Free Vascularized Fibular Graft: A Masterclass in Complex Long Bone Reconstruction

Key Takeaway
This masterclass details free vascularized fibular graft reconstruction for segmental bone defects. We cover comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution, including precise fibular harvest and allograft integration. Learn critical pearls, pitfalls, and postoperative care, ensuring successful outcomes for complex long bone defects.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater and the rigorous academic discourse surrounding one of the most elegant and biologically sound solutions for large segmental bone defects: the free vascularized fibular graft (FVFG). Today, we are embarking on a deep dive into an orthoplastic procedure that demands meticulous planning, precise surgical technique, and a profound understanding of both microsurgery and advanced orthopaedic principles. When executed correctly, the FVFG offers our patients a durable, living reconstruction with true regenerative capacity, far superior to many conventional methods. For decades, addressing significant intercalary bone defects—those massive gaps left after wide tumor resections, severe high-energy trauma, or recalcitrant osteomyelitis—has presented a formidable reconstructive challenge.
Traditional methods, while possessing historical merit and specific narrow indications, often fall short when applied to massive defects exceeding five to eight centimeters. Prosthetic implants, massive structural allografts, and allograft-prosthetic composites have historically been associated with unacceptably high rates of long-term complications and ultimate failure. We are routinely confronted with catastrophic issues such as deep periprosthetic infection, allograft non-union, fatigue fracture of the necrotic bone, and aseptic loosening of the implants. While these conventional modalities offer immediate structural support and permit early mobilization, they fundamentally lack the inherent biologic activity required to adapt, remodel, and regenerate in response to mechanical stress. They rely on the agonizingly slow and often incomplete process of creeping substitution, leaving a permanent necrotic core susceptible to failure.
Distraction osteogenesis via Ilizarov or Taylor Spatial Frame methodologies, while representing a true biologic reconstruction, is typically limited to small to medium intercalary defects. It is an incredibly prolonged and psychologically taxing process for the patient, often requiring up to two months for just a single centimeter of mature bone elongation. Pin-tract complications are ubiquitous, patient compliance is absolutely critical to success, and distraction osteogenesis cannot simultaneously address the massive soft tissue defects that are frequently concomitant with the bone loss seen in oncologic resections or severe open trauma. Furthermore, the reported experience regarding its safety, efficacy, and timeline in the immediate post-oncologic setting—especially when adjuvant chemotherapy or radiation is required—remains somewhat limited and fraught with delayed consolidations.
This is precisely where the vascularized autogenous fibular graft demonstrates its absolute superiority. Since its pioneering introduction by Taylor and colleagues in the mid-1970s, it has become the undisputed cornerstone for reconstructing massive intercalary bone defects and for performing complex resection-arthrodeses. Its inherent, unmatched advantage lies in its ability to exploit the biology of normal primary fracture healing. By preserving the intrinsic blood supply, the FVFG promotes immediate osteogenesis and rapid remodeling, bypassing the vulnerable phase of creeping substitution. The vascularized fibula allows for robust graft incorporation into the host bone, even in severely compromised recipient beds devastated by previous surgeries, chronic infection, or radiation therapy. Its unique morphologic characteristics, combined with a robust dual blood supply, offer unparalleled versatility in our reconstructive armamentarium.

