Operative Management of Clavicle and Humeral Nonunions: A Comprehensive Surgical Guide

Key Takeaway
The operative management of clavicle and humeral nonunions requires meticulous surgical technique, rigid internal fixation, and biological optimization. This guide details evidence-based approaches for plate fixation and bone grafting of the clavicle, alongside advanced reconstruction strategies for proximal and diaphyseal humeral nonunions. Key considerations include biomechanical plate positioning, management of osteoporotic bone with locking technology, and the strategic use of structural allografts or arthroplasty in complex salvage scenarios.
Comprehensive Introduction and Patho-Epidemiology
The management of nonunions in the shoulder girdle and humeral diaphysis presents a formidable, multifaceted challenge to the orthopedic surgeon. Successful salvage of these complex clinical scenarios requires a profound understanding of local pathoanatomy, meticulous soft-tissue handling, rigid biomechanical fixation, and the optimization of the biological environment. While the overall incidence of nonunion following upper extremity fractures is relatively low compared to the lower extremity, the functional devastation experienced by the patient is profound, often resulting in chronic pain, severe limitation of activities of daily living, and profound psychological distress. This masterclass delineates the evidence-based surgical techniques for addressing nonunions of the clavicle, proximal humerus, and humeral shaft, integrating classical principles of osteosynthesis with contemporary advancements in locking plate technology, intramedullary augmentation, and arthroplasty.
A nonunion is classically defined by the United States Food and Drug Administration (FDA) as a fracture that is at least nine months post-injury and has not shown any radiographic signs of healing for three consecutive months. However, in the upper extremity, particularly the proximal humerus and clavicle, rigid adherence to this timeline is often clinically impractical. According to Crosby et al., a nonunion of the proximal humerus is defined clinically and radiographically when there is an absolute cessation of healing at three months from the time of injury. At this juncture, the biological potential for spontaneous union has typically been exhausted, and surgical intervention is warranted.
The patho-epidemiology of upper extremity nonunions is categorized into three distinct biological and mechanical phenotypes: hypertrophic, atrophic, and oligotrophic. Hypertrophic nonunions are characterized by abundant callus formation ("elephant foot" appearance) and are primarily the result of mechanical instability in the presence of adequate vascularity; their treatment mandates rigid stabilization to allow the existing biological potential to bridge the gap. Atrophic nonunions exhibit no callus formation, sclerotic bone ends, and a biologically inert environment, often secondary to severe soft tissue stripping, high-energy comminution, or systemic factors such as smoking and diabetes. These require both mechanical stabilization and profound biological augmentation, typically via autogenous bone grafting. Oligotrophic nonunions represent an intermediate state, lacking significant callus but retaining some vascularity, usually requiring both mechanical and biological optimization.
The "Diamond Concept" of fracture healing is paramount in the salvage of these nonunions. The surgeon must simultaneously address the presence of osteogenic cells (via autograft or bone marrow aspirate), an osteoconductive scaffold (cancellous bone, structural allograft, or synthetic matrices), osteoinductive growth factors (bone morphogenetic proteins, though off-label in many upper extremity applications), mechanical stability (locking plates, dual plating), and adequate vascularity (preservation of the soft tissue envelope). Failure to address even one of these pillars exponentially increases the risk of a recalcitrant nonunion.
Detailed Surgical Anatomy and Biomechanics
A masterful command of the surgical anatomy and regional biomechanics is the foundational prerequisite for the operative management of upper extremity nonunions. The shoulder girdle and arm operate as a highly coordinated kinetic chain, subjecting the osseous structures to immense, multi-planar forces that complicate achieving stable fixation.
The Clavicle
The clavicle acts as the sole osseous strut connecting the axial skeleton to the upper extremity. It is an S-shaped bone, convex anteriorly in its medial two-thirds and concave anteriorly in its lateral third. This unique morphology subjects the midshaft to complex bending, torsional, and axial compressive loads during shoulder elevation and upper extremity weight-bearing. The muscular forces acting on a clavicular nonunion are significant deforming factors: the sternocleidomastoid pulls the medial fragment superiorly and posteriorly, while the weight of the arm and the pull of the pectoralis major displace the lateral fragment inferiorly and medially, resulting in the classic shortened and translated nonunion deformity.
