the joint is followed by severe degenerative changes, osteophyte formation, articular and subchondral fractures, and often calcification of surrounding soft tissues. In the knee, this is a tricompartmental disease and will not selectively affect one compartment over another.
Question 9
Which of the following methods best aids in diagnosis of an interdigital neuroma?
Explanation
REFERENCES: Richardson EG (ed): Orthopaedic Knowledge Update: Foot and Ankle 3. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2004, pp 145-147.
Bennett GL, Graham CE, Mauldin DM: Morton’s interdigital neuroma: A comprehensive treatment protocol. Foot Ankle Int 1995;16:760-763.
Question 10
A 23-year-old otherwise healthy 6-ft, 4-in basketball player complains of pain in his knees. An examination reveals localized tenderness to palpation over the inferior pole of the patella. The patient notes a significant exacerbation of his pain when the examiner takes the knee from flexion to extension. Review Topic
Explanation
Question 11
Which of the following is a recognized consequence of hip fusion?
Explanation
REFERENCES: Liechti R (ed): Hip Arthrodesis and Associated Problems. Berlin, Germany, Springer-Verlag, 1978, pp 109-117.
Sponseller PD, McBeath AA, Perpich M: Hip arthrodesis in young patients: A long-term follow-up study. J Bone Joint Surg Am 1984;66:853-859.
Question 12
A 13-year-old gymnast presents with ongoing knee pain for the past few months. She tried conservative measures including kinesiotaping, physical therapy and rest. On physical exam, she has normal valgus alignment, negative patellar tilt and discomfort with resisted open chain knee extension. A representative radiographs are shown in Figure A-C. What is the most likely clinical diagnosis? Review Topic

Explanation
Evaluation of a patient with patellofemoral pain requires a physical examination and plain radiographs. Appropriate examination of all structures around the knee is critical to rule out other diagnoses. An MRI is useful for evaluating intra-articular or intra-osseous lesions, if clinical suspicion is suggestive of this. Treatment is predominantly conservative, with focus on low impact exercises that maximize aerobic conditioning.
Earl et al. review the epidemiology, etiology and management of patellofemoral syndrome. They note that there is no clear cause of this issue, although issues related to the quadriceps and dynamic malalignment may be contributory.
Outerbridge et al. describe overuse injuries in the young athletic patient. They provide an overview of diagnosis and management specific to this patient population.
Figures A, B and C show AP, lateral and merchant radiographs of a normal knee in a skeletally immature individual. No osseous abnormalities are identified.
Incorrect
Question 13
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
REFERENCES: Alman BA, Goldberg MJ: Syndromes of orthopaedic importance, in Morrissy RT, Weinstein SL (eds): Lovell and Winter’s Pediatric Orthopaedics, ed 5. Philadelphia, PA, Lippincott Williams and Wilkins, 2001, pp 287-338.
Greene WB: Neurofibromatosis type I, in Fitzgerald RH, Kaufer H, Malkani AL (eds): Orthopaedics. St Louis, MO, Mosby, 2002, pp 1584-1588.
Question 14
In a patient who has undergone fusion with instrumentation from T4 to the sacrum for adult scoliosis, at which site is a pseudarthrosis most likely to be discovered?
Explanation
REFERENCES: Saer EH III, Winter RB, Lonstein JE: Long scoliosis fusion to the sacrum in adults with nonparalytic scoliosis: An improved method. Spine 1990;15;650-653.
Kostuik JP, Hall BB: Spinal fusions to the sacrum in adults with scoliosis. Spine
1983;8:489-500.
Balderston RA, Winter RB, Moe JH, et al: Fusion to the sacrum for nonparalytic scoliosis in the adult. Spine 1986;11:824-829.
Question 15
A 9-year-old boy is injured while playing soccer. His examination reveals painful range of motion between 5° and 75°. There is tenderness on the medial side of his knee. There is no effusion, a grade 1A Lachman test, and severe pain over the medial epicondyle of the knee. Varus stress is negative and pain is elicited with valgus stress. Initial radiographs were negative for abnormality. What is the most likely area of injury?
Explanation
Question 16
A 30-year-old man who underwent an anterior lumbar diskectomy and fusion at L4-5 and L5-S1 through an anterior retroperitoneal approach 1 month ago now reports he is unable to obtain and maintain an erection. The most likely cause of this condition is
Explanation
REFERENCES: Flynn JC, Price CT: Sexual complications of anterior fusion of the lumbar spine. Spine 1984;9:489-492.
Johnson RM, McGuire EJ: Urogenital complications of anterior approaches to the lumbar spine. Clin Orthop 1981;154:114-118.
Question 17
During head-on motor vehicle collisions occurring at highway speeds, airbag-protected individuals have a decreased rate (as compared to non-airbag protected individuals) of all of the following EXCEPT:

Explanation
Question 18
Figures 1 and 2 are the radiographs of an 18-year-old man who had surgery 6 months ago at an outside institution. He is being referred now because he has persistent pain. He is tender over the scaphoid at the snuffbox. What is the most appropriate next imaging step in his pain workup?

Explanation
Scaphoid nonunions are difficult to diagnose on plain radiographs, which offer poor reliability when attempting to determine if there is bridging trabeculae crossing the fractures site. CT scans are more useful for diagnosing scaphoid nonunion. When scanned using conventional axial cuts, the slices mayskip through the fracture nonunion site, thereby missing the defect, even with reformats. MR imaging is useful in diagnosing acute scaphoid fractures and has a high sensitivity and diagnostic value for excluding scaphoid fractures as well. Contrast does not enhance the utility of MR imaging in fracture diagnosis.
Question 19
What is the most common malignant tumor of the foot?
Explanation
REFERENCES: Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 11-26.
Bos GD, Ester RJ, Woll TS: Foot tumors: Diagnosis and treatment. J Am Acad Orthop Surg 2002;10:259-270.
Question 20
A 22-month-old girl has cerebral palsy. Which of the following findings is a good prognostic indicator of the child’s ability to walk in the future?
Explanation
REFERENCES: Bleck EE: Orthopaedic Management in Cerebral Palsy. Lavenham, Suffolk, The Lavenham Press, 1987, pp 121-139.
Tachdjian MO: The neuromuscular system: Cerebral palsy, in Wickland EH Jr (ed): Pediatric Orthopaedics, ed 2. Philadelphia, PA, WB Saunders, 1990, vol 2, p 1621.
Question 21
A patient who underwent intramedullary nailing of a femoral shaft fracture 2 weeks ago now reports groin pain. What is the next most appropriate step in management?
Explanation
obtaining a dedicated AP radiograph of the hip with the leg internally rotated 15 to 20 degrees. Because the femoral neck is anteverted, 15 to 20 degrees of internal rotation of the hip offers the best view of the femoral neck. Whereas associated lumbar spine pathology may cause groin pain, the presence of a missed femoral neck fracture must first be ruled out prior to investigating other sources of pain.
Question 22
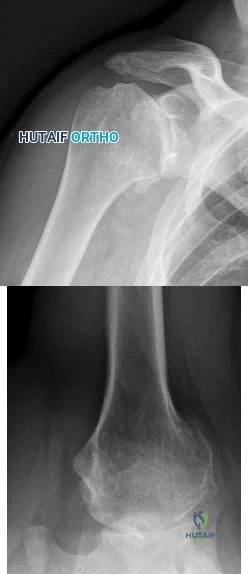
A 64-year-old man who was involved in a high-speed motor vehicle accident 6 weeks ago has been in the ICU with a closed head injury. Examination reveals that his range of motion for external rotation to the side is -30 degrees. Radiographs are shown in Figures 28a and 28b. What is the most likely diagnosis?
Explanation
REFERENCES: Robinson CM, Aderinto J: Posterior shoulder dislocations and
fracture-dislocations. J Bone Joint Surg Am 2005;87:639-650.
Cicak N: Posterior dislocation of the shoulder. J Bone Joint Surg Br 2004;86:324-332.
Question 23
repair of the rotator cuff
Explanation
Question 24
- Which of the following conditions associated with a closed fracture of the clavicle indicates the need for open reduction and internal fixation?
