Avoid Splitting of the Radial: Master Aftercare to Prevent Wrist Complications
Key Takeaway
Looking for accurate information on Avoid Splitting of the Radial: Master Aftercare to Prevent Wrist Complications? Aftercare for a fracture, potentially involving a splitting of the radial, focuses on monitoring circulation and swelling. Key steps include completing plaster application within days, instructing on exercises, and checking the plaster at two weeks for slackening or faults. Positional errors like lack of ulnar deviation or excessive wrist flexion are corrected to prevent long-term complications and facilitate recovery.
Introduction and Epidemiology
Distal radius fractures represent one of the most frequently encountered osseous injuries in orthopedic practice, accounting for approximately one-sixth of all fractures evaluated in emergency departments. The epidemiological distribution is classically bimodal. The first peak occurs in pediatric and young adult populations, typically resulting from high-energy trauma such as motor vehicle collisions or sports-related injuries. The second, larger peak manifests in the elderly population, predominantly postmenopausal females, secondary to low-energy falls on an outstretched hand in the setting of osteopenia or osteoporosis.

The management of these fractures has evolved significantly over the past two decades, with a paradigm shift toward volar locking plate fixation for unstable patterns. However, closed reduction and cast immobilization remain the cornerstone of treatment for stable, minimally displaced, or extra-articular fractures, particularly in lower-demand patients. Regardless of the primary intervention—operative or non-operative—meticulous aftercare is paramount. Suboptimal cast application, failure to recognize positional errors, or inadequate postoperative monitoring invariably leads to profound wrist complications, including malunion, stiffness, complex regional pain syndrome, and neurovascular compromise.
Mastering the aftercare protocols requires a comprehensive understanding of wrist biomechanics, the principles of rigid immobilization, and the vigilance to identify and rectify technical faults early in the clinical course.

Surgical Anatomy and Biomechanics
A thorough comprehension of the osseous and ligamentous anatomy of the radiocarpal and distal radioulnar joints is essential for achieving anatomic reduction and avoiding iatrogenic complications during both casting and surgical fixation.
Osseous Architecture
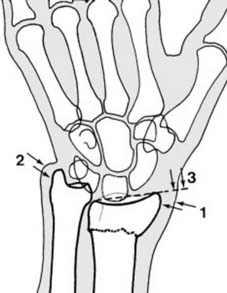
The distal radius articulates with the scaphoid and lunate at the radiocarpal joint and with the ulnar head at the distal radioulnar joint. Normal radiographic parameters are critical benchmarks for reduction:
* Radial Inclination: Averages 22 degrees (range 21 to 25 degrees).
* Volar Tilt: Averages 11 degrees (range 2 to 20 degrees).
* Radial Height: Averages 11 to 12 mm.
* Ulnar Variance: Typically neutral, though slight negative or positive variance can be physiologic.

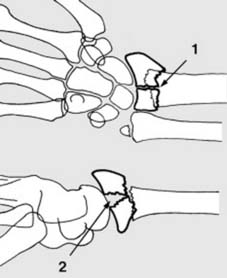
The distal radius is anatomically divided into three columns, a concept popularized by Rikli and Regazzoni. The radial column (radial styloid and scaphoid fossa) acts as an osseous buttress. The intermediate column (lunate fossa and sigmoid notch) is critical for load transmission. The ulnar column (distal ulna and triangular fibrocartilage complex) provides a stable axis for forearm rotation.
Ligamentous and Neurovascular Structures
The radiocarpal joint is stabilized by stout extrinsic volar ligaments (radioscaphocapitate, long radiolunate, short radiolunate) and thinner dorsal ligaments. The distal radioulnar joint relies heavily on the triangular fibrocartilage complex for stability.
Neurovascularly, the median nerve courses volarly between the flexor carpi radialis and the palmaris longus, making it highly susceptible to compression in the setting of excessive wrist flexion or hematoma accumulation. The superficial branch of the radial nerve exits from beneath the brachioradialis in the distal third of the forearm, placing it at risk during percutaneous pinning, external fixation, or overly tight cast application on the radial aspect of the wrist.