Detailed Surgical Anatomy and Biomechanics
Before a single incision is made, a comprehensive, three-dimensional understanding of the fibular anatomy and its surrounding neurovascular topography is absolutely paramount. The fibula is a long, slender, tubular bone, making it an exceptional cortical strut for reconstructing long-bone defects. In a healthy adult, it can reach a width of 1.5 to 2.0 centimeters and a total length of up to 35 centimeters, yielding a highly versatile harvestable segment of 25 to 30 centimeters for free tissue transfer. Its cross-sectional geometry is dynamically variable; it is typically quadrilateral in its superior aspect and transitions to a more triangular or teardrop shape inferiorly. This specific morphology allows the surgeon to intricately match bone segments of the upper extremity, such as the humerus, radius, and ulna, or to precisely dowel the graft into the medullary canal of larger load-bearing bones in the lower extremity, such as the femur and tibia.
Neurovascular Relationships and Dissection Corridors
The fibula is circumferentially enveloped by distinct muscle groups on its lateral, anteromedial, and posterior aspects, serving as the rigid origin for the four intermuscular septa of the lower leg. The most critical structures that the reconstructive microsurgeon must meticulously identify and protect during harvest are the common peroneal nerve and the peroneal vascular bundle. The common peroneal nerve, a major division of the sciatic nerve, courses obliquely and wraps around the fibular neck, transitioning from the popliteal fossa to travel superficially over the fibula just distal to the proximal tibiofibular joint. It then abruptly divides into the superficial and deep peroneal nerves. Iatrogenic injury to this nerve during the proximal dissection or osteotomy will lead to a devastating, often irreversible foot drop. We must meticulously identify, neurolyse, and protect this nerve throughout the entirety of the proximal dissection phase.
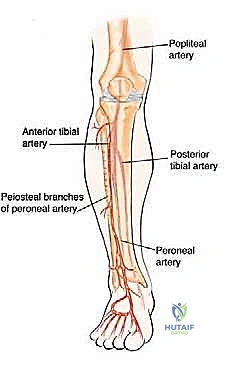
The primary blood supply and venous drainage of the fibular diaphysis are intimately and inextricably related to the peroneal artery and its two accompanying venae comitantes. These critical vessels follow a longitudinal course parallel to the posterior aspect of the fibula, lying deep within the deep posterior compartment of the leg. They are securely nestled in a protective muscular envelope between the flexor hallucis longus (FHL) and the tibialis posterior muscles. Accessing this vascular bundle requires a precise surgical approach, typically utilizing the lateral intermuscular septum as a reliable anatomic guide to navigate safely between the lateral (peroneal) and superficial posterior (soleus/gastrocnemius) compartments without compromising the vascular perforators.


The Dual Vascularization System
The fibula boasts a highly robust dual blood supply, which is the fundamental biological basis for its viability as a free tissue transfer. The first component is the endosteal blood supply, which is primarily based on the principal nutrient artery. This critical vessel typically branches from the peroneal artery approximately 6 to 14 centimeters distal to the tibioperoneal trunk bifurcation. It enters the middle third of the fibular diaphysis via the nutrient foramen and immediately divides into ascending and descending intramedullary branches. This high-pressure system is incredibly robust and is responsible for sustaining the inner two-thirds of the diaphyseal cortex, ensuring immediate osteocyte survival upon revascularization.
The second component is the periosteal blood supply, derived from a rich arcade of 8 to 9 distinct periosteal branches originating from the peroneal artery. These vessels are mostly concentrated in the middle third of the diaphysis and form a dense network over the bone surface. They supply the outer one-third of the cortex and are absolutely vital, especially in the initial stages of graft incorporation and callus formation at the host-graft junction. When complex reconstructive configurations require transverse osteotomies through the mid-diaphysis to create multiple cortical struts—such as in the "double-barrel" fibula technique for femoral reconstruction—the periosteal vessels are inevitably transected. In these scenarios, the viability of the folded bone segments relies entirely on the preservation of the endosteal system and the meticulous handling of the intramedullary vasculature.
Furthermore, the peroneal artery serves as the source of 4 to 6 distinct septocutaneous or musculocutaneous perforating vessels that pass through the posterior intercrural septum. These perforators supply the cutaneous territory lateral to the fibula, allowing for the simultaneous harvest of a vascularized skin paddle (the osteocutaneous flap). This skin paddle is invaluable not only for addressing concomitant soft tissue defects but, critically, for providing a reliable, easily accessible external monitor for flap viability in the immediate postoperative period. The peroneal artery also provides numerous muscular branches, specifically to the soleus and flexor hallucis longus muscles. Portions of these muscles can be intentionally included with the osseous flap as a "chimeric" transfer to obliterate dead space or cover exposed hardware in complex, multidimensional defects.