Explanation
Question 25
Figure 13 shows the clinical photograph of a 66-year-old man who has had an increasingly painful right foot deformity for the past 3 years. Examination reveals that the subtalar joint is fixed in 15° of valgus, and forefoot supination can be corrected to 10° from neutral. Nonsurgical management has failed to provide relief. Treatment should now consist of
Explanation
REFERENCE: Mann RA: Flatfoot in adults, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 6. St Louis, MO, Mosby, 1993, pp 757-784.
Question 26
A patient sustains a comminuted calcaneus fracture. Three months after the injury the patient complains of shoewear problems secondary to clawing of the lesser toes. What is the most likely explanation for this deformity?

Explanation
Myerson reported 3/43 patients in his series below had chronic foot compartment syndrome. There are 9 compartments in the foot: (1) medial, (2) superficial, (3) lateral, (4) adductor, (5-8) four interossei, and (9) calcaneal. The plantar fascia limits the space available for hematoma and swelling, causing damage to the intrinsic flexors of the foot (particularly the lumbricals and interossei), resulting in clawtoes.
Question 27
A professional baseball team has several pitchers with complaints of velocity loss with their pitches and shoulder pain of their dominant shoulders during spring training. Pitch counts are properly monitored. The average glenohumeral internal rotation deficit on the pitching staff is 45 degrees. The best intervention would be: Review Topic
Explanation
GIRD is a phenomenon that is frequently found in high-level overhead throwing athletes, predominantly baseball pitchers. It is defined as the measured difference in internal rotation between the non-dominant arm and dominant arm. Worsening range of motion deficits are seen with increased repetitions, both over a single season and a career. GIRD > 25º is associated with development of shoulder pathologies or pain requiring periods of inactivity. Cessation of overhead throwing activities and initiation of a stretching program to address posterior capsular contractures is largely effective (90% in some series).
Burkhart et al. reviewed the conditions associated with high-level overhead throwing athletes shoulders, culminating in a theory of pathologic progression to "dead arm syndrome" (loss of velocity and effective pitching). Their theory attributes adaptive hyperexternal rotation (occurs during late-cocking / early acceleration phases of pitching) to lead to posterior-inferior capsular contracture and GIRD. Subsequent injuries to anterior structures - including SLAP lesions - would then occur.
Illustration A is a cartoon depiction of how to perform the sleeper stretch. This is a common component of a pitcher's maintenance stretching program.
Incorrect Answers:
Question 28
A 4-year-old boy sustained a nondisplaced, but complete, fracture of the left proximal tibial metaphysis 1 year ago. The fracture healed uneventfully in an anatomic position. Examination of the injured extremity now reveals 18° of valgus compared with 3° of valgus on the opposite side. Management should now include
Explanation
REFERENCES: Zionts LE, MacEwen GD: Spontaneous improvement of posttraumatic tibia valga. J Bone Joint Surg Am 1986;68:680-687.
Beaty JH, Kumar A: Fractures about the knee in children. J Bone Joint Surg Am 1994;76:1870-1880.
Question 29
Which of the following tissues used for anterior cruciate ligament (ACL) reconstruction has the highest maximum load to failure?
Explanation
REFERENCES: Hamner DL, Brown CH Jr, Steiner ME, Hecker AT, Hayes WC: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: Biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 1999;81:549-557.
Cooper DE, Deng XH, Burstein AL, Warren RF: The strength of the central third patellar tendon graft: A biomechanical study. Am J Sports Med 1993;21:8l8-823.
Brown CH Jr, Steiner ME, Carson EW: The use of hamstring tendons for anterior cruciate ligament reconstruction: Technique and results. Clin Sports Med 1993;12:723-756.
Engebretsen L, Lewis JL: Graft selection and biomechanical considerations in ACL reconstruction. Sports Med Arthroscopy Rev 1996;4:336-341.
Question 30
- The stability of the longitudinal arch of the foot during standing with equal weight on both feet is due primarily to
Explanation
Question 31
A 33-year old man sustains a posterior elbow dislocation after a fall. Attempts at closed reduction result in recurrent instability. What is the most common ligamentous injury found at the time of surgical stabilization?
Explanation
with and without associated fractures at the time of surgery. Injury to the lateral collateral ligament complex was seen in every case, with avulsion from the distal humerus as the most common finding. Midsubstance
tears, proximal avulsions, and distal bony avulsions of the ulnar collateral ligament are less common.
Question 32
Which of the following complications may occur subsequent to resurfacing hip arthroplasty for osteonecrosis of the hip but not after total hip arthroplasty?
Explanation
REFERENCES: Gabriel JL, Trousdale RT: Stem fracture after hemiresurfacing for femoral head osteonecrosis. J Arthroplasty 2003;18:96-99.
Amstutz HC, Campbell PA, Le Duff MJ: Fracture of the neck of the femur after surface arthroplasty of the hip. J Bone Joint Surg Am 2004;86:1874-1877.
Question 33
In the evaluation of somatosensory-evoked potential waveforms for intraoperative neuromonitoring for spinal surgery, the minimum criteria for determining potentially significant changes include Review Topic
Explanation
Question 34
A 35-year-old woman began to train for a half marathon. After 8 weeks of increasing her mileage, what changes can you expect in her Achilles tendon?
Explanation
Question 35
Figure 29 is the radiograph of a 30-year-old man who sustained an isolated tibial shaft fracture. What is the most common deformity with nonsurgical management?

Explanation
discrepancies are also common. Here the fibula acts as a strut, preventing valgus collapse but predisposing to varus collapse. Valgus and procurvatum is the typical deformity in proximal tibial fractures.
Question 36
A patient notes pain under the first metatarsophalangeal joint following a soccer injury. The MRI scans shown in Figures 27a and 27b reveal what pathologic finding?
Explanation
REFERENCES: Watson TS, Anderson RB, Davis WH: Periarticular injuries to the hallux metatarsophalangeal joint in athletes. Foot Ankle Clin 2000;5:687-713.
Tewes DP, Fischer DA, Fritts HM, et al: MRI findings of acute turf toe: A case report and review of anatomy. Clin Orthop 1994;304:200-203.
Question 37
The Lisfranc ligament connects the base of the
Explanation
REFERENCES: Sarrafian SK: Anatomy of the Foot and Ankle: Descriptive, Topographic, Functional, ed 2. Philadelphia, PA, JB Lippincott, 1993.
Solan MC, Moorman CT III, Miyamoto RG, et al: Ligamentous restraints of the second tarsometatarsal joint: A biomechanical evaluation. Foot Ankle Int 2001;22:637-641.
Question 38
A 46-year-old woman reports pain and a shortened appearance of her toe after undergoing a Keller resection arthroplasty 2 years ago for hallux rigidus. Examination reveals mild swelling and motion limited to 25 degrees at the metatarsophalangeal joint. Radiographs show large dorsal osteophytes on the first metatarsal head, 50% resection of the proximal phalanx, and complete loss of the metatarsophalangeal joint space. Which of the following is considered the most reliable procedure to improve her pain and the appearance of her toe?
Explanation
REFERENCES: Myerson MS, Schon LC, McGuigan FX, Oznur A:Result of arthrodesis of the hallux metatarsophalangeal joint using bone graft for restoration of length. Foot Ankle Int 2000;21:297-306.
Mann RA, Coughlin MJ: Adult hallux valgus, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 252-253.
Mizel MS, Miller RA, Scioli MW (eds): Orthopaedic Knowledge Update: Foot and Ankle 2. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 293-303.
Question 39
The arrow in Figure 11 points toward a finding consistent with which of the following?
Explanation
REFERENCES: McLain R, Weinstein J (eds): Rothman-Simeone: The Spine, ed 4. Philadelphia, PA, WB Saunders, 1999, p 1173.
Koval KJ (ed): Orthopaedic Knowledge Update 7. Rosemont, IL, American Academy of Orthopaedic Surgeons, 2002, p 674.
Question 40
Figures 1 and 2 are the radiographs of a 55-year-old man who has a 3-year history of right shoulder pain. He has maximized nonoperative management and is interested in operative treatment. He had an open Bankart repair 20 years ago and did well until a few years ago. What is most important to know when deciding on the best surgical treatment for this patient?