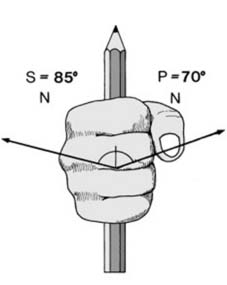
Biomechanical Load Transmission
In a neutral position, approximately 80% of the axial load across the wrist is transmitted through the distal radius, while 20% passes through the ulnar head and triangular fibrocartilage complex. Alterations in radial height or volar tilt dramatically shift these load-bearing mechanics. A loss of volar tilt to 45 degrees dorsal angulation transfers up to 65% of the load to the ulna, resulting in ulnocarpal impaction syndrome and accelerated degenerative arthrosis.
Indications and Contraindications
The decision algorithm for managing distal radius fractures hinges on fracture stability, patient physiology, and functional demands. Lafontaine criteria remain a reliable predictor of instability: initial dorsal angulation greater than 20 degrees, dorsal comminution, intra-articular extension, associated ulnar fracture, and patient age greater than 60 years. The presence of three or more criteria strongly predicts failure of conservative management.
| Modality | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Closed Reduction and Casting | Extra-articular, non-displaced fractures; Stable patterns post-reduction; Low-demand patients; High surgical risk | Open fractures; Acute carpal tunnel syndrome; Vascular compromise | Lafontaine instability criteria; Concomitant ipsilateral upper extremity fractures |
| Volar Locking Plate Fixation | Unstable extra-articular fractures; Displaced intra-articular fractures; Loss of reduction in cast; Volar shear fractures | Active local infection; Critical soft tissue compromise over the volar aspect | Severe osteopenia preventing screw purchase (consider spanning ex-fix) |
| External Fixation | Severe comminution lacking osseous landmarks; Polytrauma (damage control); Grossly contaminated open fractures | Patient inability to maintain pin site hygiene | Articular step-off requiring direct visualization (unless combined with limited internal fixation) |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning mitigates intraoperative complications and optimizes surgical efficiency. Standard posteroanterior, lateral, and oblique radiographs are mandatory. For complex intra-articular fractures, a non-contrast computed tomography scan with sagittal and coronal reformats is essential for defining articular step-offs, gap formations, and the exact location of the fracture fragments, particularly the critical lunate facet fragment.

Patient Setup
The patient is positioned supine on the operating table with the operative extremity extended on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm. The fluoroscopy unit is positioned either parallel or perpendicular to the hand table, depending on the surgeon's preference, ensuring unimpeded access for orthogonal imaging.

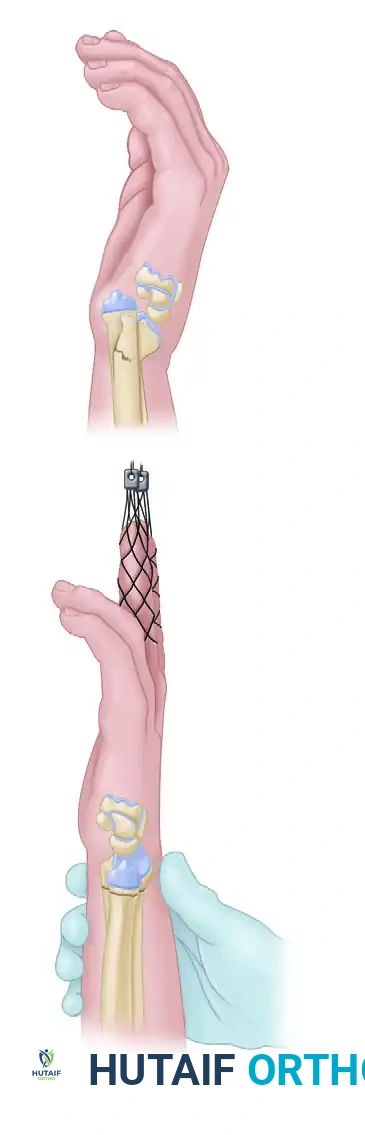
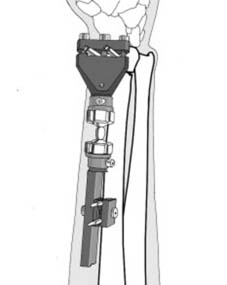
For closed reductions, adequate analgesia and muscle relaxation are critical. This is typically achieved via a hematoma block, regional anesthesia (Bier block or supraclavicular block), or procedural sedation. Finger traps and counter-traction across the upper arm with weights can be utilized to disimpact the fracture fragments and restore radial length prior to manipulation.