Exhaustive Indications and Contraindications
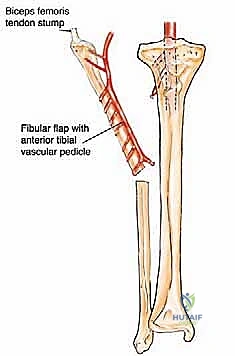
The decision to utilize a free vascularized fibular graft is not made lightly; it is reserved for the most challenging clinical scenarios where conventional bone grafting techniques are destined to fail. The primary indication is the reconstruction of massive segmental bone defects, generally defined as those exceeding 5 to 6 centimeters in length. These defects most frequently result from the wide en bloc resection of aggressive primary bone sarcomas (such as osteosarcoma, Ewing sarcoma, or chondrosarcoma), radical debridement of chronic, recalcitrant osteomyelitis, or massive bone loss following high-energy ballistic or crush trauma. In the pediatric population, the FVFG is particularly valuable as it can be harvested with the proximal fibular physis (based on the anterior tibial vessels) to provide a reconstruction that maintains longitudinal growth potential, a critical factor in preserving limb length equality.
In the realm of orthopaedic oncology, our institutional protocol often dictates a staged approach for high-grade sarcomas. This involves an initial wide oncologic resection followed by the placement of a temporary antibiotic-impregnated cement spacer and rigid stabilization. The definitive biologic reconstruction with a vascularized fibula is then carried out approximately 12 to 24 months post-resection, provided the patient has completed all adjuvant therapies and demonstrates no evidence of local tumor recurrence or distant metastases. This staged approach allows for rigorous oncologic surveillance before committing the patient and the surgical team to a highly complex, resource-intensive biologic reconstruction. Alternatively, for benign aggressive tumors (like giant cell tumors) or low-grade malignancies, immediate single-stage reconstruction is frequently indicated and highly successful.
Another major indication is the treatment of congenital pseudarthrosis of the tibia (CPT) or recalcitrant atrophic non-unions of long bones that have failed multiple previous interventions. In these hostile biologic environments, the introduction of heavily vascularized, immunocompetent living bone is often the only viable limb-salvage option. The FVFG can be used as an inlay graft, an onlay strut, or, most commonly in the lower extremity, combined with a massive structural allograft in what is known as the Capanna technique. This hybrid reconstruction leverages the immediate mechanical strength and anatomic sizing of the allograft while utilizing the vascularized fibula to provide the essential biologic engine for rapid union and long-term remodeling.

Indications and Contraindications Table
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | Segmental defects > 6 cm (Tumor, Trauma, Infection) | Conventional non-vascularized grafts resorb or fail to incorporate over large distances. |
| Absolute Indications | Congenital Pseudarthrosis of the Tibia (CPT) | Requires introduction of healthy, vascularized tissue to overcome the biologically inert dysplastic environment. |
| Relative Indications | Avascular Necrosis of the Femoral Head (AVN) | Free fibula core decompression provides structural support and revascularization to prevent collapse (though less common now with advanced arthroplasty). |
| Absolute Contraindications | "Peronea Arteria Magna" Vascular Variant | The peroneal artery is the dominant blood supply to the foot; harvest will result in catastrophic foot ischemia. |
| Absolute Contraindications | Severe Peripheral Vascular Disease (PVD) | Inadequate recipient vessels for anastomosis or compromised donor leg perfusion. |
| Relative Contraindications | Poor Patient Compliance / Severe Psychiatric Illness | The postoperative protocol requires strict non-weight-bearing and intense rehabilitation; non-compliance guarantees failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning is the absolute cornerstone of success for a procedure of this magnitude. The surgical team must develop a meticulous, step-by-step roadmap for both the recipient site preparation and the donor site harvest. The evaluation begins with an exhaustive assessment of the recipient site. High-resolution plain radiography, Computed Tomography (CT), and Magnetic Resonance Imaging (MRI) are essential to provide comprehensive, three-dimensional information regarding the exact dimensions (length, medullary diameter, and cortical thickness) of the bone defect. MRI is particularly crucial in oncologic cases to determine the required margins of resection and to assess any associated soft tissue defects that will require coverage via an osteocutaneous or chimeric flap design.
Following dimensional analysis, vascular mapping of the recipient site is mandatory. Angiography, CT Angiography (CTA), or Magnetic Resonance Angiography (MRA) must be performed to identify suitable, high-flow recipient vessels for the microvascular anastomosis. The surgeon must map out the major arteries and veins outside the zone of injury or radiation, assess their patency, evaluate for post-traumatic intimal hyperplasia, and identify potential sites for end-to-end or end-to-side anastomoses. In cases of chronic osteomyelitis or severe trauma, the local vessels may be heavily scarred or thrombosed, necessitating the planned use of interpositional vein grafts (e.g., from the great saphenous vein) to reach healthy recipient vessels outside the zone of injury.

Equally critical is the evaluation of the donor site, typically the contralateral leg to allow for a simultaneous two-team surgical approach. Plain radiography of the entire lower extremity is performed to exclude any occult fibular deformity, previous healed fractures, or benign lesions that would compromise the structural integrity of the graft. However, the most critical step is the vascular assessment. A Doppler ultrasound is used as an initial screening tool to verify adequate triphasic pulses in both the posterior tibial and dorsalis pedis arteries. We routinely perform a lower extremity equivalent to the palmar Allen's test to evaluate the deep and superficial plantar vascular arches.
If Doppler studies are even slightly inconclusive, or if there is any clinical suspicion of vascular compromise, formal CTA or conventional angiography is strictly mandatory. This is a non-negotiable safety step; the surgeon must confirm a robust collateral circulation to the foot via the anterior and posterior tibial arteries before considering fibular harvest. We must rule out the presence of a "peronea arteria magna"—a congenital variant where the anterior or posterior tibial arteries are hypoplastic or absent, and the peroneal artery provides the dominant blood supply to the foot. Harvesting the fibula and its peroneal pedicle in such a patient would result in catastrophic, limb-threatening ischemia of the foot.


Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the FVFG is typically performed using a simultaneous two-team approach to minimize total operative and ischemia time. Patient positioning is dictated by the location of the recipient site; for upper extremity or anterior lower extremity defects, the patient is positioned supine with a bump under the ipsilateral hip of the donor leg to internally rotate the limb. A sterile tourniquet is applied to the proximal thigh of the donor leg. The harvest begins with a longitudinal incision along the lateral aspect of the leg, following the palpable posterior border of the fibula. If a skin paddle is required, it is centered over the junction of the middle and distal thirds of the fibula, where the septocutaneous perforators are most reliably located.
The initial dissection involves identifying the plane between the peroneus longus and brevis muscles anteriorly and the soleus muscle posteriorly. The superficial peroneal nerve must be identified and protected in the proximal-anterior aspect of the incision. As the dissection deepens, the lateral intermuscular septum is followed down to the fibular shaft. The surgeon must meticulously preserve any cutaneous perforators traveling through this septum if an osteocutaneous flap is planned. The anterior compartment musculature (extensor digitorum longus, extensor hallucis longus, and tibialis anterior) is sharply elevated off the anterior fibular face, taking extreme care to protect the deep peroneal nerve and anterior tibial vessels lying on the interosseous membrane.


Osteotomies and Pedicle Dissection
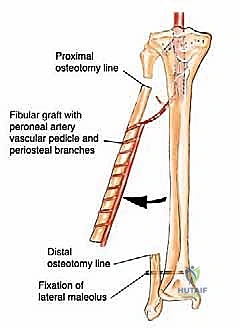
Once the anterior and lateral aspects of the fibula are exposed, the osteotomy sites are marked. It is an absolute biomechanical rule to preserve a minimum of 6 to 8 centimeters of the distal fibula to maintain the integrity of the distal tibiofibular syndesmosis and prevent catastrophic ankle valgus instability. Similarly, 6 to 8 centimeters of the proximal fibula must be preserved to protect the common peroneal nerve and maintain knee stability. The osteotomies are performed using an oscillating saw or a Gigli saw, ensuring the periosteum is not stripped from the graft segment. Following the osteotomies, the fibular segment is gently retracted laterally.
This lateral retraction exposes the deep posterior compartment. The interosseous membrane is divided longitudinally. The tibialis posterior muscle is then carefully elevated off the posterior aspect of the fibula. It is at this critical juncture that the peroneal artery and its venae comitantes are visualized. The vessels are traced proximally to their origin at the tibioperoneal trunk to maximize pedicle length. Distally, the vessels are ligated just below the distal osteotomy site. A cuff of flexor hallucis longus (FHL) muscle is routinely left attached to the posterior and medial aspects of the fibula to protect the intimately associated vascular pedicle and the vital periosteal blood supply. Once the recipient site is fully prepared and recipient vessels are isolated, the tourniquet is deflated, hemostasis is achieved, and the pedicle is finally ligated and divided, initiating the ischemia time.

Graft Inset, Fixation, and Microvascular Anastomosis
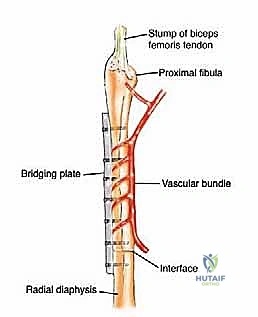
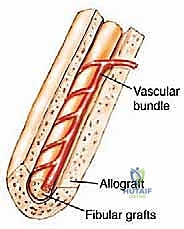
The transfer and inset of the fibula demand precise mechanical engineering. For massive lower extremity defects, we highly advocate the Capanna technique—combining the vascularized fibula with a massive structural allograft. The allograft provides immediate axial load-bearing capacity and a perfect anatomic match for the host bone, while the intramedullary vascularized fibula provides the biologic engine for union and hypertrophy. The fibula is carefully threaded through the reamed medullary canal of the allograft. Rigid internal fixation is absolutely paramount; micro-motion at the host-graft junction will shear the delicate neo-vascularity and lead to non-union. We typically utilize long, heavy-duty bridging locking plates that span the entire construct, securing the host bone, the allograft, and the fibula simultaneously. Intramedullary nailing can be used, but extreme care must be taken not to compress or injure the vascular pedicle during nail insertion.


