K-Wire Fixation of Distal Radius Fractures with and without External Fixation
DEFINITION
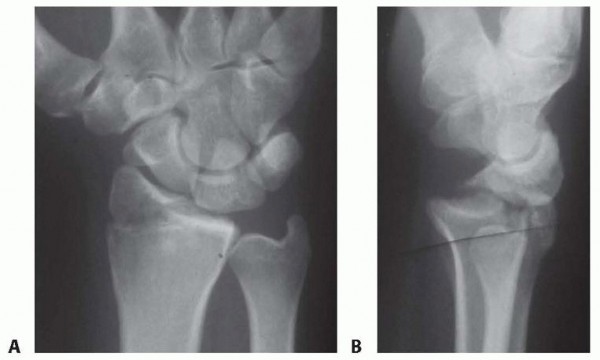
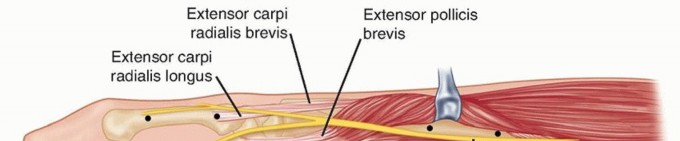
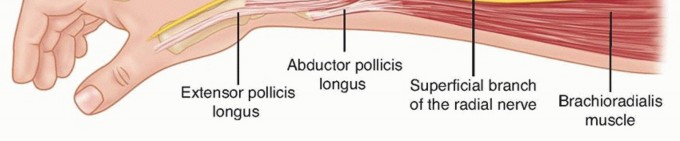
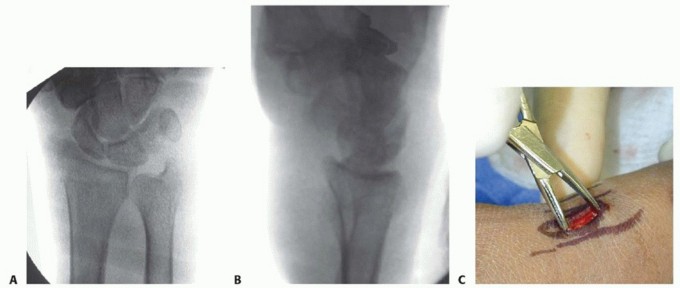
Distal radius fractures occur at the distal end of the bone, originating in the metaphyseal region and often extending to the radiocarpal and distal radioulnar joints (DRUJ).Distal radius fractures can be classified as stable or unstable and extra- or intra-articular to assist in treatment decisions.Fractures may angulate dorsally or volarly and may have significant comminution depending on the energy of the injury and the quality of the bone.Percutaneous pins or K-wires, typically 0.062 or 0.045 inches, can be used for treatment of simple intra-articular or extra-articular fractures with mild comminution and no osteoporosis.Percutaneous pins can aid reduction and stabilize the fragments in a minimally invasive manner.Percutaneous pins can support the subchondral area of the distal radius and maintain the articular reduction in highly comminuted fractures, which is useful when combined with other fixation methods.Smooth percutaneous pins may also be placed across the physis to maintain a reduction in children with minimal risk of a growth arrest.Highly comminuted fractures are more difficult to fix rigidly and often require external and/or internal fixation to maintain alignment during healing.External fixators can be hinged or static and may or may not bridge the wrist joint.K-wire fixation of extra-articular and simple intra-articular fractures has received more support over the last few years after several prospective randomized trials comparing K-wire fixation to volar plating has shown no difference in outcome at 1 year. FIG 1 • Anatomy surrounding the radial sensory nerve branch in the forearm.
ANATOMY
The distal radius consists of three articular surfaces: the scaphoid fossa, the lunate fossa, and the sigmoid notch.Ligamentotaxis aids in the reduction of intra-articular and comminuted fractures.Volar extrinsic ligamentous attachments include the radioscaphocapitate, long radiolunate, and short radiolunate ligaments.Dorsal extrinsic ligamentous attachments include the radiotriquetral ligament.Dorsal and radial to the second metacarpal lie the first dorsal interosseous muscle and the terminal branches of the radial sensory nerve.The distal radial sensory nerve branches lie superficial to the distal radius and should be protected during dissection and pin placement.The radial sensory nerve emerges between the brachioradialis and the extensor carpi radialis longus (ECRL) muscle bellies ( FIG 1).The terminal branches of the lateral antebrachial cutaneous nerve lie superficial to the forearm fascia at the radial wrist.There is a bare spot of bone between the first and second dorsal compartments in the region of the radial styloid.The brachioradialis tendon inserts onto the radial styloid deep to the first dorsal compartment.The ECRL and the extensor carpi radialis brevis (ECRB) lie dorsal to the brachioradialis in the second dorsal compartment.Lister tubercle is dorsal, with the extensor pollicis longus (EPL) tendon on its ulnar side, in the third dorsal compartment.P.253The extensor digitorum communis tendons lie over the dorsal ulnar half of the distal radius in the fourth dorsal compartment.The extensor digiti minimi lies over the DRUJ in the fifth dorsal compartment.