Explanation
Although the radiographs do not reveal any obvious signs of rotator cuff failure, the patient had had an open Bankart 20 years ago. The integrity of the subscapularis tendon following a previous open shoulder procedure is crucial in deciding which type of arthroplasty to consider. Range of motion and infraspinatus strength do not affect the decision-making process, assuming the rotator cuff is intact. Activity level can be important when deciding whether to proceed with an arthroplasty, but it is not as important as the rotator cuff integrity when choosing which
arthroplasty to use.
Question 41
A 21-year-old collegiate track athlete increased her training 4 months ago in anticipation of starting the season. Two months into her training program, she reported pain followed by a 1-month history of diffuse pain in the first metatarsophalangeal joint that was aggravated by weight bearing. A removable walker boot partially relieved the pain, and she was able to complete the season. Her pain has now returned; however, she denies any history of injury. Examination reveals tenderness over the medial sesamoid but no deformities. A radiograph and bone scan are shown in Figures 22a and 22b. What is the best treatment option at this time?
Explanation
REFERENCES: Sanders R: Fractures of the midfoot and forefoot, in Coughlin MJ, Mann RA (eds): Surgery of the Foot and Ankle, ed 7. St Louis, MO, Mosby, 1999, pp 1601-1603.
Saxena A, Krisdakumtorn T: Return to activity after sesamoidectomy in athletically active individuals. Foot Ankle Int 2003;24:415-419.
Question 42
An 18-year-old football player lands on a flexed knee and ankle after being tackled. Examination reveals increased external rotation and posterior translation and varus at 30° of flexion, which decreases as the knee is flexed to 90°. What is the most likely diagnosis?
Explanation
REFERENCES: Harner CD, Hoher J: Evaluation and treatment of posterior cruciate ligament injuries. Am J Sports Med 1998;26:471-482.
Veltri DM, Warren RF: Isolated and combined posterior cruciate ligament injuries. J Am Acad Orthop Surg 1993;1:67-75.
Question 43
A workers' compensation carrier for a local manufacturing company requests a second opinion on a 59-year-old man who sustained a crush injury to his foot and leg at work 6 months ago. His leg and foot were pinned between a forklift and a wall when an employee he was supervising lost control of the forklift. The employer suspects that the injured worker is malingering because the treating physician released him to work, but he has not returned to work. Which of the following elements of your history will best help you determine that the injured worker does not want to return to work out of fear of a confrontation with the employee he was supervising?
Explanation
Question 44
With increasing abduction in the scapular plane, maintaining neutral rotation, contact area, and contact pressure per unit area between the humeral head and glenoid follows what pattern if the total load across the joint is held constant?
Explanation
REFERENCES: Warner JJP, Bowen MK, Deng XH, et al: Articular contact patterns of the normal glenohumeral joint. J Shoulder Elbow Surg 1998;7:381-388.
Greis PE, Scuderi MG, Mohr A, et al: Glenohumeral articular contact areas and pressures following labral and osseous injury to the anteroinferior quadrant of the glenoid. J Shoulder Elbow Surg 2002;11:442-451.
Question 45
A 12-year-old boy sustains open comminuted midshaft tibial and fibular fractures while playing indoor soccer. The wound is grossly clean and measures 7 cm with some periosteal stripping. Antibiotics and tetanus toxoid are administered immediately in the emergency department. Following irrigation and debridement of the wound in the operating room, treatment should include
Explanation
REFERENCES: Jones BG, Duncan RD: Open tibial fractures in children under 13 years of age-10 years experience. Injury 2003;34:776-780.
Bartlett CS III, Weiner LS, Yang EC: Treatment of type II and type III open tibia fractures in children. J Orthop Trauma 1997;11:357-362.
Robertson P, Karol LA, Rab GT: Open fractures of the tibia and femur in children. J Pediatr Orthop 1996;16:621-626.
Cullen MC, Roy DR, Crawford AH, et al: Open fracture of the tibia in children. J Bone Joint Surg Am 1996;78:1039-1047.
Question 46
A 30-year-old woman who runs approximately 30 miles a week has had right hip and groin pain for the past 3 weeks. Examination reveals an antalgic gait, limited motion of the right hip, and pain, especially with internal and external rotation. Plain radiographs are normal, and an MRI scan is shown in Figure 21. Management should consist of
Explanation
REFERENCES: Griffin LY (ed): Orthopaedic Knowledge Update: Sports Medicine. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 239-253.
Fullerton LR Jr, Snowdy HA: Femoral neck stress fractures. Am J Sports Med
1988;16:365-377.
Question 47
A 19-year-old soccer player feels a pop in his knee while making a cut and notes the development of an effusion over several hours. Examination reveals medial joint line tenderness, but the knee is stable to manual stress testing of all ligaments. Examination under anesthesia confirms a stable knee. What is the most critical factor in determining healing after repair of the lesion shown in Figure 14?
Explanation
REFERENCES: DeHaven KE, Arnoczky SP: Meniscus repair: Basic science, indications for repair, and open repair. Instr Course Lect 1994;43:65-76.
Henning CE, Lynch MA, Clark JR: Vascularity for healing of meniscus repairs. Arthroscopy 1987;3:13-18.
Question 48
Figure 17 shows the clinical photograph of a 45-year-old female tennis player who has right arm pain and weakness with elevation after undergoing a cervical biopsy several months ago. The cause of her shoulder weakness is damage to the
Explanation
REFERENCES: Kuhn JE, Plancher KD, Hawkins RJ: Scapular winging. J Am Acad Orthop Surg 1995;3:319-325.
Wright TA: Accessory spinal nerve injury. Clin Orthop 1975;109:15-18.
Question 49
5 mm of change in the atlanto-dens interval (ADI) between flexion and extension views
Explanation
With the introductions of disease-modifying antirheumatic agents (DMARDs), the incidence of RA patients undergoing cervical spine surgery has decreased significantly. Basilar invagination, atlantoaxial instability, and subaxial subluxation are the three most common manifestations of cervical disease. Multiple studies in RA patients with untreated or poorly controlled disease have led to the development of a set of measurements that identify patients who require surgical intervention and predict outcome after surgery. Additionally, progressive neurological compromise and
refractory
pain
are
indications
for
intervention.
Kim and Hilibrand reviewed management of the rheumatoid cervical spine and outline parameters for surgical intervention. These include a PADI < 14 mm, cervicomedullary angle <135 degrees, progressive neurological deficit, refractory pain, atlantoaxial impaction as determined by migration >5 mm rostral to McGregor's line, and subaxial canal diameter < 14 mm.
Boden et al. analyzed 73 patients followed for rheumatoid cervical spine disease with an average follow up of 7 years. They found that the PADI correlated with paralysis. Patients with PADI less than 10 mm had no recovery, and all patients with PADI greater than 14 mm had full recovery.
Illustration A demonstrates the measurement of the ADI and PADI. Illustration B demonstrates how to measure the cervicomedullary angle (as marked by A), which is typically determined on MRI
Incorrect
Question 50
Figure 45 shows the radiograph of a 2-year-old patient who has progressive lumbar scoliosis as the result of hemivertebra. Examination reveals no associated cutaneous lesions, and an MRI scan shows no associated intraspinal anomalies. Treatment should consist of
Explanation
REFERENCE: Callahan BC, Georgopoulos G, Eilert RE: Hemivertebral excision for congenital scoliosis. J Pediatr Orthop 1997;17:96-99.
Question 51
An ulnar nerve palsy at the level of the wrist is typically associated with deficits in the palmaris brevis, the hypothenar muscles, and what other groups of muscles?
Explanation
median nerve.
REFERENCES: Goldfarb CA, Stern PJ: Low ulnar nerve palsy. JASSH 2003;3:14-26.
Omer G: Ulnar nerve palsy, in Green DP, Hotchkiss R, Pederson W (eds): Green’s Operative Hand Surgery, ed 4. Philadelphia, PA, Churchill Livingstone, 1999, pp 1526-1541.
Question 52
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 53
A 13-year-old boy has pain and a firm mass in his left knee. A radiograph and MRI scan are shown in Figures 2a and 2b, and a biopsy specimen is shown in Figure 2c. Based on these findings, what is the most likely diagnosis?
Explanation
REFERENCES: Simon M, Springfield D, et al: Osteogenic sarcoma: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott Raven, 1998, p 267.
Wold LA, et al: Atlas of Orthopaedic Pathology. Philadelphia, PA, WB Saunders, 1990,
pp 14-15.