Once rigid skeletal fixation is achieved, the operating microscope is brought into the field for the microvascular anastomosis. The ischemia time should ideally be kept under two to three hours. The peroneal artery is typically anastomosed end-to-end or end-to-side to a major recipient artery (e.g., the superficial femoral, popliteal, or posterior tibial artery) using 8-0 or 9-0 nylon sutures. The two venae comitantes are anastomosed to the deep venous system, frequently utilizing mechanical venous coupler devices to ensure a perfectly patent, non-thrombogenic intima-to-intima repair. Following clamp release, immediate perfusion of the graft must be confirmed by observing brisk bleeding from the medullary canal and the muscle cuff, and by assessing the capillary refill of the skin paddle.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, the free vascularized fibular graft is a highly complex procedure with a recognized complication profile. Complications can be broadly categorized into intraoperative, early postoperative, and late postoperative events. Intraoperative complications primarily involve iatrogenic injury to the neurovascular structures. Injury to the common peroneal nerve during proximal dissection can result in permanent foot drop, necessitating future tendon transfer procedures (e.g., Bridle procedure). Inadvertent injury to the peroneal pedicle or avulsion of the nutrient artery during osteotomy can critically compromise the graft, potentially forcing the surgeon to abandon the free transfer and convert to a non-vascularized technique or an alternative flap.
Early postoperative complications are dominated by microvascular thrombosis. Arterial or venous thrombosis typically occurs within the first 72 hours and presents as a pale, pulseless skin paddle or a congested, engorged paddle, respectively. The incidence of microvascular failure ranges from 5% to 10% in major centers. Immediate return to the operating room for surgical exploration, thrombectomy, and revision of the anastomosis is mandatory. Delay in recognition almost invariably leads to complete flap necrosis. Deep surgical site infection is another devastating early complication, particularly in cases of trauma or prior osteomyelitis. Aggressive serial debridements, targeted intravenous antibiotics, and potentially the application of negative pressure wound therapy are required to salvage the construct.


Late complications are primarily mechanical. Stress fractures of the fibular graft are exceedingly common, occurring in up to 30% to 40% of lower extremity reconstructions before the graft has fully hypertrophied. These fractures often heal with conservative management (casting or bracing) due to the robust vascularity of the graft, which actually stimulates further hypertrophy. Non-union at the host-graft junction occurs in approximately 10% to 15% of cases, often requiring secondary bone grafting (autologous iliac crest) and revision of the internal fixation. Donor site morbidity must also be respected; patients frequently experience transient weakness of the great toe (EHL/FHL tethering), claw toe deformities, and, if the distal osteotomy is performed too low, progressive ankle valgus instability requiring syndesmotic screw fixation or distal tibiofibular synostosis.
Complications and Salvage Strategies Table
| Complication Type | Estimated Incidence | Clinical Presentation | Salvage / Management Strategy |
|---|---|---|---|
| Microvascular Thrombosis | 5% - 10% | Loss of Doppler signal, pale or congested skin paddle within 72h. | EMERGENT return to OR. Thrombectomy, revision of anastomosis, potential use of vein grafts. |
| Graft Stress Fracture | 20% - 40% (Lower Ext) | Sudden onset localized pain, radiographic evidence of fracture line. | Often heals conservatively with protected weight-bearing. May require revision fixation if displaced. |
| Host-Graft Non-Union | 10% - 15% | Persistent pain > 6 months, lack of bridging callus on CT. | Revision rigid fixation, autologous cancellous bone grafting (ICBG), optimization of biology. |
| Ankle Valgus Instability | 5% - 10% | Progressive valgus deformity of the donor ankle, pain with weight-bearing. | Preventative: leave >8cm distal fibula. Salvage: Distal tibiofibular syndesmotic screw or formal arthrodesis. |
| Deep Infection | 5% - 15% | Erythema, purulent drainage, systemic sepsis, elevated CRP/ESR. | Aggressive I&D, hardware retention if stable, culture-directed IV antibiotics, suppressive therapy. |


Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a free vascularized fibular graft is a prolonged, highly structured, and multi-phased process that requires absolute patient compliance and close coordination between
Clinical & Radiographic Imaging Archive