Detailed Surgical Approach and Technique
Whether executing a closed reduction or proceeding with open reduction and internal fixation, adherence to biomechanical principles and anatomic planes is non-negotiable.
Closed Reduction and Cast Application
The technique of closed reduction involves recreating the deformity to disimpact the fracture, followed by longitudinal traction and translation to correct the displacement. For a classic dorsally displaced Colles fracture, traction is applied, the distal fragment is translated volarly, and the wrist is brought into slight flexion and ulnar deviation.

The application of the cast or splint requires meticulous technique. A well-molded sugar-tong splint or a short arm cast utilizing three-point molding principles is standard. The plaster must be molded to support the volar aspect of the distal radius and the dorsal aspect of the distal fragment, preventing dorsal collapse. Crucially, the wrist must not be immobilized in extreme flexion. The historical Cotton-Loder position (extreme flexion and ulnar deviation) has been universally abandoned due to the unacceptably high rates of median nerve compression, extensor tendon tethering, and profound joint stiffness.

Volar Approach and Plate Fixation
For operative management, the modified Henry approach to the volar distal radius is the workhorse incision.
- Incision and Superficial Dissection: A longitudinal incision is made over the flexor carpi radialis tendon. The tendon sheath is incised, and the tendon is retracted ulnarly, protecting the median nerve. The radial artery is identified and carefully protected radially.
- Deep Dissection: The internervous plane is developed between the flexor pollicis longus and the radial artery. The pronator quadratus is identified, and an L-shaped incision is made along its radial and distal borders. The muscle is elevated subperiosteally from radial to ulnar, exposing the volar cortex of the distal radius.
- Reduction and Fixation: The fracture is debrided of hematoma. Reduction is achieved via manual traction, hyperextension, and subsequent volar flexion. A volar locking plate is applied proximal to the watershed line to avoid flexor tendon irritation. Distal locking screws are placed to support the subchondral bone of the radiocarpal joint.
- Closure: The pronator quadratus is repaired loosely over the plate if possible, though tight closure is unnecessary and may lead to ischemic contracture. The skin is closed in a standard fashion.

Complications and Management
Complications following distal radius fractures are frequent and can be devastating if not recognized and managed promptly. These stem from both the natural history of the injury and iatrogenic errors during casting or surgery. Masterful aftercare is the primary defense against these morbidities.
Cast Related Complications and Positional Errors
The aftercare of a casted distal radius fracture requires a rigorous, scheduled protocol to monitor for swelling, displacement, and technical faults in the plaster.

Day 1 Aftercare: The patient must be evaluated the day following reduction. The digits are examined for adequacy of circulation, capillary refill, and the degree of swelling. The palm, fingers, thumb, and elbow are systematically checked for constriction caused by the bandaging or elbow flexion. Any necessary adjustments, including splitting the cast or loosening outer bandages, must be made immediately to prevent compartment syndrome or ischemic contracture.

Days 2 to 5 Aftercare: At the subsequent review, digital swelling is reassessed. If the swelling is slight, the temporary splint or uncompleted plaster is finalized. If marked swelling persists, completion is delayed. Superficial layers of the cotton bandage are removed, the primary slab is retained, and encircling plaster bandages are applied. The patient is instructed in mandatory elbow and shoulder range of motion exercises. Unless significant swelling persists, the sling should be discarded to encourage functional use of the limb and prevent proximal stiffness.