Question 54
A 24-year-old baseball pitcher reports pain over the posterior aspect of his shoulder that occurs only during throwing. He notes that the discomfort is greatest during the late cocking and early acceleration phases. Examination reveals localized tenderness with palpation over the external rotators and posterior glenoid. Radiographs are shown in Figures 38a through 38c. What is the most likely diagnosis?
Explanation
REFERENCES: Meister K, Andrews JR, Batts J, Wilk K, Baumgarten T, Baumgartner T: Symptomatic thrower’s exostosis: Arthroscopic evaluation and treatment. Am J Sports Med 1999;27:133-136.
Ferrari JD, Ferrari DA, Coumas J, Pappas AM: Posterior ossification of the shoulder: The Bennett lesion. Etiology, diagnosis, and treatment. Am J Sports Med 1994;22:171-176.
Walch G, Boileau P, Noel E, et al: Impingement of the deep surface of the supraspinatus tendon on the posteriorsuperior glenoid rim: An arthroscopic study. J Shoulder Elbow Surg 1992;1:238-245.
Question 55
During total knee arthroplasty using a posterior cruciate-retaining design, excessive tightness in flexion is noted, while the extension gap is felt to be balanced. Which of the following actions will effectively balance the knee?
Explanation
REFERENCE: Ayers DC, Dennis DA, Johanson NA, Pelligrini VD: Common complications of total knee arthroplasty. J Bone Joint Surg Am 1997;79:278-311.
Question 56
Figure 1 shows a patient with an open tibia fracture who presents to the emergency department after a propeller injury in brackish water (river water and sea water). What is the most appropriate antibiotic coverage for this patient?

Explanation
soil-borne pathogens (clostridial species). Vancomycin is not indicated for coverage in marine environments, rather it is more commonly used for populations with a high prevalence of nosocomial infections. Sulfamethoxazole-trimethoprim is not used for open fracture coverage.
Question 57
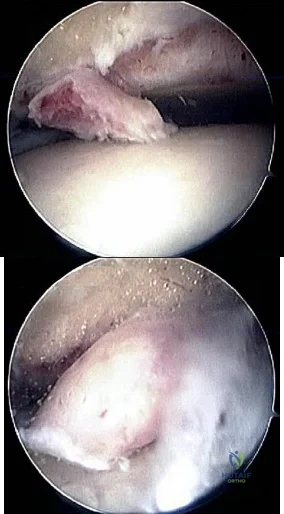
40A B Figures 40a and 40b are this patient's intraoperative arthroscopic images. The abnormality seen here illustrates which of the patient's clinical findings?
Explanation
Ankle sprains are the most common musculoskeletal injury; however, most of these sprains do not progress to chronic instability. Initial injuries are treated with RICE (rest, ice, compression, elevation), range of motion, weight bearing
as tolerated, and proprioceptive therapy. Lace-up ankle braces are most effective during the subacute period after a sprain. Structured physical therapy focused on proprioception is recommended for 6 weeks. Examination findings for ankle ligament instability are unreliable because of associated subtalar joint motion. Casting is not as effective as functional rehabilitation. Stress radiographs are recommended, but a clear pathologic range of measurements is not defined. Generalized ligament laxity can result in false-positive findings of instability; therefore, contralateral stress radiographs are often necessary for comparison. The difference in anterior drawer measurement between both ankles should not exceed 5mm. Likewise, the difference in talar tilt measurement between both ankles should be 5 or fewer degrees. Patients with mechanical symptoms, a joint effusion, or continued pain may have an intra-articular pathology such as a loose body or osteochondral lesion. Ankle instability can exist without ligamentous laxity. Symptoms of chronic instability can result from osteochondral lesions of talus, peroneal tendon pathology, loose bodies, anterior ankle impingement, and fracture nonunions. Although there is not sufficient evidence to recommend arthroscopy prior to all ligament reconstructions, arthroscopy is recommended when other pathology is suspected.
RECOMMENDED READINGS
Colville MR. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998 Nov-Dec;6(6):368-77. Review. PubMed PMID: 9826420. View Abstract at PubMed
DiGiovanni CW, Brodsky A. Current concepts: lateral ankle instability. Foot Ankle Int. 2006 Oct;27(10):854-66. Review. PubMed PMID: 17054892. View Abstract at PubMed
Maffulli N, Ferran NA. Management of acute and chronic ankle instability. J Am Acad Orthop Surg. 2008 Oct;16(10):608-15. Review. PubMed PMID: 18832604. View Abstract at PubMed
Question 58
What is the most consistent finding regarding glenohumeral kinematics in patients with symptomatic tears of the rotator cuff?
Explanation
REFERENCES: Yamaguchi K, Sher JS, Anderson WK, et al: Glenohumeral motion in patients with rotator cuff tears: A comparison of asymptomatic and symptomatic shoulders. J Shoulder Elbow Surg 2000;9:6-11.
Poppen NK, Walker PS: Normal and abnormal motion of the shoulder. J Bone Joint Surg Am 1976;58:195-201.
Question 59
A 6-year-old boy presents with a mass and a lucent lesion involving the tibial shaft as seen in Figure 17a. The mass is mildly tender to palpation. The bone scan is focally hot in the tibia. Biopsy specimens are shown in Figures 17b and 17c. What is the most likely diagnosis?
Explanation
REFERENCES: Campanacci M, Laus M: Osteofibrous dysplasia of the tibia and fibula. J Bone Joint Surg Am 1981;63:367-375.
McCaffery M, Letts M, Carpenter B, et al: Osteofibrous dysplasia: A review of the literature and presentation of an additional 3 cases. Am J Orthop 2003;32:479-486.
Question 60
During C1-C2 transarticular screw fixation, screw misplacement is most likely to result in injury to the
Explanation
REFERENCES: Mueller ME, Allgower M, et al: Manual of Internal Fixation, ed 3. New York, NY, Springer-Verlag, 1991, pp 634-636.
Gebhard JS, Schimmer RC, Jeanneret B: Safety and accuracy of transarticular screw fixation C1-C2 using an aiming device: An anatomic study. Spine 1998;23:2185-2189.
Question 61
What part of the glenoid labrum has the least vascularity?
Explanation
REFERENCE: Cooper DE, Arnoczky SP, O’Brien SJ, et al: Anatomy, histology and vascularity of the glenoid labrum: An anatomical study. J Bone Joint Surg Am 1992;74:46-52.
Question 62
This reporting avoids a ceiling and floor effect, where most of the respondents score either at the top or the bottom of the assessment scale.
Explanation
The only accurate statement is that, at 1 month, patients in group 3 are more likely to live longer than patients in group 1 and 2.
The Kaplan-Meier curve is a statistical method used in survivorship analysis to estimate survival rates at different time points. The horizontal axis depicts the time points and the vertical axis depicts the probability of survival. At a given time point, greater survivorship is demonstrated by higher values on the vertical axis.
Kocher et al. reviewed clinical epidemiology and biostatistics relevant in orthopaedic
surgery. They reported that survivorship data are typically analyzed with use of the Kaplan-Meier method. This analysis is used when the actual date of the end point is known. A survivorship curve can be plotted to illustrate the percentage of patients still alive after the intervention.
Petrie et al. reviewed statistics, terminology and the principles involved in simple data analysis, and outlines areas of medical statistics that have gained
prominence in recent years in orthopaedic papers. The authors provide an insight into some of the more common errors that occur in published orthopaedic journals and which are frequently encountered at the review stage in papers submitted to the Journal of Bone and Joint Surgery.
Figure A depicts a Kaplan-Meier curve for 3 groups of patients undergoing 3 different interventions.
Incorrect Answers:
When evaluating patient-reported outcomes in spine surgery, the Patient- Reported Outcomes Measurement Information System (PROMIS) has been found to have what differences compared to other assessment tools?
Communication failures have been associated with increased treatment costs, increased complications, and delays in patient care.
The leading cause of medical errors, wrong-site surgeries, diagnostic delays and loss to follow-up is attributed to communication errors. Studies have shown that this directly leads to increased complications, increased treatment costs, and delays in patient care. In the surgical setting, the performance of the pre-surgical time-out affords clarification of the treatment plan, confirmation of the procedure and site, and an opportunity for the team to address any concerns.
