Management of Clavicular Malunions: Corrective Osteotomy and Fixation
Key Takeaway
Symptomatic clavicular malunions present with pain, weakness, and scapular dyskinesia due to altered shoulder girdle biomechanics. Shortening greater than 20 millimeters significantly impacts glenohumeral mobility. Corrective osteotomy with rigid plate fixation and optional intercalary bone grafting restores anatomical length and alignment. This comprehensive guide details the indications, surgical approaches, biomechanical considerations, and postoperative rehabilitation protocols for managing complex midshaft and lateral clavicle malunions.
Introduction to Clavicular Malunions
Historically, the vast majority of clavicle fractures were treated nonoperatively, with the prevailing dogma suggesting that clavicular malunions are well-tolerated and cause no significant functional limitations. However, contemporary orthopedic literature and advanced biomechanical analyses have catalyzed a paradigm shift. While many patients do achieve asymptomatic union despite some degree of deformity, a distinct subset of patients develops debilitating symptoms secondary to altered shoulder girdle mechanics.
Malunion of the clavicle can result in profound functional deficits, chronic pain, and neurovascular compromise. The malunions that typically prove most disabling involve the medial or lateral thirds of the bone, though severe midshaft deformities are increasingly recognized as sources of significant morbidity. Symptoms of a symptomatic malunion include rapid fatigability, thoracic outlet syndrome (TOS), difficulty wearing over-the-shoulder straps, subjective weakness, chronic pain, and the cosmetic deformity of a droopy, "driven-in," or ptotic shoulder.
Biomechanics and Pathoanatomy
The clavicle functions as the sole osseous strut connecting the axial skeleton to the upper extremity. It acts akin to a crane jib, suspending the scapula and maintaining the optimal resting length of the shoulder girdle musculature.
The Impact of Shortening and Angulation
When a clavicle fracture heals with significant shortening or angular deformity, the spatial orientation of the glenoid fossa is fundamentally altered.
* Scapular Kinematics: Shortening causes the scapula to protract, internally rotate, and tilt anteriorly. This resting malposition (scapular dyskinesia) forces the rotator cuff to operate at a mechanical disadvantage.
* Glenohumeral Mobility: Altered glenoid version directly impacts glenohumeral mobility and scapular rotation, leading to impingement syndromes and rapid fatigability of the periscapular musculature.
* Clinical Thresholds: Eskola et al., in a landmark study of 89 patients, demonstrated that clavicular shortening of 15 mm or more caused significant discomfort and dysfunction of the shoulder girdle. Similarly, Hill et al. found that 20 mm of shortening following closed treatment of displaced middle-third fractures was highly correlated with poor clinical outcomes.
Clinical Pearl: While Oroko et al. and Nordqvist et al. did not find a strict linear correlation between shortening and poor results in all cohorts, the modern consensus dictates that shortening greater than 2 cm in an active patient is a major risk factor for symptomatic malunion.
Thoracic Outlet Syndrome (TOS)
Inferior angulation and hypertrophic callus formation can encroach upon the costoclavicular space. This osseous prominence can compress the brachial plexus (particularly the medial cord) and the subclavian vessels, resulting in secondary thoracic outlet syndrome. In some patients, simply excising the offending bony prominence relieves the neurological symptoms, a technique successfully reported by Fujita et al. and Rowe. However, in the presence of global shoulder dysfunction, a formal corrective osteotomy is preferred.
Clinical Evaluation
Patient History
Patients actively seeking treatment for clavicular malunions typically present at least 1 year post-injury. The history is characterized by persistent complaints unresponsive to conservative management (physical therapy, NSAIDs, activity modification). Key historical features include:
* Chronic, aching pain exacerbated by overhead activities.
* Neurological complaints (paresthesias, numbness) radiating down the arm, indicative of TOS.
* Inability to carry heavy backpacks or wear bra straps due to localized pressure over the fracture apex.
* Dissatisfaction with the cosmetic appearance of the shoulder.
Physical Examination
- Inspection: Note the classic "ptotic" or "driven-in" shoulder. Assess for hypertrophic scarring or prominent hardware if previously treated.
- Palpation: Identify the apex of the deformity. Point tenderness is common.
- Range of Motion: Assess for scapular winging and dyskinesia during active forward elevation and abduction.
- Neurovascular Exam: Perform provocative tests for thoracic outlet syndrome (Adson's test, Wright's test, Roos test). Document baseline sensory and motor function of the upper extremity.
Radiographic Imaging
- Standard Radiographs: Bilateral anteroposterior (AP) and 15-degree cephalic/caudal tilt views. Bilateral imaging is crucial to accurately measure the degree of shortening compared to the contralateral, uninjured clavicle.
