Extensor Tendon Realignment and Intrinsic Rebalancing in the Rheumatoid Hand
Key Takeaway
Ulnar drift in the rheumatoid hand requires meticulous surgical correction to restore biomechanical balance. This comprehensive guide details the step-by-step execution of extensor tendon realignment, intrinsic muscle rebalancing, and metacarpophalangeal joint synovectomy. For severe deformities with joint subluxation, interposition arthroplasty is discussed. Emphasizing precise soft-tissue handling, tendon centralization, and structured postoperative rehabilitation, these techniques aim to halt deformity progression, alleviate pain, and optimize hand function in patients with inflammatory arthropathies.
INTRODUCTION AND BIOMECHANICAL PRINCIPLES
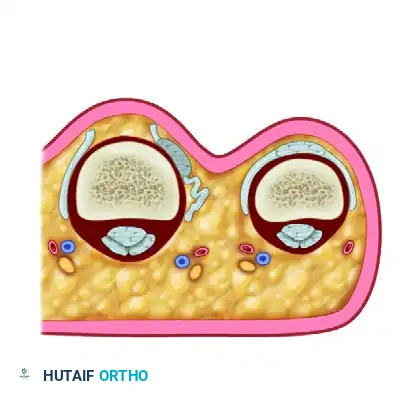
The rheumatoid hand frequently presents with a complex, progressive deformity characterized by volar subluxation and ulnar drift of the metacarpophalangeal (MCP) joints. This pathognomonic cascade is initiated by chronic synovitis, which distends the joint capsule, attenuates the collateral ligaments, and destroys the articular cartilage. As the radial sagittal band becomes attenuated by the expanding synovial pannus, the extensor digitorum communis (EDC) tendon subluxates into the ulnar valley between the metacarpal heads.
Once the extensor tendon falls ulnar to the axis of rotation, it ceases to function as an MCP joint elevator and instead becomes a paradoxical deforming force, exacerbating both ulnar deviation and volar subluxation. Concurrently, the intrinsic muscles—particularly the ulnar intrinsics—contract and shorten, further tethering the proximal phalanx into ulnar deviation. The long flexor tendons, acting across the palmar aspect of the joint, also bowstring ulnarly, exerting a massive palmar and ulnar-directed vector that ultimately leads to frank MCP joint dislocation.
Surgical intervention via extensor tendon realignment and intrinsic rebalancing is indicated for mild to moderate deformities where the articular cartilage remains largely preserved and the joint is passively correctable. In advanced stages with fixed dislocations and severe joint destruction, soft-tissue rebalancing alone is insufficient, necessitating interposition arthroplasty.
Clinical Pearl: The primary goal of soft-tissue reconstruction in the rheumatoid hand is not merely cosmetic correction, but the restoration of biomechanical balance to prevent the inexorable progression toward fixed dislocation. Early synovectomy and tendon centralization can significantly prolong the native lifespan of the MCP joints.
PREOPERATIVE PREPARATION AND POSITIONING
Patient Evaluation
A thorough preoperative clinical and radiographic evaluation is mandatory. The surgeon must assess the passive correctability of the MCP joints. If the joints are stiff, fixed, or demonstrate severe architectural destruction on radiographs (e.g., complete loss of joint space, periarticular erosions, or cystic changes), soft-tissue realignment is contraindicated, and the patient should be templated for implant arthroplasty.
Anesthesia and Positioning
- Anesthesia: Regional anesthesia (supraclavicular or axillary brachial plexus block) is preferred, providing excellent intraoperative conditions and prolonged postoperative analgesia.
- Positioning: The patient is positioned supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) after exsanguination with an Esmarch bandage.
SURGICAL TECHNIQUE: EXTENSOR TENDON REALIGNMENT
1. Incision and Venous Preservation
Meticulous handling of the dorsal skin and venous network is critical to prevent postoperative edema, which can severely compromise hand rehabilitation.
- Marking: Prior to exsanguination and tourniquet inflation, use a sterile skin pencil to outline the major dorsal veins. These veins typically course through the "valleys" between the metacarpal heads. Marking them while they are engorged ensures they can be identified and preserved after they collapse under tourniquet ischemia.
- Incision: Make a transverse dorsal incision directly over the metacarpal heads, extending from the second to the fifth metacarpal.
- Dissection: Carefully elevate the dorsal skin flaps. Identify the previously marked dorsal veins and retract them gently using vessel loops. Preservation of these veins and the accompanying dorsal lymphatics is paramount.