PATHOGENESIS
Distal radius fractures are the most common fractures of the upper extremity in adults, representing about 20% of all fractures seen in the emergency room. 22Mechanism of injury typically is a fall on an outstretched hand with axial loading, but other common histories include motor vehicle accidents or pathologic fractures.Higher energy injuries cause increased comminution, angulation, and displacement.Osteoporosis, tumors, and metabolic bone diseases are risk factors for sustaining pathologic distal radius fractures.In children, fractures typically occur along the physis due to its relative weakness compared to the surroundingligaments.
NATURAL HISTORY
Distal radius fractures needing no reduction and those that are stable after reduction typically recover functional range of motion with minimal long-term sequelae.Three parameters that affect outcome include articular congruity, angulation, and shortening. 21,26Two millimeters or more of articular surface incongruity of the distal radius can lead to degenerative changes, pain and stiffness.Dorsal angulation can lead to decreased range of motion and increased load transfer to the ulna. Radial shortening can lead to decreased range of motion, pain, and ulnar impaction of the carpus.
PATIENT HISTORY AND PHYSICAL FINDINGS
The history of a fall on an outstretched hand is the most common presentation for a patient with a distal radius fracture.Motor vehicle or motorcycle accidents and osteoporosis account for most comminuted fractures. It may be clinically indicated to implement a workup for osteoporosis.Pain, tenderness, swelling, crepitus, deformity, ecchymosis, and decreased range of motion at the wrist are typical symptoms and warrant radiographic evaluation.Physical examination should include the following:Inspection: Evaluate the integrity of the skin, cascade of the digits, direction of displacement, and presence of any swelling.Identify points of maximal tenderness to differentiate between distal radius injuries and carpal or ligamentous injuries.Palpate specific areas of the wrist and hand to differentiate distal intra-articular, DRUJ, and carpal injuries.Two-point discrimination: Higher than normal (5 mm) results in the form of progressive neurologic deficit may signify an acute carpal tunnel syndrome or ulnar neuropathy.Passive finger stretch test to assist with diagnosis of compartment syndrome. EPL tendon function should be evaluated.EPL assessment: Assess the resting position of the thumb interphalangeal joint and the patient's ability to lift the thumb off of a flat surface to determine the continuity of the EPL tendon.Palpation of forearm and elbow to assess for concomitant injury proximally The DRUJ must be assessed for displacement and instability.The bony anatomy must be carefully evaluated to avoid missing minimally displaced fractures, which may displace without treatment.Skin should be assessed to avoid missing an open fracture.Swelling should be monitored to allow for early diagnosis of compartment syndrome.Sensory examination should be monitored for progressive changes, which may represent acute carpal tunnel syndrome.
IMAGING AND OTHER DIAGNOSTIC STUDIES


DIFFERENTIAL DIAGNOSIS
Bony contusion Radiocarpal dislocationScaphoid or other carpal fracture Perilunate or lunate fracture-dislocation Distal ulnar fractureWrist ligament or triangular fibrocartilage complex injury DRUJ injury
NONOPERATIVE MANAGEMENT
Nonoperative treatment consists of splinting or casting for stable fracture patterns using a three-point mold.Fractures amenable to nonoperative treatment include fractures that are stable after reduction with minimal metaphyseal comminution, shortening, angulation, and displacement.Evaluation for secondary displacement weekly for 2 to 3 weeks is critical as the swelling subsides.Unstable patterns will displace if not surgically stabilized.There is little role for nonoperative treatment in highly comminuted fractures.The physiologic age, medical comorbidities, and functional level of the patient should be considered in determining the need for surgical treatment.Early range of motion of the nonimmobilized joints is essential in the nonoperative treatment of all fractures near the wrist to prevent contracture.The cast or splint must not extend past the metacarpophalangeal joints so as to allow digital motion.