- Computed Tomography (CT): A CT scan with 3D reconstructions is the gold standard for preoperative planning. It precisely quantifies angular deformity, translation, and shortening, and helps delineate the plane of the malunion for the planned osteotomy.
Indications and Contraindications for Surgery
Several investigators, including McKee, Wild, and Schemitsch, have demonstrated excellent outcomes following osteotomy and plate fixation for symptomatic clavicular malunions.
Radiographic Criteria for Osteotomy
The authors’ current radiographic criteria for osteotomy and plating include:
* Substantial shortening: Greater than 1 cm (usually 2 to 3 cm).
* Angular deformity: Greater than 30 degrees.
* Translation: Greater than 1 cm.
Clinical Indications
- Chronic pain and weakness refractory to conservative management for at least 1 year.
- Thoracic outlet syndrome secondary to osseous compression.
- Rotator cuff impingement secondary to altered scapular mechanics (as reported by Naert, Chipochase, and Krishnan).
- Note: Surgery is rarely, if ever, indicated for cosmesis alone, though cosmetic satisfaction is a frequent secondary benefit.
Contraindications
- Inadequate soft-tissue coverage.
- Active infection.
- Asymptomatic malunion (regardless of radiographic appearance).
- Noncompliant patient.
- Severely osteopenic or pathological bone.
Surgical Technique: Midshaft Malunion Osteotomy
The goal of surgery is to restore the anatomical length, alignment, and rotation of the clavicle, thereby restoring the resting position of the shoulder girdle.
1. Patient Positioning and Preparation
- Place the patient in the beach-chair position with the head secured.
- Place a small bump between the scapulae to allow the shoulder girdle to fall posteriorly, aiding in the restoration of clavicular length.
- Prep and drape the entire forequarter, allowing free manipulation of the arm. If an intercalary bone graft is anticipated, prep the ipsilateral iliac crest.
2. Surgical Approach
- Make a transverse or slightly oblique incision centered over the palpable deformity.
- Carefully dissect through the subcutaneous tissue and platysma.
Surgical Warning: The supraclavicular nerves traverse this field. Meticulous dissection and preservation of these branches are critical to prevent painful postoperative neuromas and anterior chest wall numbness.
3. Exposure and Protection of Neurovascular Structures
- Elevate the clavipectoral fascia and periosteum minimally to preserve the blood supply, but sufficiently to visualize the malunion.
- CRITICAL STEP: Place a malleable retractor or a blunt Hohmann retractor inferior to the clavicle to protect the subclavian vein, subclavian artery, and brachial plexus during the osteotomy and drilling.
4. The Osteotomy
- Based on preoperative CT templating, identify the original fracture plane.
- Use a fine oscillating saw to perform the osteotomy. Depending on the morphology, an oblique osteotomy along the original fracture line or a transverse osteotomy may be required.
- If a prominent posterior or inferior bony spike is compressing the brachial plexus, resect it meticulously.
5. Restoration of Length and Bone Grafting
- Apply a laminar spreader or a specialized distraction tool to restore the anatomical length of the clavicle.
- To Graft or Not to Graft: McKee et al. reported success in 15 patients without the use of intercalary bone grafts, achieving an average preoperative shortening correction of 2.9 cm. However, other authors (Chan et al., Bosch et al.) strongly recommend interposition structural bone grafting (e.g., tricortical iliac crest) when lengthening exceeds 1.5 to 2 cm.
- Rationale for Grafting: Extensive acute lengthening without a graft can leave a massive cortical defect and place undue tension on the brachial plexus. If associated nonunion is present, autologous cancellous bone grafting is mandatory.
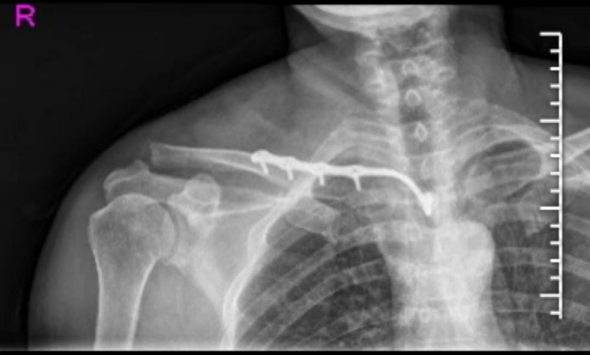
6. Plate Fixation
- Apply a pre-contoured, anatomically designed clavicle locking plate.
