Heal Your Clavicle Fractures: Expert Guide & Recovery Tips
Key Takeaway
For anyone wondering about Heal Your Clavicle Fractures: Expert Guide & Recovery Tips, Clavicle fractures clavicle account for 2.6% of all fractures and up to 66% of shoulder fractures. Eighty percent occur in the middle third, a vulnerable S-shaped section lacking muscle reinforcement. The primary mechanism of injury is typically a fall onto the affected shoulder, leading to a bending force on the clavicle.
Introduction and Epidemiology
Clavicle fractures represent a prevalent orthopedic injury, frequently encountered in diverse patient populations. As a crucial component of the shoulder girdle, the clavicle serves to transmit forces from the upper extremity to the axial skeleton and maintain scapular position relative to the thorax, facilitating optimal glenohumeral joint function. Fractures of the clavicle account for approximately 2.6% of all skeletal fractures across the body and a substantial 44% to 66% of all fractures occurring about the shoulder girdle. This high incidence underscores their clinical significance, necessitating a thorough understanding of their epidemiology, biomechanics, and management.
The demographic distribution of clavicle fractures is bimodal, with peaks observed in young, active males (typically under 30 years of age) due to high-energy trauma sustained during sports activities or motor vehicle collisions, and in older females, often associated with low-energy falls secondary to osteopenia or osteoporosis. Pediatric clavicle fractures, particularly at birth, also represent a distinct entity.
A critical epidemiological distinction lies in the anatomical location of the fracture. Middle third clavicle fractures constitute the vast majority, accounting for approximately 80% of all clavicle fractures. These fractures typically occur at the junction of the lateral convex and medial concave curves, a region known for its relative structural weakness. In contrast, fractures of the lateral third of the clavicle comprise about 15% of cases, often involving the distal clavicle and its articulations with the acromion and coracoclavicular ligaments. Fractures of the medial third of the clavicle are the least common, representing only about 5% of all clavicle fractures, and frequently pose unique diagnostic and therapeutic challenges due to their proximity to vital mediastinal structures and the complex biomechanics of the sternoclavicular joint. Understanding these epidemiological trends is fundamental for guiding clinical assessment and treatment strategies.
Surgical Anatomy and Biomechanics
The clavicle, a slender S-shaped long bone, is unique in its developmental and functional characteristics within the human skeleton. It is the first bone in the body to undergo ossification, beginning intramembranously during the fifth week of gestation. Conversely, it is the last ossification center to fuse, with the medial epiphysis at the sternal end typically uniting with the diaphysis between 22 and 25 years of age. This protracted ossification process can sometimes lead to confusion with medial clavicle fractures in younger adults.
Clavicular Morphology and Ligamentous Attachments
The S-shape of the clavicle is characterized by a medial end that is convex anteriorly and a lateral end that is concave anteriorly. This morphology allows for crucial biomechanical functions and influences fracture patterns. The clavicle is widest and most robust at its medial end, tapering and thinning laterally before expanding slightly at its flattened acromial end. The medial and lateral ends feature flat expansions, while the middle shaft is more tubular, often exhibiting sparse medullary bone, which contributes to its vulnerability to fracture.
The primary function of the clavicle is to serve as a rigid strut, bracing the shoulder posterolaterally from the trunk. This strut function is essential for maintaining the scapula in its optimal position, allowing for a wide range of motion and enabling the deltoid muscle to function at optimal length and strength. Without this strut, the shoulder girdle would collapse anteromedially.
Several crucial muscle groups attach to the clavicle, influencing fracture displacement and stability. The sternocleidomastoid muscle originates from the medial third, tending to elevate the medial fragment. The pectoralis major muscle attaches to the anterior aspect of the medial two-thirds, and the deltoid muscle originates from the lateral two-thirds, contributing to inferoposterior displacement of distal fragments. The trapezius muscle attaches to the posterior aspect of the lateral third, assisting in scapular elevation and retraction. Inferiorly, the subclavius muscle inserts into the subclavian groove on the undersurface of the middle third. Distal to the subclavius insertion, the middle third lacks substantial reinforcement by muscles or ligaments, rendering it additionally vulnerable to fracture.