Two Week Aftercare: At the two-week mark, the plaster is evaluated for marked slackening (requiring replacement) or softening (requiring reinforcement). Movements in the fingers, elbow, and shoulder are critically examined. Radiographs are obtained to assess maintenance of reduction. While slight slipping is often inevitable in non-operative management, marked slipping may indicate the need for remanipulation or conversion to operative fixation. At this stage, the plaster may be safely transitioned to a lighter resin or fiberglass cast.
Positional Errors:
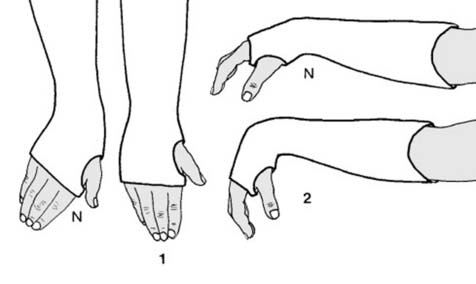
1. Lack of Ulnar Deviation: The most common positional fault is the failure to maintain ulnar deviation. If discovered within the first two weeks, the wrist should be replastered in the correct position. If discovered later, it is often sadly accepted, but the surgeon must anticipate late problems. Lack of ulnar deviation increases the risk of distal radioulnar joint disruption, non-union of the ulnar styloid, restriction of pronosupination, and chronic ulnar-sided wrist pain.
2. Excessive Wrist Flexion: As previously noted, the Cotton-Loder position is obsolete. Excessive flexion leads to profound difficulty in recovering dorsiflexion and a functional grip. More importantly, it is highly associated with acute compression of the median nerve. If excessive flexion is present, the plaster must be immediately removed and re-applied with the wrist in a more neutral, extended position.
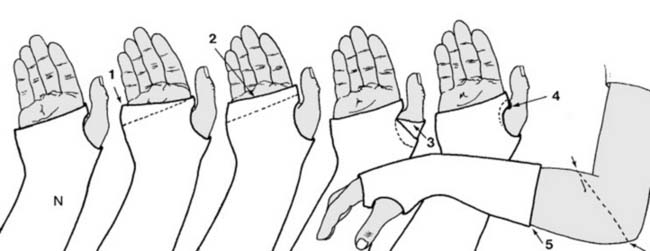
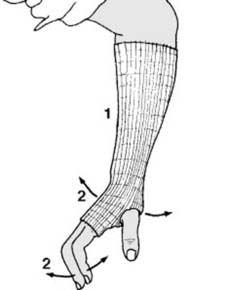
Plaster Faults: Errors in plastering technique restrict motion and cause skin breakdown. Common faults discovered during aftercare include:
1. The distal edge of the plaster failing to follow the normal oblique line of the metacarpophalangeal joints, restricting the little and ring fingers. The plaster must be trimmed to allow full 90-degree flexion of all metacarpophalangeal joints.
2. Plaster extending beyond the distal palmar crease, restricting all metacarpophalangeal joints.
3. The thumb being restricted by errant turns of the plaster bandage. The plaster should be trimmed proximal to the interphalangeal joint to permit free movement.
4. The plaster digging into the delicate skin of the first web space, which requires immediate trimming to prevent ulceration.
5. A plaster that is too short, failing to provide adequate biomechanical support to the fracture site.
Surgical Complications
Operative management, while providing superior biomechanical stability, introduces its own spectrum of complications.
| Complication | Incidence | Etiology and Risk Factors | Management and Salvage Strategy |
|---|---|---|---|
| Tendon Rupture (EPL or Flexors) | 1-5% | Prominent dorsal screws (EPL); Plate placed distal to watershed line (FPL/FDP) | Hardware removal; Tendon transfer (EIP to EPL) or tendon grafting |
| Median Neuropathy | 5-15% | Fracture hematoma; Excessive traction; Poor positioning; Iatrogenic injury | Immediate cast splitting if closed; Carpal tunnel release if progressive or unresponsive |
| Complex Regional Pain Syndrome | 5-10% | Tight casts; Poor pain control; Failure to mobilize digits early | Aggressive hand therapy; Gabapentinoids; Stellate ganglion blocks |
| Intra-articular Hardware Penetration | 2-8% | Unrecognized screw penetration during fluoroscopy (loss of dorsal tilt) | Immediate hardware removal/exchange; Utilization of skyline views intraoperatively |
| Loss of Reduction / Malunion | 5-20% | Inadequate fixation; Severe osteopenia; Premature weight-bearing | Corrective osteotomy with structural bone grafting and rigid internal fixation |