- Superior vs. Anteroinferior Placement: Superior plating offers excellent biomechanical stability on the tension band side but carries a higher risk of hardware prominence. Anteroinferior plating utilizes longer screws in the AP plane and reduces hardware irritation, though it requires careful trajectory to avoid neurovascular injury.
- Ensure at least three (preferably four) bicortical locking screws are placed in both the medial and lateral fragments.
- Achieve absolute stability. If an intercalary graft is used, it should be compressed and incorporated into the fixation construct.
Pitfall: Failure to achieve rigid fixation in a corrective osteotomy will inevitably lead to hardware failure and nonunion. Utilize lag screws through the plate or independently if the osteotomy geometry allows.
Management of Lateral Third Malunions
Malunions of the lateral third of the clavicle present a unique biomechanical challenge, as they frequently involve disruption of the coracoclavicular (CC) ligament complex.
* If the lateral malunion is symptomatic, simple osteotomy and plating may be insufficient if the CC ligaments remain incompetent.
* In these scenarios, a procedure analogous to that described for chronic acromioclavicular (AC) joint dislocations is indicated.
* This involves corrective osteotomy, rigid plate fixation (often utilizing a lateral clavicle plate with multiple small distal screws), and concurrent CC ligament reconstruction using a free tendon allograft or a suspensory cortical button device to restore the superior-inferior stability of the lateral clavicle.
Postoperative Rehabilitation Protocol
Successful outcomes depend heavily on a structured, phased rehabilitation program to prevent hardware failure while promoting osseous union and restoring shoulder kinematics.
Phase I: Immediate Postoperative (Weeks 0-2)
- Immobilization: The patient is placed in a standard shoulder sling.
- Motion: Pendulum exercises are initiated immediately postoperatively to prevent glenohumeral adhesive capsulitis.
- Restrictions: Strict non-weight bearing of the operative extremity. No active elevation or abduction.
Phase II: Early Motion (Weeks 2-4)
- Motion: Active-assisted range of motion (AAROM) is initiated at 2 weeks. This includes supine wand exercises and pulley systems, limiting elevation to 90 degrees.
- Wound Care: Suture removal at 14 days. Monitor for signs of superficial infection.
Phase III: Active Motion (Weeks 4-6)
- Radiographic Check: At 4 weeks, AP and tilt radiographs are obtained. If radiographs demonstrate maintenance of reduction and early callus formation with no hardware failure, the protocol advances.
- Motion: Full active and passive range of motion is initiated.
- Weaning: The patient is progressively weaned from the sling for activities of daily living.
Phase IV: Strengthening (Weeks 6-8 and Beyond)
- Radiographic Check: Resisted and strengthening activities are strictly withheld until radiographs reveal definitive osseous union, typically observed between 6 to 8 weeks.
- Strengthening: Once union is confirmed, initiate progressive resistance exercises focusing on the rotator cuff and periscapular stabilizers (rhomboids, trapezius, serratus anterior) to correct the chronic scapular dyskinesia that accompanied the malunion.
- Return to Sport/Heavy Labor: Usually permitted at 3 to 4 months postoperatively, contingent upon full restoration of strength and radiographic consolidation.
Outcomes and Complications
Clinical Outcomes
The literature demonstrates high satisfaction rates following corrective osteotomy. In the series by McKee et al., functional scores improved in all 15 patients. Of 12 patients with preoperative pain and weakness, symptoms resolved completely in eight and improved in four. Neurological complaints resolved or improved in 10 of 11 patients. Furthermore, 12 of 13 patients who found their preoperative cosmetic appearance unacceptable were satisfied postoperatively. Bosch et al. and Chan et al. similarly reported excellent functional and cosmetic restoration following osteotomy and grafting.
Potential Complications
- Nonunion: The most significant complication. In McKee's series, there was one loss of fixation resulting in nonunion. Rigid fixation and meticulous soft-tissue handling are paramount.
- Hardware Prominence: Due to the subcutaneous nature of the clavicle, plates frequently become symptomatic once the bone has healed. Elective hardware removal is common (two plates were removed electively in the McKee series) but should be delayed until at least 12-18 months postoperatively.
- Neurovascular Injury: Iatrogenic injury to the subclavian vessels or brachial plexus is a catastrophic risk during osteotomy and drilling.
- Infection and Wound Breakdown: Rare, but requires aggressive debridement and targeted antibiotic therapy if it occurs.
- Hypertrophic Scarring: Patients should be counseled preoperatively regarding the cosmetic appearance of the surgical incision, as the anterior chest wall is prone to keloid and hypertrophic scar formation.
You Might Also Like