Neurovascular Proximity
The medial one-third of the clavicle and its inferior aspect are in close proximity to several vital structures, including the brachial plexus, the subclavian artery and vein, the axillary vessels, and the superior dome of the lung (pleural apex). Fractures in this region, particularly those with significant displacement, carry a higher risk of neurovascular injury or pneumothorax/hemothorax. The sternoclavicular joint capsule, reinforced by anterior and posterior sternoclavicular ligaments, and the interclavicular ligament provide significant stability to the medial end.
Ligamentous Stability of the Lateral Clavicle
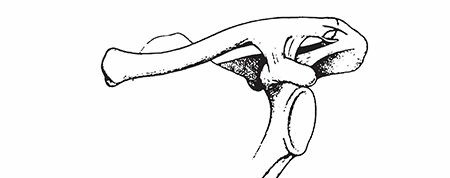
The distal clavicle is characterized by its articulation with the acromion at the acromioclavicular (AC) joint and its strong ligamentous connections to the coracoid process. The coracoclavicular (CC) ligaments are paramount for the vertical stability of the AC joint and the entire shoulder girdle. These ligaments consist of two distinct components:
1. Trapezoid ligament: Located anterolaterally, it is a quadrilateral sheet running from the superior aspect of the coracoid process to the trapezoid line on the conoid tubercle of the clavicle.
2. Conoid ligament: Situated posteromedially, it is a stronger, conical ligament extending from the base of the coracoid process to the conoid tubercle on the clavicle.
These CC ligaments are significantly stronger than the intrinsic AC ligaments and provide the primary restraint against superior clavicular migration relative to the acromion. Fractures of the lateral clavicle that disrupt these ligaments often result in superior displacement of the medial fragment, necessitating operative stabilization to restore proper shoulder biomechanics.
Biomechanical Vulnerability
The junction between the medial convex forward and lateral concave forward cross-sectional configurations, located in the middle third of the clavicle, represents a distinct biomechanical weak point. This area is particularly vulnerable to fracture, especially with axial loading or direct bending forces. The sparse medullary bone in this segment further contributes to its susceptibility. The mechanism of injury for most clavicular fractures, accounting for approximately 87%, involves falls onto the affected shoulder, leading to a bending force that exploits this biomechanical weakness. Direct impact accounts for only 7% of fractures, while falls onto an outstretched hand (FOOSH) account for 6%. Rarely, clavicle fractures can occur secondary to violent muscle contractions, such as during seizures or severe trauma.

Indications and Contraindications
The decision-making process for managing clavicle fractures involves a careful consideration of fracture characteristics, patient factors, and potential risks and benefits of operative versus non-operative treatment. While historically most clavicle fractures were managed non-operatively, a growing body of evidence supports operative intervention for specific fracture patterns, particularly those with significant displacement or shortening.
Non-Operative Management Indications
Non-operative management typically involves a period of immobilization, often with a sling, followed by a structured rehabilitation program. It is generally indicated for:
* Minimally displaced or non-displaced fractures: Fractures with less than 100% displacement or less than 2 cm of shortening.
* Stable fracture patterns: Particularly in the middle third, where bony contact is maintained or early callus formation is expected.
* Nondisplaced lateral clavicle fractures: Those with intact coracoclavicular ligaments (Neer Type I).
* Medial clavicle fractures: Due to the rarity and proximity to vital structures, most medial clavicle fractures are managed non-operatively unless there is significant displacement with impending neurovascular compromise or sternoclavicular joint instability.
* Pediatric fractures: Children generally have a robust healing potential and a higher tolerance for malunion, making non-operative treatment the standard for most pediatric clavicle fractures.
* Patients with significant comorbidities: Those for whom the risks of surgery outweigh the potential benefits (e.g., severe cardiopulmonary disease, uncontrolled diabetes, active infection).
* Patient preference: After thorough discussion of risks and benefits of both treatment modalities.
Operative Management Indications
Operative fixation aims to restore anatomical alignment, provide stable internal fixation, and facilitate early rehabilitation to optimize functional outcomes and minimize the risk of nonunion or symptomatic malunion. Indications for operative intervention include:
- Significant displacement: Generally defined as >100% displacement (no cortical contact) or >2 cm of shortening in adults, particularly for middle third fractures.