Post Operative Rehabilitation Protocols
The ultimate functional outcome of a distal radius fracture is heavily dependent on the quality of the rehabilitation protocol. The primary goal is to restore pain-free motion and grip strength while protecting the healing osseous structures.
Phase One Early Immobilization
During the first 10 to 14 days, the focus is on edema control and proximal/distal joint mobility. Whether the patient is in a cast or a postoperative splint, active range of motion of the fingers (full composite flexion and extension), thumb, elbow, and shoulder is mandatory. Edema is managed with strict elevation and digital compressive wrapping if necessary.

Phase Two Intermediate Mobilization
At two to six weeks, patients managed with volar locking plates are typically transitioned to a removable thermoplastic splint. Active and active-assisted range of motion of the wrist (flexion, extension, pronation, supination) is initiated. Passive stretching is generally avoided during this phase to prevent hardware failure or loss of reduction. Scar massage and desensitization techniques are introduced to manage the surgical incision and prevent adhesions. For patients managed non-operatively, cast immobilization continues, but digital motion remains a critical daily requirement.

Phase Three Strengthening and Load Bearing
Beyond six weeks, assuming clinical and radiographic evidence of union, the splint is progressively weaned. Strengthening exercises utilizing putty, hand grippers, and light weights are incorporated. Proprioceptive training and weight-bearing through the upper extremity are advanced. Full return to heavy manual labor or contact sports is typically delayed until 10 to 12 weeks post-injury, contingent upon the restoration of grip strength to at least 80% of the contralateral limb.
Summary of Key Literature and Guidelines
The management of distal radius fractures is guided by robust clinical evidence and consensus guidelines. The American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines provide evidence-based recommendations emphasizing the importance of rigid immobilization and the selective use of operative fixation for unstable patterns.

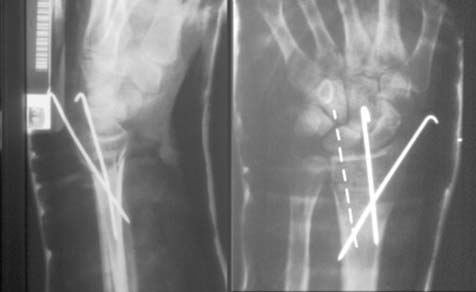
Key literature, including the DRAFFT (Distal Radius Acute Fracture Fixation Trial), has challenged the absolute superiority of volar locking plates over percutaneous K-wire fixation in specific demographics, highlighting that functional outcomes at 12 months may be comparable in older populations. Furthermore, studies by Arora et al. have demonstrated that while radiographic restoration is superior with volar plating in the elderly, this does not consistently translate to superior functional outcomes compared to non-operative management, provided that catastrophic positional errors and cast complications are avoided.
Ultimately, the mastery of distal radius fracture management lies not solely in surgical prowess, but in the meticulous execution of aftercare. By vigilantly monitoring for positional errors, avoiding plaster faults, and instituting early, aggressive rehabilitation, the orthopedic surgeon can predictably prevent devastating wrist complications and ensure optimal functional recovery.
You Might Also Like