SURGICAL MANAGEMENT
Surgical treatments are indicated to prevent malunion and improve pain control, function, range of motion, and to decrease the time of return to function.Surgery is reserved for unstable fractures, including displaced, intra-articular, comminuted, or severely angulated injuries and fractures that displace following attempted closed management.Percutaneous pinning can assist in obtaining and maintaining reduction of displaced fractures with limited comminution in a minimally invasive manner.External fixators maintain radius length but cannot always control angulation and displacement; therefore,supplementation with percutaneous pins is typically performed. 2Conversely, external fixators may augment percutaneous pins and plate fixation when extensive comminution is present.Supplemental external fixation should be considered for fractures with comminution of over 50% of the diameter of the radius on a lateral view or when significant volar cortical comminution is present.External fixation may be used as a neutralization device because the distraction forces decrease soon after fracture reduction.External fixators also are useful for “damage control orthopaedics” to temporarily stabilize wrist fractures, especially for complex, combined, open injuries.For nonbridging external fixation, there must be at least 1 cm of volar cortex intact and adequate fragment sizes to allow proper pin placement.A relative contraindication to pin fixation with or without external fixation is a volar shear injury, which should be reduced and stabilized using a volar plate and screws.
PREOPERATIVE PLANNING
All radiographs should be reviewed before surgery and brought into the operating room.Analysis of the pattern and presumed stability of the fracture fragments determines whether percutaneous fixation, with or without external fixation, is suitable.For intra-articular fractures, the specific fragments to be reduced and fixed must be identified preoperatively to avoid incomplete reduction of the joint surface.The surgeon must be prepared to change his or her management decision intraoperatively if the fracture behavior is different from anticipated. A variety of fixation devices should be available in the operating room.
POSITIONING
The patient is positioned supine on the operating table with a radiolucent arm board. A tourniquet is applied near the axilla with the splint still in place ( FIG 3).Fluoroscopy should be used for confirmation of reduction and fixation throughout the procedure.There must be enough range of motion of the shoulder and elbow to allow standard anteroposterior (AP), lateral, and oblique images.
APPROACH

FIG 3 • Positioning of patient supine on the hand table with tourniquet in place.
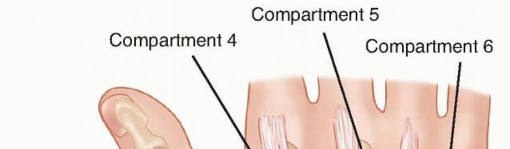

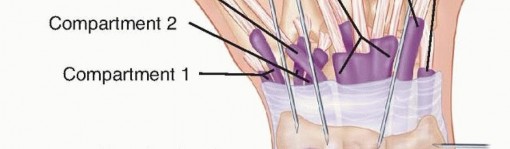
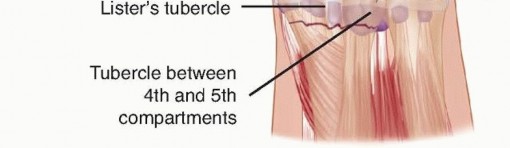
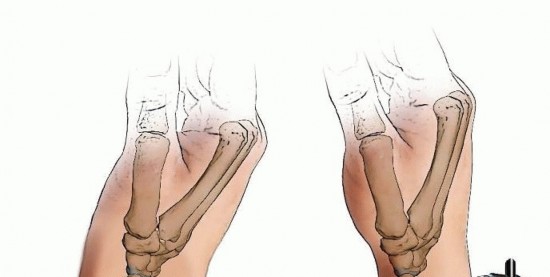
FIG 4 • Areas for K-wire insertion at the distal radius.
TECHNIQUES
Closed Reduction of a Distal Radius Fracture

TECH FIG 1 • Closed reduction over a towel bump using traction and palmar translation.
KAPANDJI TECHNIQUE FOR PERCUTANEOUS PINNING
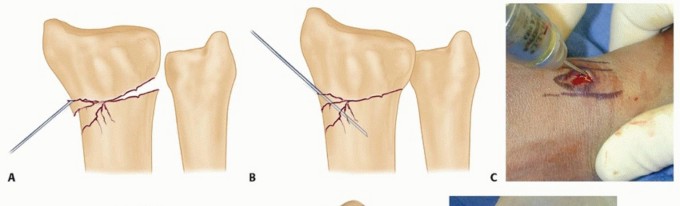
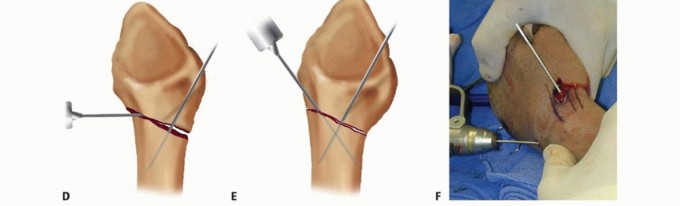
TECH FIG 2 • A. An incision is made over the radial styloid, and a K-wire is manually inserted into the fracture site. B. The wire is levered distally to correct the radial inclination. C. The wire is advanced proximally, using power, into cortical bone. D. An incision is made over Lister tubercle, and a wire is inserted into the fracture site. E,F. The wire is levered distally to correct the dorsal angulation and advanced proximally using power into cortical bone.