- Severe comminution: Multifragmentary fractures that are inherently unstable.
- Open fractures: Requiring debridement and stabilization to prevent infection and facilitate healing.
- Neurovascular compromise: Fractures associated with injury to the brachial plexus or subclavian vessels, necessitating emergent reduction and stabilization.
- Skin compromise: Fractures with impending skin perforation (tenting), especially in thin patients.
- Polytrauma patients: Where early mobilization is critical, and a stable clavicle can aid overall recovery.
- Symptomatic nonunion or malunion: Persistent pain, functional limitations, or neurovascular symptoms from a previously treated fracture.
- Specific lateral clavicle fracture patterns:
- Neer Type II: Fractures distal to the conoid and trapezoid ligaments, leading to instability of the medial fragment due to trapezius pull.
- Neer Type V: Comminuted distal fractures, often with displacement.
- Medial clavicle fractures: Rare indications include persistent sternoclavicular joint dislocation/subluxation, mediastinal compression symptoms, or significant displacement causing neurovascular compromise or tracheal impingement.
- Floating shoulder: Ipsilateral scapular neck and clavicle fractures with significant displacement.
Contraindications
Absolute contraindications to surgery for clavicle fractures are rare and typically relate to the patient's overall medical condition, rather than the fracture itself.
* Absolute Contraindications:
* Active local or systemic infection.
* Significant medical comorbidities precluding safe anesthesia and surgery.
* Severe, non-correctable coagulopathy.
* Relative Contraindications:
* Poor soft tissue envelope or severe contamination.
* Extensive local skin disease.
* Poor patient compliance with postoperative protocols.
* Active smoking (increases risk of nonunion and infection).
| Feature | Non-Operative Indications | Operative Indications |
|---|---|---|
| Displacement | Minimally displaced (<100%) or non-displaced | >100% displaced (no cortical contact), >2 cm shortening |
| Comminution | Simple, stable patterns | Severe, multifragmentary, unstable comminution |
| Integrity | Closed fractures, intact skin | Open fractures, impending skin tenting |
| Neurovascular | Intact neurovascular status | Associated neurovascular compromise |
| Associated Inj. | Isolated injury or stable associated injuries | Polytrauma, floating shoulder |
| Location | Most pediatric fractures, stable medial third, Neer Type I lateral | Displaced middle third, Neer Type II/V lateral, symptomatic medial |
| Prior Treatment | Acute fracture, no prior nonunion/malunion | Symptomatic nonunion or malunion |
| Patient Factors | Significant comorbidities, patient preference for non-op | Healthy, active patient desiring early return to function |
Preoperative Planning and Patient Positioning
Thorough preoperative planning is critical for optimizing surgical outcomes and minimizing complications in clavicle fracture fixation. This phase encompasses comprehensive patient evaluation, detailed imaging assessment, strategic implant selection, and meticulous operative setup.
Patient Evaluation and Assessment
A comprehensive medical history should be obtained, focusing on the mechanism of injury, associated symptoms (e.g., paresthesias, weakness, chest pain, dyspnea), hand dominance, and pre-existing medical conditions, particularly those affecting bone healing (e.g., diabetes, smoking, corticosteroid use, nutritional deficiencies). A meticulous physical examination is essential. This includes:
* Inspection: Assessment for skin tenting, open wounds, ecchymosis, and deformity.
* Palpation: Tenderness, crepitus, and assessment of fracture fragment mobility.
* Neurovascular Assessment: Meticulous evaluation of the brachial plexus and subclavian/axillary vessels. Assessment of pulses, capillary refill, sensation, and motor function distal to the injury. Any deficits warrant immediate investigation.
* Associated Injuries: Evaluation for injuries to the cervical spine, scapula, ribs, lung, and ipsilateral upper extremity.
Imaging Studies
Standard imaging typically includes:
* Anteroposterior (AP) Clavicle View: Demonstrates overall alignment and displacement.