Weller et al. reviewed barriers to effective teamwork in healthcare delivery. They found that effective communication across all team members, inclusive training, and the creation of democratic teams can reduce treatment delays and minimize complications. They concluded that all team members should have a shared understanding of the situation when involved in patients care.
Lingard et al. performed a prospective study determining the feasibility of a preoperative 10-item checklist discussion including nurses, surgeons, and anesthesiologists. They reported that the discussion usually took place prior to bringing the patient to the OR and took on average 3.5 minuted. Overall, the guided discussion was very well received by participants and provided an opportunity to inform providers of the patient's information to address potential problems. The authors cited that variations in workflow patterns as a potential barrier to widescale implementation of the checklist discussion.
Incorrect answers:
The outcomes of three novel interventions are investigated and the preliminary results are depicted in Figure A. Which of the following statements is most accurate?
Linezolid acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome.
Linezolid is a type of oxazolidinone, a relatively newer class of antibiotics that are active against multidrug-resistant staphylococci, streptococci, and enterococci. Although many antimicrobial agents affect or disrupt protein synthesis in bacteria, linezolid is unique in that it disrupts protein synthesis at its origin rather than later in the cascade. It achieves this by binding to the
50S subunit of the bacterial ribosome, preventing the formation of the initiation complex.
Swaney et al. performed a study to investigate the mechanism of action of linezolid. They found that linezolid inhibits the formation of the initiation complex in bacterial translation systems by preventing the formation of the N- formylmethionyl-tRNA-ribosome-mRNA ternary complex.
Thompson et al. performed a study on the efficacy of various antibiotics in treating periprosthetic joint infections (PJI). They administered oral linezolid with or without oral rifampin, intravenous vancomycin with oral rifampin, intravenous daptomycin or ceftaroline with or without oral rifampin, oral doxycycline, or sham treatment at human- exposure doses for 6 weeks in a mouse model of PJI. They found that oral-only linezolid-rifampin and all intravenous antibiotic-rifampin combinations resulted in no recoverable bacteria and minimized reactive bone changes. Additionally, although oral linezolid was found to be the most effective monotherapy, all oral and intravenous antibiotic monotherapies failed to clear infection or prevent reactive bone changes.
They concluded that the oral-only linezolid-rifampin option might reduce venous access complications and health-care costs.
Illustration A is a diagram depicting the mechanism of action of various antibiotics.
Incorrect Answers:
50S subunit of the bacterial ribosome, preventing protein chain elongation by inhibiting peptidyl transferase activity of the ribosome.
elongation by blocking aminoacyl translocation.
Failure of effective communication in the surgical setting has been associated with what?
Unfractionated heparin works in the coagulation cascade by promoting the ability of antithrombin III to inhibit factors IIa, III, Xa.
Heparin works by binding to and enhancing the ability of antithrombin III to inhibit factors IIa, III, Xa. It is metabolized by the liver. The risks associated with the use of unfractionated heparin include bleeding and heparin induced thrombocytopenia (HIT). The reversal agent is protamine sulfate.
Agnelli et al. reviewed direct thrombin inhibitors for the prevention of VTE after major orthopaedic surgery. They reported widespread use, however, limitations in the use of unfractionated heparin and low-molecular-weight heparins. They highlighted that direct thrombin inhibitors (Ximelagatran) inactivate thrombin without requiring any plasma cofactor, inhibit both free
and fibrin-bound thrombin, and do not appreciably bind to plasma proteins. They concluded that the features of rapid absorption, conversion, bioavailability, low variability, dose-time, food independency, and the predictable anticoagulant activity make direct thrombin inhibitors an attractive antithrombotic agent especially for prolonged out-of hospital prophylaxis.
Kwong et al. reviewed the efficacy and safety of fondaparinux, a selective factor Xa inhibitor and reported its efficacy and safety in 4 phase III clinical trials. They reported fondaparinux usage resulted in an overall 55% decrease in the risk of venous thromboembolism (VTE) relative to the low-molecular- weight heparin enoxaparin without increasing the incidence of clinically relevant bleeding, which was similarly low for both agents. They concluded
that the superior efficacy of fondaparinux relative to enoxaparin is the result of its unique mechanism of action, clinical pharmacology.
McLynn et al. investigated the risk factors and chemoprophylaxis for VTE in elective spine surgery. They reported that independent risk factors for VTE included greater age, male gender, increasing body mass index, dependent functional status, lumbar spine surgery, longer operative time, perioperative blood transfusion, longer length of stay, and other postoperative
complications. The majority of patients received unfractioned heparin and they observed this did not significantly influence the rate of VTE, but was associated with a significant increase in hematoma requiring a return to the operating room. They concluded that there is insufficient evidence to support the routine use of chemoprophylaxis in low-risk patients, and recommended full consideration of risks and benefits after elective spine surgery.
Figure A depicts the coagulation cascade, with the factor circled in red (IIa) being the target of unfractionated heparin, through its effect on antithrombin III.
Incorrect Answers:
Which of the following antibiotics acts to inhibit protein synthesis by preventing the formation of the initiation complex between the 30S and 50S subunits of the ribosome?
Acetaminophen inhibits prostaglandin E2 production through its effect on interleukin-1 beta. It exerts its effects on the central nervous system.
Multimodal pain management has become an increasingly important consideration in total joint arthroplasty recovery, namely in regard to minimizing opioid requirements while optimizing pain control and patient satisfaction. Given the negative side effects and increasing scrutiny on narcotic use, modalities that help to decrease post-operative narcotic requirements have become a major focus and include nonsteroidal anti- inflammatories, selective COX-2 inhibitors, gabapentinoids, local anesthetic blocks, and acetaminophen. Acetaminophen acts directly the central nervous system, providing both pain relief and antipyretic effects. It does so by inhibiting prostaglandin E2 production through the blockade of interleukin-1 beta.
Jinnah et al. performed a comparison of two multimodal pain regimens used for postoperative pain control in total joint arthroplasty patients. They hypothesized that using a multimodal pain protocol focusing on periarticular injections including liposomal bupivacaine would have improved results when compared with a parenteral opioid- based regimen. They found a decrease in length of stay and rate of discharge to skilled nursing facilities with the implementation of a novel multimodal protocol. They concluded that a multimodal approach inclusive of periarticular injection can lead to a reduced
length of stay.
Politi et al. performed a prospective randomized trial comparing the use of intravenous versus oral acetaminophen in total joint arthroplasty. They found that IV acetaminophen did not provide a significant difference in pain relief except within the first 0-4 hours. They concluded that IV acetaminophen does not provide a significant benefit when compared to the oral form, which is also less expensive.
Incorrect Answers:
Which of the following agents results in blood anticoagulation by exerting inhibitory effects on the factor circled in the color red in Figure A?
Based on the stress-strain curve in Figure A, ceramic has the highest modulus of elasticity.
Young's modulus is a measure of the stiffness (ability to resist deformation) of a material in the elastic zone that is calculated by measuring the slope of the stress-strain curve in the elastic zone. A higher modulus of elasticity indicates a stiffer material. Relative values of Young's modulus include: (1) ceramic, (2) alloy, (3) stainless steel, (4) titanium, (5)
cortical bone, (6) matrix polymers, (7) PMMA, (8) polyethylene, (9) cancellous bone, (10) tendon/ligaments, and (11) cartilage.
Lang et al. published a review on the use of ceramics in total hip replacement. They report that properties of ceramic which make it particularly attractive for this application include its hardness, high compression strength, and excellent wettability. However, its low fracture toughness and linear elastic behavior make it prone to breakage under stress.
Figure A is a stress-strain curve, the slope of which is used to determine Young's modulus.
Incorrect Answers:
Which of the following medications work by inhibiting prostaglandin E2 production through interleukin-1 beta?
A power analysis determines the minimum number of patients needed in a study to show a clinically significant difference. It should be performed before starting the study.
Power is the probability of finding a significant association if one truly exists. It is defined as 1 minus the probability of a type 2 error (beta) and is generally set to 80% meaning that we are willing to accept a 20% chance of a type 2 error. A power analysis will determine the minimum number of patients that shows a clinically significant difference. The minimum number of patients should be determined prior to initiating a study. Calculation of power after a study has been completed is controversial and discouraged.