Author's Preferred Technique for Percutaneous Pinning
TECH FIG 3 • A,B. PA and lateral views demonstrating reduction of distal radius fracture. C. The incision is made over the radial styloid.(continued)




TECH FIG 3 •(continued)D. A pin is inserted retrograde into the radial styloid. E. PA radiograph demonstrating the course of the radial styloid wire. F. Two radial styloid wires and two dorsoulnar wires are in place. G. PA view showing fixation and the path of the wires. H. Lateral view showing fixation and path of wires. I. Pins are bent, cut, and covered above the skin. The pins are cut just beneath the skin, which is closed with a 5-0 nylon suture. Alternatively, the pins are bent and cut and left outside the skin ( TECH FIG 3I). A dressing and splint are then applied.3. Bridging External Fixator Application
DISTAL PIN PLACEMENT



TECH FIG 4 • A. An incision is made over the second metacarpal base, with reflection of the first dorsal interosseous muscle and radial sensory nerve terminal branches. (The thumb is at the top of the photograph.) B. Diagram showing placement of fixator pins in the shaft of the index and the base of the index and long metacarpals. C. Parallel placement of two metacarpal pins. Proximal Pin Placement and Frame Construction

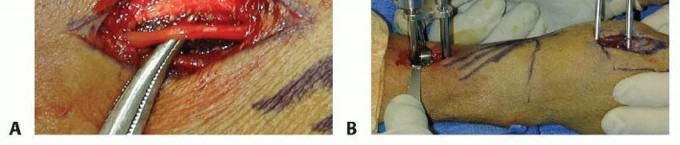
TECH FIG 5 • A. Incision over the radial forearm demonstrating the radial sensory nerve branch deep to the fascia. (The hand is to the right.) B. The double drill guide is placed onto the radius.(continued)


TECH FIG 5 •(continued)C. Final reduction is maintained by the addition of clamps and rods. D. K-wires are used for supplemental fixation when necessary.
NONBRIDGING EXTERNAL FIXATOR APPLICATION
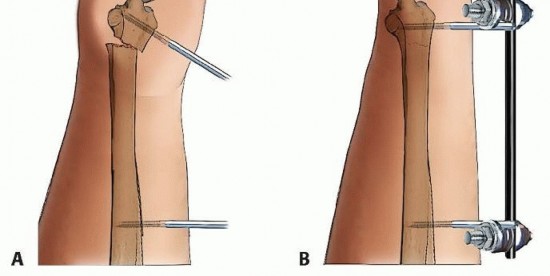
TECH FIG 6 • A. Distal pin placement. B. Final reduction with nonbridged external fixator in place. This pin should be placed parallel to the first pin in both planes, with the starting point halfway between the radiocarpal joint and the fracture.The two proximal radius pins are placed using the technique described for placement of a bridging external fixator.The incisions are closed, after which the clamps are applied but not tightened. Reduction is achieved by manipulation of the distal pins and clamps.Pushing the pins in the dorsal/volar plane corrects dorsal tilt. Adjusting the pin clamp can correct radial inclination.Reduction is confirmed using fluoroscopy, and the clamps are tightened ( TECH FIG 6B).P.260
PEARLS AND PITFALLS
Indications ▪ Determine stability1.Determine comminution and supplement fixation with external or internal fixation as necessary.Surgical approach1.Make skin incisions for pin placement to avoid sensory nerves, tendons, and crossing veins.2.Obtain adequate exposure of the radial sensory branch at forearm and hand to avoid injury.Hardware placement3.Choose pins of appropriate diameter.4.Supplement fixation with pins using external or internal fixation as necessary.5.Do not leave pins more than 1 to 2 mm out of the cortex, and keep all pins extra-articular.6.If placing the proximal metacarpal pin in metaphyseal bone, ensure that three cortices are penetrated.7.Do not back out conical pins because fixation will be lost.8.Evaluate the DRUJ after fixation to determine stability.9.Subcutaneous pins are more costly to remove because that requires a second procedure, but they have a lower infection rate. Therefore, if fixation is needed for an extended period, bury the pins.10.Overdistraction of the carpus must be avoided because it is associated with chronic pain-mediated syndromes and nonunion.Postoperative management1.Allow for adequate immobilization.2.Encourage early range of motion of the fingers, elbow, and shoulder whenever possible.3.Educate the patient regarding appropriate pin care.4.Begin strengthening only after healing is complete and range of motion is maximized.