The neurovascular proximity is the primary hazard in clavicular surgery. The subclavian vein, subclavian artery, and the cords of the brachial plexus lie directly posterior and inferior to the middle third of the clavicle, separated only by the thin subclavius muscle. Superior plating acts as a tension band against the gravitational pull of the arm; however, anteroinferior plating offers distinct anatomical and biomechanical advantages. Placing the plate on the anteroinferior surface allows the surgeon to direct the drill bits and screws in a superoposterior direction, safely directing instrumentation away from the vital subclavicular structures. Furthermore, anteroinferior plates are less prominent beneath the skin, significantly reducing postoperative hardware irritation.
The Proximal Humerus
The proximal humerus consists of the humeral head, the greater and lesser tuberosities, and the surgical neck. The blood supply is notoriously tenuous, primarily derived from the ascending branch of the anterior circumflex humeral artery (the arcuate artery) and supplemented by the posterior circumflex humeral artery. Fractures at the anatomical neck or severe multi-part fractures frequently disrupt this blood supply, precipitating avascular necrosis and subsequent atrophic nonunion.
Biomechanically, the proximal humerus is subjected to massive, opposing forces from the rotator cuff. The supraspinatus and infraspinatus exert a superior and posterior pull on the greater tuberosity, the subscapularis pulls the lesser tuberosity medially, and the pectoralis major exerts a powerful medial and internal rotation force on the humeral shaft. In the setting of osteoporotic bone—where the cancellous metaphyseal bone is resorbed, leaving only a thin "egg-shell" cortex—these forces easily overcome standard fixation. The subchondral bone of the humeral head is often the only region of dense bone remaining, necessitating the use of fixed-angle locking plates with multiple divergent screws to maximize purchase.
The Humeral Shaft
The humeral diaphysis transitions from a cylindrical cross-section proximally to a triangular cross-section distally. Unlike the lower extremity, the humerus does not experience cyclical axial loading during normal ambulation; instead, it is subjected to massive torsional and bending forces. The arm acts as a long lever, making fracture site motion notoriously difficult to control with external splintage alone, contributing to the 10% nonunion rate.
The radial nerve is the most critical anatomical structure in humeral shaft surgery. It courses from the posterior cord of the brachial plexus, enters the posterior compartment through the triangular interval, and spirals around the posterior humerus in the spiral groove, accompanied by the profunda brachii artery. It pierces the lateral intermuscular septum approximately 10 to 14 centimeters proximal to the lateral epicondyle to enter the anterior compartment. In humeral shaft nonunions, the radial nerve is frequently encased in dense fibrous scar tissue or callus, making iatrogenic injury a profound risk during surgical exposure.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for an upper extremity nonunion requires a meticulous risk-benefit analysis, weighing the patient's physiological age, functional demands, medical comorbidities, and the specific pathoanatomy of the pseudarthrosis.
| Clinical Scenario | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Clavicle Nonunion | Intractable pain, shoulder weakness, neurovascular compromise (thoracic outlet symptoms), skin tenting, shortening > 2cm. | Active untreated infection, medically unfit for anesthesia. | Asymptomatic nonunion in a low-demand patient, active smoking (requires cessation). |
| Proximal Humerus Nonunion | Painful pseudarthrosis, loss of overhead function, progressive varus collapse, hardware failure, articular penetration of screws. | Florid osteomyelitis, profound medical instability, paralyzed deltoid and rotator cuff. | Severe Parkinson's disease, Charcot arthropathy, massive irreparable cuff tear (steers toward RTSA rather than ORIF). |
| Humeral Shaft Nonunion | Gross instability, painful motion at nonunion site, radial nerve palsy (progressive), angular deformity > 20 degrees. | Active deep space infection (requires staged management), terminal illness. | Painless pseudarthrosis in elderly/sedentary patients (amenable to Sarmiento bracing), severe osteoporosis without structural graft options. |
In physiologically younger patients with adequate bone stock, joint preservation via Open Reduction and Internal Fixation (ORIF) is the absolute primary goal. Conversely, in the elderly, low-demand patient with severe osteoporotic bone and multiple medical comorbidities, the diminished function caused by a painless pseudarthrosis may be preferable to the significant risks of open reduction, extensive blood loss, and prolonged anesthesia. In such cases, the use of a custom-molded, lightweight functional orthosis may allow sufficient activities of daily living to avoid further surgical intervention.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful nonunion surgery. The surgeon must not approach these cases as routine acute fractures; they are complex reconstructive procedures that demand a comprehensive strategy for exposure, debridement, fixation, and biological augmentation.