Vavken et al. performed a review on the management of confounding in controlled orthopaedic trials. They report that confounding occurs when the effect of exposure of an outcome is distorted by a confounding factor and will lead to spurious effect estimates in clinical studies. They performed a cross- sectional study of a sample of controlled trials reported in the orthopaedic literature in 2006. They conclude that only 30 studies reported that the had a power analysis performed.
Kocher et al. performed a review of clinical epidemiology and biostatistics as a primer for orthopedic surgeons. They report that a power analysis should be performed prior to initiating the study. This will ensure the study is appropriately powered and decrease the effects of chance. They conclude that when a study determines no significant effect the power of the study should be reported.
Incorrect Answers:
Based on the stress-strain curve in Figure A, which of the following materials has the highest modulus of elasticity?
The World Health Organization (WHO) defines osteopenia as a bone mineral density (BMD) that is between 1 and 2.5 standard deviations below young normal (T-score of - 1 to -2.5).
The WHO defines osteopenia as decreased BMD without fracture risk. Osteopenia is defined as a T-score of 1 to 2.5 standard deviations below young normals (-1 to -2.5), while osteoporosis is defined as a T-score of more than
Question 63
A 5-year-old girl sustains an isolated injury to the right shoulder area after falling off the monkey bars. Examination reveals intact neurovascular function in the extremity distally, but she is quite uncomfortable. An AP radiograph of the proximal humerus is shown in Figure 24. Her parents state that she is a very talented gymnast. Considering her age and potential athletic career, management should consist of
Explanation
REFERENCES: Martin RF: Fractures of the proximal humerus and humeral shaft, in Letts RM (ed): Management of Pediatric Fractures. New York, NY, Churchill Livingstone, 1994,
pp 144-148.
Sanders JO, Rockwood CA Jr, Curtis RJ: Fractures and dislocation of the humeral shaft and shoulder, in Rockwood CA Jr, Wilkins KE, Beaty JH (eds): Fractures in Children, ed 4. Philadelphia, PA, Lippincott-Raven, 1996, vol 3, pp 937-939.
Question 64
What nerve is most at risk during placement of the anterolateral portal in elbow arthroscopy?
Explanation
REFERENCES: O’Driscoll SW, Morrey BF: Elbow arthroscopy, in Morrey BF (ed): The Elbow. Philadelphia, PA, Lippincott, Williams and Wilkins, 1994, pp 21-34.
Field LD, Altchek DW, Warren RF, O’Brien SJ, Skyhar MJ, Wickiewicz TL: Arthroscopic anatomy of the lateral elbow: A comparison of three portals. Arthroscopy 1994;10:602-607.
Question 65
A 15-year-old wrestler sustains an abduction, hyperextension, and external rotation injury to his right shoulder. The MRI scan findings shown in Figures 27a and 27b are most consistent with Review Topic
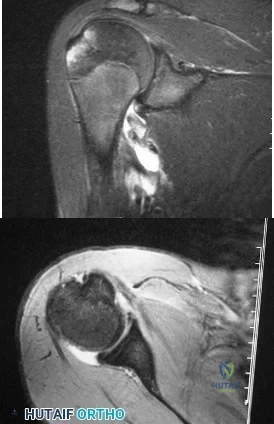
Explanation
Question 66
Figures below show the radiographs, and the CT obtained from a 58-year-old woman who underwent cementless left total hip arthroplasty. Nine months after surgery, she continued to have groin pain when actively flexing her hip. She has trouble walking up stairs and getting out of her car. What is the most likely diagnosis?

Explanation
Groin pain after total hip replacement has a number of possible causes, and an exact diagnosis may remain elusive in some patients. Infection should be ruled out with laboratory studies and, if indicated, diagnostic aspiration of the hip joint. Implant loosening should be evaluated by plain radiograph and bone scan, if indicated. Synovitis resulting from wear debris should be considered in patients with polyethylene liners who experience late-onset symptoms or in any patient with a metal-on-metal bearing. This patient's symptoms are classic for iliopsoas tendonitis. Physical examination usually reveals pain and weakness with resisted hip flexion. A cross-table lateral radiograph and CT show that the anterior edge of the acetabulum protrudes beyond the anterior wall, thereby acting as a source of iliopsoas tendon irritation. In such cases, acetabular component revision and repositioning are indicated. Fluoroscope-guided iliopsoas cortisone injection can help to establish the diagnosis and relieve groin pain. If the acetabular component is well positioned, then iliopsoas tenotomy should be considered.
Question 67
A 47-year-old man is seen in consultation in the ICU after being admitted and treated emergently for a dissecting aortic aneurysm. Current examination reveals generalized weakness of the lower extremities with a significant decrease in pain and temperature sensation from approximately the waist down. Proprioception is maintained. What is the most likely diagnosis at this time? Review Topic
Explanation
Question 68
Figures 1 and 2 are the radiographs of a 24-year-old male wrestler who underwent surgery for recurrent shoulder dislocations using coracoid autograft. At his first postoperative visit, the patient complains of decreased sensation on the lateral aspect of his forearm. The patient’s symptoms are most likely due to injury of the
Explanation
Question 69
A 16-year-old girl has had anterior leg pain and a mass for the past 8 months. Figures 2a and 2b show a radiograph and an H & E histologic specimen. Which of the following disorders is believed to be a precursor of this lesion?
Explanation
REFERENCE: Springfield DS, Rosenberg AE, Mankin HJ, et al: Relationship between osteofibrous dysplasia and adamantinoma. Clin Orthop 1994;309:234-244.
Question 70
A 45-year-old man is seen in the emergency department after returning from a 2-hour airplane flight. He is reporting severe pain in his right leg but has no trouble moving his ankle, leg, or knee. Venous doppler testing reveals no evidence of deep venous thrombosis. He is placed on IV cephazolin but continues to worsen. On the third day in the hospital he has increased pain, some respiratory distress, and trouble maintaining his blood pressure. His leg takes on the appearance seen in Figure 15. An urgent MRI scan shows thickening of the subcutaneous tissues and superficial swelling in the leg but no evidence of an abscess. What is the next most appropriate step in management? Review Topic

Explanation
Question 71
A 66-year-old man has a high-grade angiosarcoma of the right tibia. A radiograph is shown in Figure 43. Treatment should consist of
Explanation
REFERENCE: Simon MA, Springfield DA: Surgery for Bone and Soft Tissue Tumors. Philadelphia, PA, Lippincott-Raven, 1998, ch 29.
Question 72
What is the primary reason for including the ilium in the distal fixation of long instrumentation constructs in adult scoliosis?
Explanation
REFERENCES: Islam NC, Wood KB, Transfeldt EE, et al: Extension of fusions to the pelvis in idiopathic scoliosis. Spine 2001;26:166-173.
Emami A, Deviren V, Berven S, et al: Outcome and complications of long fusions to the sacrum in adult spine deformity: Luque-Galveston, combined iliac and sacral screws, and sacral fixation. Spine 2002;27:776-786.
Question 73
What tendon has an intra-articular (instrasynovial) location in the knee joint?
Explanation
REFERENCES: Kimura M, Shirakura K, Hasegawa A, Kobayashi Y, Udagawa E: Anatomy and pathophysiology of the popliteal tendon area in the lateral meniscus: 1. Arthroscopic and anatomical investigation. Arthroscopy 1992;8:419-423.
Arnoczky SP, Skyhar MJ, Wickiewicz TL: Basic science of the knee, in McGinty JB (ed): Operative Arthroscopy. New York, NY, Raven Press, 1991, pp 155-182.
Question 74
A 77-year-old woman who underwent total knee arthroplasty 16 years ago now reports pain, swelling, and notable crepitation with range of motion. AP, lateral, and Merchant radiographs are shown in Figures 54a through 54c. What is the most likely diagnosis?
Explanation
REFERENCES: Poss R (ed): Orthopaedic Knowledge Update 3. Park Ridge, IL, American Academy of Orthopaedic Surgeons, 1990, pp 590-593.
Leopold SS, Berger RA, Patterson L, et al: Serum titanium level for diagnosis of a failed metal-backed patellar component. J Arthroplasty 2000;15:938-943.
Frymoyer JW (ed): Orthopaedic Knowledge Update 4. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1993, pp 613-614.