POSTOPERATIVE CARE
After fixation with percutaneous pins, the wrist is immobilized alone in a short-arm splint to allow for swelling but provide stability. A cast is applied after the swelling goes down.Isolated radial styloid fractures fixed with pins can be placed in a volar wrist splint.External fixation devices typically require no additional immobilization, although a volar forearm-based Orthoplast (Johnson & Johnson, Langhorne, PA) splint may be used for support and patient comfort.The splint or cast is continued for 4 to 8 weeks until healing occurs and the pins are removed.K-wires and half-pins should be inspected and cleaned regularly using either soap and water or half-strength hydrogen peroxide and water.Finger, elbow, and shoulder range of motion are begun immediately, and wrist range of motion is begun as the fracture heals.
OUTCOMES
Multiple prospective randomized trials comparing volar plate fixation to closed reduction and percutaneous pinning have demonstrated quicker return to functional recovery with volar plate fixation but no difference in function at 1 year. 12,13,20,28Functional and cost comparison of extra-articular and simple intra-articular fractures treated with volar plate fixation versus closed reduction and percutaneous fixation showed only a significant cost increase with volar plate fixation and no difference in function. This study calls into question the extra cost associated with volar plate fixation. No external fixation was used to augment the percutaneous fixation which would increase the cost of this treatment method and may negate the cost benefit of percutaneousfixation. 5A prospective randomized trial comparing percutaneous pinning and casting versus external fixation with augmentation (eg, pins, screws, bone graft) found no difference in clinical outcomes for fractures with minimal articular displacement. 10In patients older than 60 years of age, percutaneous pinning has been shown to provide only marginal radiographic improvement over cast immobilization alone, with no correlation with clinical outcome. 4Ebraheim et al 6 reported excellent outcomes for restoration of radiographic parameters and functional outcomes with intrafocal pinning and trans-styloid augmentation.An evaluation of percutaneous pinning outcomes found the best results for metaphyseal fractures. Good results were found for intra-articular fractures. The worst results were seen in fractures with associatedulnar styloid fractures and fractures in elderly persons. 19A retrospective review of radiographic and clinical outcomes of open reduction internal fixation (volar and dorsal) versus external fixation revealed no significant differences, except that palmar tilt was more effectively restored with dorsal plating. 29A meta-analysis found no evidence for the use of internal fixation over external fixation for unstable distal radius fractures. 16Women older than 55 years of age with unstable intra-articular distal radius fractures treated with external fixation have a high rate of secondary displacement but can have acceptable functionaloutcomes. 11Patients older than the age of 55 years have better results with external fixation and pinning than with pinning alone. Younger patients with two or more sides having comminution also have better results with supplemental external fixation. 27Nonbridging external fixation has been shown to maintain volar tilt and carpal alignment better than bridging external fixation while having significantly better function during the first year. 17Nonbridging external fixation was shown to have no clinical advantage in patients older than 60 years ofage with moderately or severely displaced distal radius fractures. 3A prospective, randomized comparison of bridging versus nonbridging external fixation revealed more complications in the nonbridging fixators and better outcomes in the bridged fixator group. 23P.261A prospective study compared unrepaired ulnar styloid fractures to those without ulnar styloid fractures and found no significant differences in clinical outcome. However, DRUJ instability was not evaluated. 24
COMPLICATIONS
Infection (pin tract or deep). Pin tract infections occur in 10% to 30% of patients and historically have been a major problem with this treatment method. 9,10Pin tract infections can be minimized by reducing the time pins are left in place or by burying the pins beneath the skin. 15,25One study showed that pin tract infections can be reduced to a 2% incidence if they are only left in place for 30 days, then removed in the office, and the wrist then casted for another 2 weeks without the pins in place.If K-wires are going to be left in place for longer than 30 days, they should be buried under the skin at the time of surgery to help prevent pin tract infections.Injury to tendons, vessels, and nerves due to percutaneous technique. Stiffness may result if tendons are inadvertently skewered, and the radial sensory branch can be injured.Injury to the radial sensory branch can cause a painful neuroma and should be avoided. Loss of range of motionPosttraumatic arthritis Weakness in grip or pinchTenosynovitis and tendon rupture Malunion or nonunion Compartment syndromeCarpal tunnel syndrome Hardware failureNonunion (associated with overdistraction with an external fixator) Complex regional pain syndrome (CRPS) 30Vitamin C should be prescribed to prevent CRPS (500 mg once a day for 50 days)
REFERENCES
You Might Also Like