Advanced Imaging and Workup
Standard orthogonal radiographs (true anteroposterior, scapular Y, and axillary lateral views for the shoulder; AP and lateral for the humerus) are mandatory to assess deformity, hardware failure, and bone loss. However, a computed tomography (CT) scan with 3-dimensional reconstructions is the gold standard for evaluating the exact geometry of the nonunion, the degree of sclerosis, and the available bone stock for screw purchase. If an atrophic nonunion is present, an infectious workup including Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP), and a complete blood count is required to rule out an indolent infection (e.g., Cutibacterium acnes in the shoulder).
Digital Templating and Graft Selection
Digital templating software must be utilized to select the appropriate implant length and trajectory. For the humeral shaft, the plate must be long enough to achieve a minimum of eight cortices of fixation proximal and distal to the nonunion. For the clavicle, a minimum of six cortices per side is required. The surgeon must preoperatively determine the need for structural augmentation. If a large cortical defect is anticipated, an intramedullary fibular allograft or a structural iliac crest bone graft must be ordered and available in the operating room.
Patient Positioning
For clavicle and proximal humerus nonunions, the patient is placed in the beach-chair position. A small bump is placed between the scapulae to allow the shoulder girdle to fall posteriorly, aiding in the restoration of clavicular length and providing access to the anterior shoulder. The head must be rigidly secured in a neutral position to prevent cervical spine hyperextension and brachial plexus traction. For humeral shaft nonunions, the position depends on the approach. Anterolateral approaches are performed supine with the arm on a hand table. Posterior approaches require the lateral decubitus or prone position, with the arm draped free over a radiolucent post. In all cases, the ipsilateral anterior or posterior iliac crest must be prepped and draped for autogenous bone graft harvesting.
Step-by-Step Surgical Approach and Fixation Technique
Clavicular Nonunion: Plating and Grafting
- Surgical Approach: Make an incision parallel with and just distal to the clavicle. This infraclavicular approach avoids placing the scar directly over the hardware, minimizing wound breakdown and hardware prominence.
- Dissection and Exposure: Incise the platysma. Carefully identify, mobilize, and protect the supraclavicular nerve branches to prevent postoperative chest wall numbness or the formation of painful neuromas. Incise the periosteum and meticulously strip it from the anterior and inferior aspects of the bone. Preserve the superior and posterior periosteal attachments to maintain residual vascularity.
- Preparation of the Nonunion Site: Exsect all intervening fibrous tissue and pseudarthrosis membrane. Use a high-speed burr or sharp osteotome to open the sclerotic medullary canals of both the medial and lateral fragments. Resection must continue until punctate bleeding (the "paprika sign") is observed, ensuring a viable biological bed for graft incorporation.
- Plate Fixation: Reduce the fracture, restoring anatomical length and rotation. Apply a pre-contoured 3.5-mm reconstruction plate, a dynamic compression plate (DCP), or a modern low-profile, clavicle-specific locking plate to the anteroinferior surface. Ensure at least three bicortical screws (six cortices) are achieved on each side of the nonunion. If a lag screw can be placed across the nonunion site, it should be inserted prior to plate application to achieve absolute interfragmentary compression.
- Bone Grafting: Harvest autogenous cancellous bone from the anterior iliac crest. Pack the graft densely around the nonunion site, particularly filling any inferior or posterior cortical defects.
- Closure: Close the clavipectoral fascia and platysma meticulously over the plate to provide a robust soft-tissue envelope. Close the skin with subcuticular sutures.
Proximal Humerus Nonunion: ORIF vs. Arthroplasty
In physiologically younger patients, joint preservation is the primary goal. Healy et al. demonstrated that the best outcomes are achieved with rigid internal fixation combined with cancellous bone grafting.
Historically, a tension band construction was utilized to neutralize the deforming forces of the rotator cuff. In contemporary practice, locking plates have revolutionized this treatment. The locking plate functions as a fixed-angle construct, offering significantly higher torsional strength and allowing for multiple divergent proximal screw placements. This divergent trajectory maximizes purchase in the subchondral bone. For hypertrophic and oligotrophic nonunions, locking plates augmented with intramedullary fibular allografts provide exceptional structural stability. The allograft acts as an internal strut, preventing varus collapse.
When joint preservation is impossible—due to severe osteopenia, avascular necrosis, or massive articular destruction—shoulder arthroplasty becomes the treatment of choice.