* 45-degree Cephalic Tilt View (Serendipity View): Particularly useful for visualizing middle and medial third fractures, helping to delineate superior-inferior displacement and shortening.
* Axial View (or Clavicle Outlet View): Can help assess sagittal plane displacement.
For complex fractures, particularly those involving the medial or lateral third, or suspected associated injuries, further imaging may be warranted:
* Computed Tomography (CT) Scan: Indispensable for detailed assessment of comminution, articular involvement (AC or SC joints), true shortening, and relationship to vital structures, especially for medial third fractures. A CT angiogram may be necessary if vascular injury is suspected.
* Magnetic Resonance Imaging (MRI): Rarely used for acute clavicle fractures, but may be beneficial in assessing associated ligamentous injuries (e.g., coracoclavicular ligaments in distal clavicle fractures) or soft tissue injuries, or in evaluating for nonunion.
Preoperative Templating and Implant Selection
Based on imaging, surgeons should template plate length, contour, and screw placement. Key considerations include:
* Plate type: Locking compression plates (LCPs) are widely used due to their angular stable fixation, particularly in osteoporotic bone or comminuted fractures. Reconstruction plates may be an option for highly contoured areas or specific fracture patterns. Pre-contoured plates are designed to match the S-shape of the clavicle, reducing intraoperative bending.
* Plate position: Superior plating often provides better biomechanical stability but carries a higher risk of hardware prominence and irritation to the supraclavicular nerves. Anterosuperior or anterior plating may be used to mitigate these risks.
* Screw types: Cortical screws are used in conjunction with non-locking plates, while locking screws provide angular stability with LCPs. Bicortical screw purchase is generally preferred.
* Potential need for bone graft: Autologous (iliac crest) or allograft may be considered for highly comminuted fractures with bone loss, or in revision cases for nonunion.
Anesthesia and Patient Positioning
- Anesthesia: General anesthesia is typically employed. Regional nerve blocks (e.g., interscalene block) can be considered as an adjunct for postoperative pain control, but care must be taken to avoid obscuring neurovascular monitoring during dissection.
- Patient Positioning:
- Beach Chair Position: This is a common and versatile position, allowing excellent access to the entire clavicle, scapula, and glenohumeral joint if needed. The patient is semi-sitting with the back of the bed elevated, and the head supported in a headrest. The affected arm is draped free to allow for intraoperative manipulation.
- Supine Position with a Shoulder Roll: This position is also frequently used. A padded rolled towel or sandbag is placed longitudinally between the scapulae, allowing the shoulders to fall posteriorly and facilitating exposure of the clavicle. The affected arm is draped free.
Regardless of the chosen position, appropriate padding of pressure points is crucial. The surgical field should be prepped and draped to allow for wide exposure from the sternum to the acromion and superiorly to the neck base. Fluoroscopy equipment should be positioned to allow for AP and cephalic tilt views without interfering with the surgical field.

Detailed Surgical Approach and Technique
Operative fixation of clavicle fractures aims to restore anatomical alignment, provide stable fixation, and facilitate early functional recovery. The specific approach and technique depend on the fracture location, pattern, and surgeon preference.
General Principles
- Aseptic Technique: Strict adherence to sterile principles is paramount to prevent surgical site infection.
- Adequate Exposure: An incision that provides sufficient visualization of the fracture site and surrounding anatomy, while minimizing soft tissue stripping.
- Neurovascular Protection: Meticulous dissection to identify and protect vital structures, particularly the supraclavicular nerves, brachial plexus, and subclavian vessels.
- Gentle Tissue Handling: Minimize retraction and blunt dissection to preserve periosteal blood supply.
- Anatomic Reduction: Restoration of length, alignment, and rotation of the clavicle fragments.
- Stable Fixation: Use of appropriate hardware to withstand physiological loads during the healing process.
Surgical Approach and Incision
The most common approach for middle and lateral third clavicle fractures is an anterosuperior skin incision. This incision follows the natural skin creases (Langer's lines) just inferior to the palpable subcutaneous border of the clavicle, or directly over it. The length of the incision is dictated by the fracture pattern and required exposure. For highly comminuted or long oblique fractures, a longer incision may be necessary to facilitate reduction and plating.