Question 75
.What is the most appropriate treatment if instability is present at the time of evaluation?
Explanation

Question 76
Which of the following findings helps to distinguish between stress fractures of the tibia and shin splints?
Explanation
After activity, pain persists longer with tibial stress fractures.
DISCUSSION: Anterior tibial pain can often be difficult to diagnose. A bone scan showing the tibial cortex in a diffuse, longitudinal orientation is consistent with shin splints compared to a more discreet, localized uptake more commonly seen with a stress fracture. Bone stress injuries are due to cyclical overuse of the bone. They are relatively common in athletes and military recruits but are also seem in otherwise healthy people who have recently started new or intensive physical activity. Diagnosis of bone stress injuries is based on the patient’s history of increased physical activity and on imaging findings.
The general symptom of a bone stress injury is stress-related pain. Bone stress injuries are difficult to diagnose based only on a clinical examination because the clinical symptoms may vary depending on the phase of the pathophysiological spectrum in the bone stress injury. Imaging studies are needed to ensure an early and exact diagnosis. If the diagnosis is made early, most bone stress injuries heal well without complications.
REFERENCES: Mubarak SJ, Gould RN, Lee YF, et al: The medial tibial stress syndrome: A cause of shin splints. Am J Sports Med 1982;10:201-205.
Knobloch K, Yoon U, Vogt PM: Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int 2008:29:671-676.
Kiuru MJ, Pihlajamaki HK, Ahovuo JA: Bone stress injuries. Acta Radiol 2004;45:317-326.
Question 77
Figures 1 and 2 display the radiographs obtained from a woman who had volar plating of the distal radius 8 months earlier. Two days ago, she noticed she could not actively extend her thumb. What is the most appropriate treatment that would restore active thumb extension?
Explanation
Although the fracture is aligned in anatomic position, prominence of a least one of the distal screws is evident on the lateral radiographic view. The prominent screw is the most likely cause of the EPL tendon rupture. If the patient chooses surgical treatment, the best option would be removal of the offending hardware combined with extensor indicis proprius to EPL tendon transfer. Intercalary grafting would also be an acceptable option. If the tendon transfer were to be performed alone, the prominent screw(s) could rupture the transferred tendon as well. Also, it is rarely possible to repair the EPL tendon primarily in such cases, because this rupture is an attrition type. Casting would obviously not provide any benefit in this situation, and IP arthrodesis would not be the first surgical treatment option. This problem can be avoided by using shorter screws or not placing screws in plate holes that direct screws into the third dorsal extensor compartment. Intraoperative fluoroscopy and special views, such as the carpal shoot-through view, are useful for avoiding this complication.
Question 78
Figures 1 through 5 show the radiographs obtained from a 37-year-old man who has a 10-year history of right, ulnar-sided wrist pain and a volar ulnar prominence with wrist supination. Approximately 20 years ago, he had a forearm injury that was definitively treated in a long arm cast. What surgical treatment option is most likely to improve his symptoms and maintain pronosupination?

Explanation
The patient sustained a radial shaft fracture with subsequent apex volar malunion. As a result, his distal ulna subluxates volarly with wrist supination. Radiographs of the wrist reveal minimal arthritic changes. The most appropriate treatment option is to surgically correct his radial shaft malunion, which would indirectly address his DRUJ instability. A DRUJ ligament reconstruction or triangular fibrocartilage complex repair could be used to augment DRUJ stability; however, they might be unnecessary after correction of the radial shaft malunion. A DRUJ ligament reconstruction alone would not achieve stability of the DRUJ joint and maintain full wrist pronosupination. An ulnar head implant arthroplasty would not be reliable in eliminating the instability or the pain. Similarly, a one-bone forearm procedure might
improve the patient's pain and instability but at the cost of abnormal wrist and forearm mechanics and kinematics.
Question 79
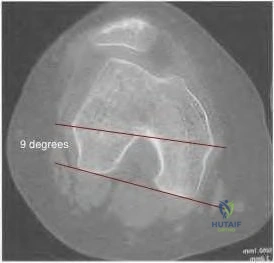
98 degrees (range, 0 degrees to 9 degrees). In knees with varus joint lines
Explanation
Question 80
Which of the following mechanisms of inhibition has been linked to cigarette smoking and lumbar spinal fusion?
Explanation
REFERENCE: Daftari TK, Whitesides TE Jr, Heller JG, et al: Nicotine on the revascularization of bone graft: An experimental study in rabbits. Spine 1994;19:904-911.
Question 81
- A 40-year old man has limited, painful motion in dorsiflexion at the metatarsophalangeal (MTP) joint of the right great toe, despite nonsurgical treatment. Radiographs show dorsal and medial osteophytes and minimal narrowing of the articular space. Treatment should consist of
Explanation
Question 82
Figure 23 shows the radiograph of a 55-year-old man who underwent a total hip arthroplasty 5 years ago. Management should now consist of
Explanation
REFERENCES: Lewallen DG, Berry DJ: Periprosthetic fracture of the femur after total hip arthroplasty: Treatment and results to date, in Cannon WD Jr (ed): Instructional Course Lectures 47. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1998, pp 243-249.
Bethea JS, DeAndrade JR, Fleming LL, Lindenbaum SD, Welch RB: Proximal femoral fractures following total hip arthroplasty. Clin Orthop 1982;170:95-106.
Question 83
Which of the following represents a contraindication for interspinous process decompression for the treatment of lumbar spinal stenosis? Review Topic
Explanation
Question 84
A 14-year-old girl has had progressive heel pain for the past several months. Based on the radiograph, MRI scan, and biopsy specimens shown in Figures 37a through 37d, treatment should include
Explanation
blood-filled spaces with bland fibrous connective tissue septa. The stroma has histiocytes, fibroblasts, scattered giant cells, hemosiderin, and occasional inflammatory cells. Treatment of these lesions consists of extended curettage, plus or minus the use of adjuvants (liquid nitrogen, phenol, argon beam coagulation), and finally filling the bone void (allograft or other bone substitute).
REFERENCES: Gibbs CP Jr, Hefele MC, Peabody TD, et al: Aneurysmal bone cyst of the extremities: Factors related to local recurrence after curettage with a high-speed burr. J Bone Joint Surg Am 1999;81:1671-1678.
Ramirez AR, Stanton RP: Aneurysmal bone cyst in 29 children. J Pediatr Orthop 2002;22:533-539.
Question 85
A construction worker sustained a comminuted calcaneus fracture 2 years ago. He now reports progressive hindfoot pain with the recent onset of anterior ankle pain. A lateral hindfoot radiograph is shown in Figure 31. Treatment should consist of
Explanation
REFERENCES: Carr JB, Hansen ST, Benirschke SK: Subtalar distraction bone block fusion for late complications of os calcis fractures. Foot Ankle 1988;9:81-86.
Myerson M, Quill GE Jr: Late complications of fractures of the calcaneus. J Bone Joint Surg Am 1993;75:331.
Question 86
As reflected by the SF-36 scores, patients with which of the following conditions demonstrate the most disability in physical function?
Explanation
REFERENCE: Pollak AN, McCarthy ML, Bess RS, et al: Outcomes after treatment of high-energy tibial plafond fractures. J Bone Joint Surg Am 2003;85:1893-1900.
Question 87
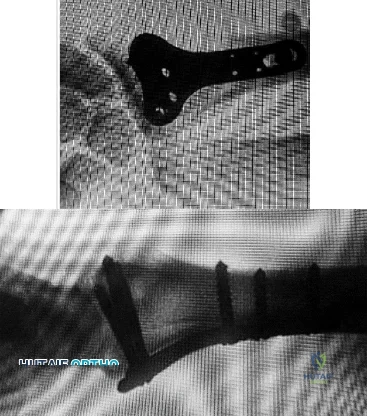
During total shoulder replacement for rheumatoid arthritis, fracture of the humeral shaft occurs. An intraoperative radiograph shows a displaced short oblique fracture at the tip of the prosthesis. At this point, the surgeon should
Explanation
REFERENCES: Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-1346.
Boyd AD Jr, Thornhill TS, Barnes CL: Fractures adjacent to humeral protheses. J Bone Joint Surg Am 1992;74:1498-1504.