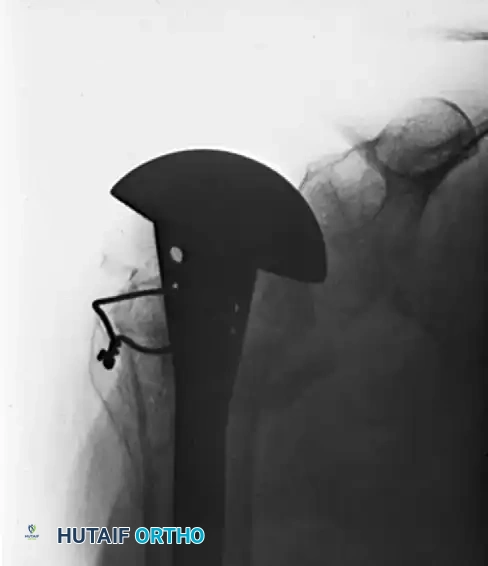
Nonunited fractures at the anatomical neck of the humerus, where the articular segment is devascularized, can be treated by open reduction and the insertion of a hemiarthroplasty prosthesis through the head fragment. The Neer I prosthesis relies heavily on the anatomical healing of the greater and lesser tuberosities around the implant to restore rotator cuff function. Meticulous tuberosity mobilization, heavy non-absorbable suture fixation through the prosthesis fin, and securement to the humeral shaft are critical steps.
In the low-demand elderly patient with a functional deltoid, poor tuberosity bone stock, or concurrent rotator cuff arthropathy, Reverse Total Shoulder Arthroplasty (RTSA) is the highly successful salvage procedure. By medializing the center of rotation and lowering the humerus, RTSA increases the deltoid moment arm, bypassing the need for a functioning rotator cuff.
Humeral Shaft Nonunion: Compression Plating and Structural Augmentation
For the vast majority of humeral diaphyseal nonunions, the gold standard treatment is open reduction, autogenous bone grafting, and dynamic compression plating, yielding up to a 98% union rate.
- Surgical Approach: The posterior approach is highly favored for mid-to-distal third nonunions as it provides an expansive, flat surface for plate application. The triceps is split or reflected to expose the posterior humerus.
- Radial Nerve Management: The radial nerve must be meticulously identified, neurolysed, and protected. It is mobilized from the spiral groove and gently retracted with vessel loops. Extensive scar tissue often distorts its anatomy, requiring tedious micro-dissection.
- Biological Preparation: Radical excision of all fibrous pseudarthrosis tissue is mandatory. The sclerotic bone ends must be freshened until healthy, bleeding bone is encountered. The medullary canal must be recanalized bilaterally using drill bits or curettes.
- Fixation Strategy: A 4.5-mm broad dynamic compression plate (LC-DCP) or a 4.5-mm locking compression plate is applied. Interfragmentary compression is achieved using an articulated tension device or eccentrically placed screws. Dual plating (orthogonal 90-90 configuration) may be utilized in cases of extreme instability.
- Structural Augmentation: In cases of atrophic nonunion with significant cortical defects, an intramedullary fibular allograft is highly recommended. The fibula is impacted into the canal, and screws are passed through the plate, the near cortex, the fibular strut, and the far cortex.
While primary intramedullary (IM) nailing of acute humeral shaft fractures is well-established, exchange nailing for nonunions has not proven successful in the humerus. The humerus lacks the axial compressive forces of gait that stimulate healing in lower extremity exchange nailing, and IM nailing does not reliably control rotational forces. The preferred salvage strategy for failed IM nailing is nail removal, open debridement, compression plating, and copious autogenous bone grafting.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for upper extremity nonunions carries a high risk profile due to the altered anatomy, compromised soft tissue envelope, and poor bone quality.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategy |
|---|---|---|---|
| Radial Nerve Palsy | 5% - 15% (Humeral Shaft) | Iatrogenic traction, entrapment in callus, direct laceration during posterior approach. | Most are transient neuropraxias resolving in 3-6 months. Cock-up splinting. Tendon transfers if no recovery by 12 months. |
| Hardware Failure | 2% - 8% | Inadequate fixation (too few cortices), failure to use locking screws in osteoporotic bone, lack of medial support. | Revision ORIF with longer locking plates, dual plating, intramedullary fibular strut augmentation, and ICBG. |
| Deep Infection | 1% - 5% | Prolonged operative time, poor soft tissue envelope, prior open fracture, smoking, diabetes. | Aggressive serial I&D, hardware removal if unstable, placement of antibiotic cement spacer (Masquelet technique), IV antibiotics. |
| Recalcitrant Nonunion | 2% - 10% | Biological failure (atrophic bed not adequately grafted), persistent mechanical instability, smoking. | Re-evaluate Diamond Concept. Revision with vascularized free fibular graft or massive structural allograft. |
| Adhesive Capsulitis | 10% - 20% (Proximal Humerus) | Prolonged immobilization, excessive surgical trauma, failure to initiate early passive ROM. | Aggressive physical therapy, intra-articular corticosteroid injections, arthroscopic capsular release if refractory. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following nonunion takedown and fixation is a delicate balance between protecting the osteosynthesis construct and preventing profound joint stiffness. The protocol must be individualized based on the rigidity of fixation, bone quality, and the specific anatomical site.