2. Extensor Hood Release and Arthrotomy
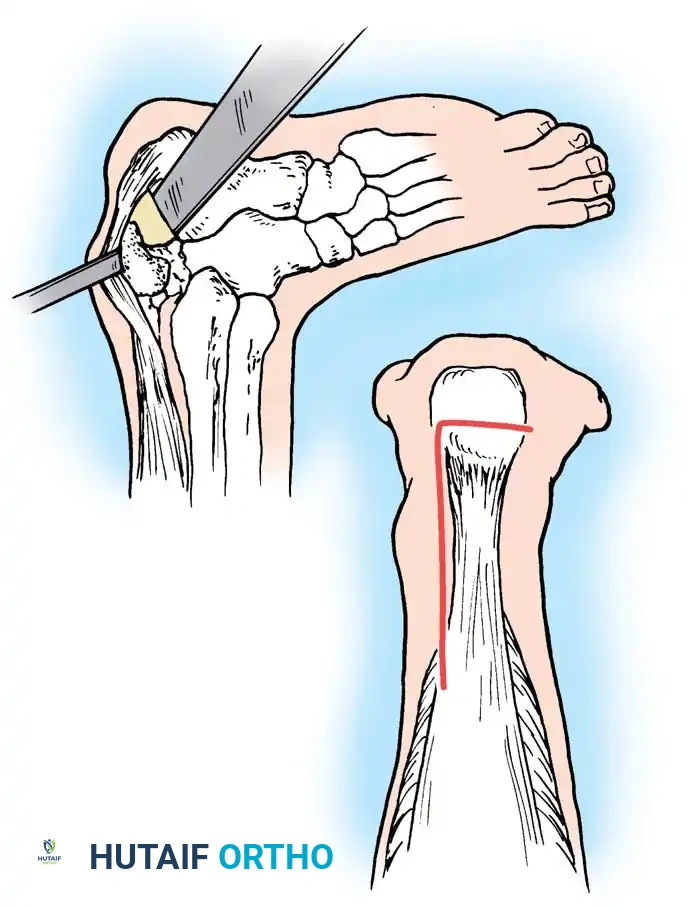
- Radial Incision: Enter each MCP joint through a longitudinal incision on the radial side of the extensor hood, parallel to the extensor tendon.
- Mobilization: Dissect the extensor hood from the underlying joint capsule. This step is crucial to release the ulnarly displaced extensor mechanism, allowing it to be mobilized back to the dorsal midline.
- Capsulotomy: Make a longitudinal incision in the dorsal capsule.
> Surgical Warning: Ensure the capsular incision does not lie directly deep to the tendon incision. Offsetting these incisions prevents adherence of the extensor tendon to the joint capsule during the healing phase, which would severely restrict active flexion.
3. Metacarpophalangeal Joint Synovectomy
Synovectomy is the cornerstone of halting disease progression.
* Dissect between the synovial pannus and the joint capsule.
* Excise the hypertrophic synovium comprehensively. Pay special attention to the synovium herniating through the capsule and draping over the dorsal neck of the metacarpal. In severe rheumatoid cases, the dorsal capsule is often so attenuated and infiltrated by disease that the majority of it must be excised alongside the synovium.
* Abrasion Technique: The synovium frequently burrows under the collateral ligaments at the metacarpal head. Remove this inaccessible tissue by abrasion: wrap two or three layers of a rough gauze sponge over the point of a curved hemostat and vigorously sweep it through the recesses beneath the collateral ligaments.
4. Extensor Mechanism Centralization
To correct the ulnar drift, the extensor tendon must be centralized and secured.
* Ulnar Relaxing Incision: Make a secondary longitudinal incision on the ulnar side of the central tendon. This acts as a relaxing incision, freeing the tethered extensor mechanism and permitting it to be repositioned dorsally over the metacarpal head. This ulnar incision is left open to heal by secondary intention.