Petersen SA, Hawkins RJ: Revision of failed total shoulder arthroplasty. Orthop Clin North Am 1998;29:519-533.
Question 88
Figures 87a and 87b are the radiographs of an 18-year-old pedestrian who was struck by a car. During intramedullary nailing, it is difficult to maintain proper alignment. Poller blocking screws placed in the proximal fragment at which position(s) relative to the nail can help prevent the typical deformity?

Explanation
Question 89
Figure 62a and Figure 62b
Explanation
Figure 58 reveals a posttraumatic valgus deformity. Correction of valgus with lateral soft-tissue release places tension on the peroneal nerve, resulting in an increased risk for nerve palsy. Figures 59a (lateral view) and 59b (Merchant view) illustrate juvenile rheumatoid arthritis with tibiofibular fusion and lateral patellar dislocation. Chronic patellar dislocation is associated with contracture of the lateral retinacular soft tissues and increased risk for patellar subluxation or dislocation after TKA. Extensor mechanism realignment, possibly including tibial tubercle osteotomy and/or proximal soft-tissue realignment, may be required during TKA to centralize the extensor mechanism. Figures 60a (anteroposterior [AP] view) and 60b (lateral view) reveal a fused knee in full extension.
TKA after fusion is associated with multiple complications including skin necrosis, infection, and instability. The skin is contracted because of limited knee motion and has multiple scars (Figure 60c). Mobilization of the skin during and after knee arthroplasty can place excess tension on the soft tissues, resulting in skin necrosis and infection. Treatment consisting of prompt debridement and soft-tissue coverage, usually with medial gastrocnemius muscle transposition, is required. Figure 61 shows a knee with prior tibial tubercle fixation and marked patella infera. Shortening of the patellar ligament is associated with restricted knee motion. This may necessitate more extensile exposure using tibial tubercle osteotomy or rectus snip during TKA to obtain adequate surgical exposure. The inferior position of the patella can cause impingement between the patellar component and tibial insert, resulting in anterior knee pain. Restoring a more normal position of the patella may necessitate distal positioning of the femoral component as well as tibial tubercle osteotomy with proximal recession of the osteotomized tibial tubercle. Figures 62a (AP view of the distal femur) and 62b (AP view of the proximal femur) show a posttraumatic deformity with a large retained intramedullary rod. There is a varus distal femoral deformity that is not severe enough to necessitate extra-articular corrective osteotomy. However, intramedullary hardware precludes use of conventional intramedullary instrumentation, so computer navigation or patient-specific cutting guides will be necessary to orient the bone cuts and avoid implant malalignment.
Question 90
The best candidate for a reverse total shoulder arthroplasty is a patient with rotator cuff tear arthropathy with Review Topic
Explanation
Question 91
A 22-year-old swimmer underwent thermal capsulorrhaphy treatment for recurrent anterior subluxation. Following 3 weeks in a sling, an accelerated rehabilitation program allowed him to return to swimming in 3 1/2 months. While practicing the butterfly stroke, he sustained an anterior dislocation. He now continues to have symptoms of anterior instability and has elected to have further surgery. Surgical findings may include a
Explanation
REFERENCES: Abrams JS: Thermal capsulorrhaphy for instability of the shoulder: Concerns and applications of the heat probe. Instr Course Lect 2001;50:29-36.
Hecht P, Hayashi K, Lu Y, et al: Monopolar radiofrequency energy effects on joint capsular tissue: Potential treatment for joint instability. An in vivo mechanical, morphological, and biochemical study using an ovine model. Am J Sports Med 1999;27:761-771.
Question 92
Figures 3a and 3b show the MRI scans of a patient with neck pain. What is the most likely diagnosis?
Explanation
REFERENCES: Kim HW, Weinstein SL: Spine update: The management of scoliosis in neurofibromatosis. Spine 1997;22:2770-2776.
Funasaki H, Winter RB, Lonstein JB, et al: Pathophysiology of spinal deformities in neurofibromatosis: An analysis of seventy-one patients who had curves associated with dystrophic changes. J Bone Joint Surg Am 1994;76:692-700.
Question 93
A 21-year-old football player who sustained a direct blow to the posterior hindfoot while making a cut is unable to bear weight on the injured foot. Examination reveals tenderness and swelling of the great toe metatarsophalangeal (MTP) joint. Radiographs are shown in Figures 9a and 9b. What is the most likely diagnosis?
Explanation
REFERENCES: Rodeo SA, et al: Diastasis of bipartite sesamoids of the first metatarsophalangeal joint. Foot Ankle 1993;l4:425-434.
Rodeo SA, O’Brien S, Warren RF, et al: Turf toe: An analysis of metatarsal joint sprains in professional football players. Am J Sports Med 1990;18:280-285.
Question 94
Deep anterior compartment
Explanation
Question 95
During total hip arthroplasty, what characteristic of irradiated (10 Mrad) and subsequently melted highly cross-linked polyethylene should provide a more wear-resistant construct than traditional gamma- irradiated (2.5-4 Mrad)-in-air polyethylene mated with the same head?
Explanation
Highly cross-linked polyethylene makes material resistant to adhesive wear. Abrasive wear from third bodies does not decrease wear. The fatigue strength of such material is inferior to that of traditional polyethylene, and its resistance to creep is the same, if not lower, than that of traditional polyethylene.
Question 96
An elite gymnast injured her ankle in an awkward dismount 36 hours ago. Examination reveals weakness on single leg step-up. A clinical photograph of the medial ankle is shown in Figure 15. Plain radiographs are normal. To help confirm the diagnosis, the next step in evaluation should consist of
Explanation
REFERENCES: Lutter LD, Mizel MS, Pfeffer GB (eds): Orthopaedic Knowledge Update: Foot and Ankle. Rosemont, IL, American Academy of Orthopaedic Surgeons, 1994, pp 307-317.
Rosenberg ZS, Cheung Y, Jahss MH, Noto AM, Norman A, Leeds NE: Rupture of the posterior tibial tendon: CT and MR imaging with surgical correlation. Radiology 1988;169:229-235.
Question 97
Figure 16 shows the clinical photograph of a 3-month-old infant with a foot deformity that has been nonprogressive since birth. Examination reveals that the deformity corrects actively and with passive manipulation. There is no associated equinus. Management should consist of
Explanation
REFERENCE: Farsetti P, Weinstein SL, Ponseti IV: The long-term functional and radiographic outcomes of untreated and non-operatively treated metatarsus adductus. J Bone Joint Surg Am 1994;76:257-265.
Question 98
- A right-handed, 53 year old man reports pain in the left shoulder following a fall on an abducted externally rotated shoulder 3 months ago. Examination reveals pain on elevation and tenderness localized to the anterior aspect of the shoulder. Results of the lift-off test are inconclusive due to limited internal rotation. Figure 2 shows the T1-weighted axial image from an MRI-arthrogram. Treatment should include
Explanation
Question 99
A 44-year-old man sustains the injury shown in Figures 1 through 3. What is the most appropriate treatment?

Explanation
Reduction, either open or closed, with internal fixation (pinning) is the recommended treatment for the majority of these injuries. Closed reduction with pinning is most often performed for acute injuries. Open reduction with pinning is performed for those injuries that cannot be reduced by closed means or those with a delayed presentation. Four cases of successful closed reduction and splinting, all performed upon presentation in the emergency department, have been described by Storken and associates, but the authors note that their review of three prior reports uncovered cases of secondary dislocation, which required surgical stabilization. One of the dislocations occurred 4 months after the reduction. They assert that an indication for primary ORIF is a CMC dislocation associated with major fractures. Primary arthrodesis can be considered in cases with severe intra-articular comminution, but this procedure substantially limits the ability of the hand to increase and decrease the transverse metacarpal arch, which is an important functional movement. It can also lead to osteoarthritis of the triquetrohamate joint. Suspension arthroplasty has been described for old fracture-dislocations of the fifth CMC joint, using a partial slip of the extensor carpi ulnaris.








Question 100
- A 32-year-old has diffuse pain, weakness, and limited overhead motion in the shoulder as a result of falling on his outstretched arm 2 months ago. Examination reveals medial scapular winging, and an electromyogram shows denervation of the long thoracic nerve. Management should consist of
Explanation