Phase I: Maximum Protection (Weeks 0 to 2)
Immediately postoperatively, the upper extremity is immobilized in a sling or shoulder immobilizer to protect the soft tissue repair and the surgical incision. For clavicle and proximal humerus nonunions, gentle pendulum exercises are initiated within the first 48 hours to prevent adhesive capsulitis. Active range of motion (ROM) of the elbow, wrist, and hand is highly encouraged to reduce edema and prevent distal stiffness. No active forward elevation or external rotation of the shoulder is permitted.
Phase II: Early Motion and Tissue Healing (Weeks 2 to 6)
Once the surgical incisions have healed and sutures are removed, the patient transitions to active-assisted range of motion (AAROM). For proximal humerus fixations, supine forward elevation using a cane or pulleys is initiated. The surgeon must dictate specific ROM limits based on intraoperative stability (e.g., limiting external rotation to 30 degrees to protect tuberosity repairs in hemiarthroplasty). For humeral shaft nonunions treated with rigid broad plating, active ROM of the shoulder and elbow can be cautiously initiated, avoiding any lifting or torsional stress.
Phase III: Progressive Range of Motion (Weeks 6 to 12)
At the 6-week mark, orthogonal radiographs are obtained to assess for early bridging callus and maintenance of hardware position. If clinical and radiographic progression is satisfactory, the sling is discontinued entirely. Patients progress to full active range of motion (AROM) in all planes. Isometric strengthening of the deltoid and rotator cuff may begin. However, dynamic resistance exercises and heavy lifting remain strictly contraindicated until solid osseous union is confirmed.
Phase IV: Strengthening and Return to Function (Weeks 12+)
Once definitive radiographic union is observed—characterized by bridging trabeculae across at least three cortices and obliteration of the fracture line—the patient is cleared for progressive resistance training. Theraband exercises, light weights, and functional kinetic chain integration are emphasized. Patients with physically demanding occupations or athletes typically require 4 to 6 months of dedicated rehabilitation before a full, unrestricted return to heavy labor or contact sports. For patients who underwent RTSA, rehabilitation focuses heavily on deltoid recruitment and compensatory strategies, recognizing that internal rotation and behind-the-back motion may remain permanently limited.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative strategies for upper extremity nonunions is deeply rooted in several landmark biomechanical and clinical studies. The American Academy of Orthopaedic Surgeons (AAOS) guidelines strongly emphasize the necessity of rigid mechanical stability coupled with biological augmentation for diaphyseal nonunions.
Sarmiento's pioneering work on functional bracing established the non-operative standard for acute humeral shaft fractures; however, his long-term data also highlighted that failure to achieve union by 12 weeks with bracing exponentially increases the likelihood of a true pseudarthrosis, necessitating operative intervention. Ring and Jupiter's exhaustive reviews on humeral diaphyseal nonunions cemented the gold standard of the 4.5-mm broad LC-DCP combined with autogenous iliac crest bone grafting, demonstrating union rates exceeding 95% and establishing the futility of exchange nailing in the humerus.
For the proximal humerus, Neer's original classification and subsequent work on hemiarthroplasty laid the foundation for managing devascularized head fragments. Healy et al. provided the definitive evidence that rigid internal fixation with cancellous grafting is superior for joint preservation in younger patients. More recently, the biomechanical superiority of fixed-angle locking plates in osteoporotic bone has been universally validated, drastically reducing the rates of varus collapse and screw cut-out. Furthermore, Boileau and Grammont's development of the Reverse Total Shoulder Arthroplasty (RTSA) has completely revolutionized the salvage of proximal humerus nonunions in the elderly, offering predictable pain relief and functional elevation in scenarios that were previously deemed unsalvageable.
🔗 Read the comprehensive guide: Dual Onlay Graf"