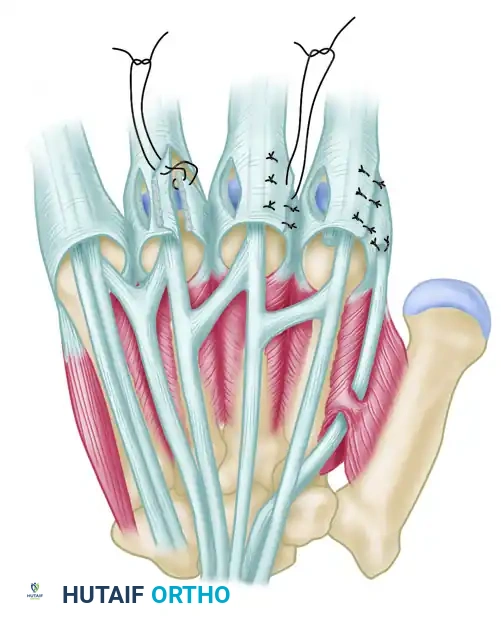
* Radial Imbrication: Realign the extensor tendon directly over the MCP joint. Close the radial-sided incision in the extensor hood using nonabsorbable sutures (e.g., 4-0 braided polyester or nylon). The edges of the radial hood should be overlapped (imbricated) to tighten the radial sagittal band and securely hold the tendon in its centralized position.
Figure 73-23 (Parts 3 & 4): The incision on the radial side of the hood is closed after its edges are overlapped (imbricated) to maintain the centralized position of the extensor tendon.
5. Extensor Tendon Tenodesis
In cases where the extensor mechanism is highly unstable, simple imbrication may fail over time.
* Perform a tenodesis of the extensor tendon to the base of the proximal phalanx.
* This can be achieved using small suture anchors placed into the dorsal base of the proximal phalanx, or by passing nonabsorbable sutures through transosseous drill holes. This anchors the centralized tendon, preventing recurrent ulnar subluxation during active flexion.
SURGICAL TECHNIQUE: INTRINSIC REBALANCING
Intrinsic muscle contracture is a primary driver of ulnar deviation. Rebalancing these forces is essential for long-term success.
The Flatt Transfer
The Flatt transfer involves releasing the deforming ulnar intrinsic insertions and transferring them to the radial side of the adjacent digits to provide a corrective radial pull.
- Ulnar Release: Through the existing exposure, identify the ulnar intrinsic tendon insertion on the ulnar side of the central tendon. Make an incision to release this insertion completely.
- Mobilization: Free the ulnar intrinsic insertion from its surrounding adhesions.
- Transfer: Reroute the released ulnar intrinsic tendon and suture it to the capsule or the radial collateral ligament on the radial side of the MCP joint of the adjacent ulnar finger.

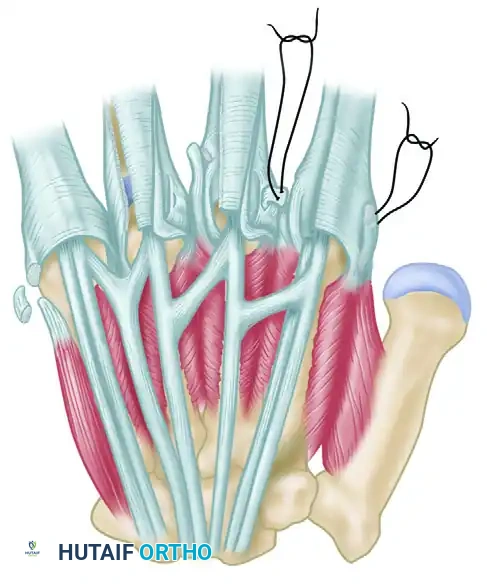

Figure 73-24: The Flatt transfer of released ulnar intrinsics to the radial side of adjacent digits. The ulnar intrinsic insertion is freed and sutured to the radial capsule of the adjacent finger to counteract ulnar drift.
Additional Rebalancing Procedures
- Abductor Digiti Quinti (ADQ) Release: The ADQ is a powerful ulnar deviator of the little finger. Excise a segment of the ADQ tendon to relieve its ulnar pull on the fifth digit.
- First Dorsal Interosseous (FDI) Advancement: To increase the radial pull on the index finger, the FDI tendon can be shortened or advanced distally.
- Extensor Indicis Proprius (EIP) Transfer: When the index finger exhibits marked, recalcitrant ulnar deviation, the EIP tendon can be detached from its insertion, routed radially, and transferred to the first dorsal interosseous muscle or the radial collateral ligament to reinforce radial deviation and extension.
SEVERE ULNAR DRIFT AND METACARPOPHALANGEAL DISLOCATION
Pathomechanics of Advanced Deformity
In severe, end-stage ulnar drift, one or more MCP joints will frankly dislocate volarly. Interestingly, a biomechanical trade-off occurs in the rheumatoid hand: MCP joint dislocation effectively releases the longitudinal soft-tissue tension across the ray, thereby decreasing tension distally and partially protecting the proximal interphalangeal (PIP) joint from swan-neck or boutonnière deformities. Conversely, if the PIP joints dislocate first, the MCP joints are partially protected.
Despite this, the long flexor tendons remain a massive deforming force. Whether they remain within their sheaths or subluxate ulnarly, they exert a continuous ulnar and palmarly directed force that perpetuates the MCP joint dislocation. In these advanced cases, soft-tissue realignment is futile due to the loss of the articular fulcrum. Surgery must address the destroyed metacarpal head and the contracted surrounding ligaments.
Interposition Arthroplasty
Function of a dislocated, arthritic MCP joint is best restored via resection arthroplasty and interposition of a prosthesis.
- Implant Selection: Numerous designs exist, but the Swanson silicone implant remains the gold standard with the most extensive long-term clinical data. Pyrolytic carbon implants are a modern alternative showing promising results regarding wear characteristics, though they require competent collateral ligaments.
- Surgical Principles: The metacarpal head is resected, decompressing the joint. The medullary canals of the metacarpal and proximal phalanx are broached. The silicone spacer is inserted, acting not as a true hinge, but as a dynamic spacer that maintains alignment while an encapsulating fibrous scar forms around it. It is this fibrous capsule, guided by the implant, that ultimately provides joint stability and permits motion.
- Outcomes: The average expected range of motion at the MCP joint following Swanson arthroplasty is approximately 55 degrees. While this is less than a normal joint, it occurs within the critical functional arc required for activities of daily living. Pain relief is highly reliable.
Pitfalls and Complications in Arthroplasty:
* Infection: Occurs in 0% to 3% of cases. Active infection is an absolute contraindication to implant arthroplasty.
* Implant Breakage: Reported rates vary wildly from 2% to 82%. However, obvious or occult fractures (often visible on tomograms) frequently do not impair function, as the encapsulating scar tissue continues to provide stability.
* Subluxation/Dislocation: Subluxation occurs in roughly 20% of cases, and frank dislocation in 5%.
* Grommets: Metal sleeves or grommets designed to diminish abrasion at the bone-prosthesis interface have not been shown to significantly decrease the implant fracture rate.
Contraindications to Arthroplasty: Severe bone loss precluding implant seating, poor skin coverage that prohibits tension-free closure, irreparable flexor/extensor tendon damage, and active infection. Patients must be counseled that results deteriorate over time, and revision surgery may eventually be required.
POSTOPERATIVE CARE AND REHABILITATION
The success of extensor tendon realignment and intrinsic rebalancing relies heavily on strict adherence to a specialized postoperative rehabilitation protocol.
Phase 1: Immobilization (Weeks 0–2)
- Immediately postoperatively, the hand is placed in a bulky, non-compressive dressing reinforced with a volar plaster splint.
- The wrist is positioned in 20 to 30 degrees of extension.
- The MCP joints are immobilized in full extension (0 degrees) with a slight radial deviation bias to counteract the preoperative ulnar drift.
- The PIP and DIP joints are left free to allow immediate active motion, preventing distal stiffness and promoting tendon gliding.
- Strict elevation is maintained to minimize edema.
Phase 2: Suture Removal and Dynamic Splinting (Weeks 2–6)
- At 2 weeks, the bulky dressing and skin sutures are removed.
- The patient is transitioned to a custom-fabricated thermoplastic dynamic extension splint. This splint supports the MCP joints in extension and radial deviation during rest but allows active flexion against rubber-band traction.
- The splint must be worn continuously (day and night) to protect the imbricated radial sagittal bands and the transferred intrinsic tendons while they heal.
- Supervised hand therapy is initiated, focusing on active MCP flexion and active-assisted extension.
Phase 3: Weaning and Strengthening (Weeks 6–12)
- At 6 weeks, the dynamic splint is gradually weaned during the day but is often continued at night for an additional 4 to 6 weeks to prevent recurrence of the ulnar drift.
- Progressive strengthening exercises are introduced.
- Patients are educated on joint protection techniques and ergonomic modifications to avoid placing excessive ulnar-directed forces on the reconstructed digits during daily activities.
By meticulously executing these surgical steps and adhering to a rigorous rehabilitation protocol, the orthopedic surgeon can effectively restore biomechanical alignment, alleviate pain, and significantly improve the functional capacity of the rheumatoid hand.
You Might Also Like