Dissection and Internervous Planes
- Skin Incision: Make the incision down to the subcutaneous fat.
- Subcutaneous Dissection: Carefully dissect through the subcutaneous tissue. Identify and protect the supraclavicular nerves, which cross the operative field perpendicularly to the clavicle. These sensory nerves are superficial and prone to injury, leading to numbness or dysesthesias. Gentle retraction or careful dissection and preservation are crucial.
- Platysma: If the incision extends medially, the platysma muscle may be encountered. This muscle should be sharply divided in line with the skin incision and carefully repaired at closure to minimize scar hypertrophy.
- Deep Fascia: Incise the deep fascia overlying the clavicle.
- Subperiosteal vs. Extraperiosteal Dissection:
- Subperiosteal dissection: Involves incising the periosteum longitudinally along the superior aspect of the clavicle and carefully elevating it. This provides a clear view of the bone and limits soft tissue disruption. However, it can devascularize fracture fragments, potentially impeding healing.
- Extraperiosteal (submuscular) dissection: Involves elevating the deltoid or pectoralis major origin off the superior aspect of the clavicle while preserving the periosteum where possible. This is often preferred, particularly for locking plate fixation, to maximize biological healing potential. The periosteum is then carefully incised only as needed for plate application.
- Protection of Inferior Structures: Throughout the dissection, particularly when drilling or passing instruments, care must be taken to protect the neurovascular structures inferior to the clavicle. A malleable retractor or a blunt elevator can be placed along the inferior aspect of the clavicle to shield these structures.
Fracture Reduction
Reduction of clavicle fractures aims to restore anatomical length, alignment, and rotation.
* Indirect Reduction: For less displaced fractures, gentle traction on the arm, sometimes combined with manipulation of the shoulder girdle, may achieve acceptable alignment.
* Direct Reduction: For significantly displaced or comminuted fractures, direct manipulation of fragments is often required.
* Fragment clamps: Pointed reduction clamps or bone-holding forceps are invaluable for grasping and reducing fragments.
* Joysticks: K-wires can be inserted into the main fragments to serve as joysticks, allowing for controlled manipulation.
* Periosteal elevators: Can be used to lever fragments into position.
* Addressing shortening: Requires sustained traction, sometimes assisted by an assistant pulling on the ipsilateral arm.
* Restoring rotation: Essential to prevent symptomatic malunion and is often achieved by aligning the anterior surfaces of the fragments. Temporary K-wires may be used to maintain reduction while plates are applied.
Fixation Techniques
Once anatomical reduction is achieved, stable internal fixation is applied.
Plate and Screw Fixation (Most Common)
- Plate Selection: Pre-contoured locking compression plates (LCPs) are the workhorse for middle third clavicle fractures. They are designed to match the S-shape of the clavicle and offer angular stability, which is advantageous in comminuted fractures or osteoporotic bone. Reconstruction plates may be used if pre-contoured plates are unavailable or unsuitable.
- Plate Position:
- Superior plating: Offers maximal biomechanical advantage due to the tension-band effect. However, it can lead to hardware prominence, irritation of supraclavicular nerves, and potentially higher rates of implant removal.
- Anterosuperior or Anterior plating: Often preferred for patient comfort, as it reduces hardware prominence. Biomechanically, it may be less rigid than superior plating but is often sufficient, especially with locking constructs.
- Application Steps:
- Contouring: If using a non-pre-contoured plate, carefully contour it to match the anatomical S-curve of the clavicle. Over-bending or under-bending can lead to cortical impingement or loss of reduction.
- Plate Placement: Position the plate along the desired surface (superior, anterosuperior, or anterior), ensuring adequate purchase in both the medial and lateral main fragments. At least three bicortical screws are generally recommended on each side of the fracture, ideally engaging different cortical areas.
- Lag Screw Principle (for oblique fractures): If the fracture pattern allows, a lag screw can be inserted across the fracture line prior to plate application to achieve interfragmentary compression. This significantly enhances stability.
- Screw Insertion:
- Standard (non-locking) screws: Drill, measure, tap (if needed), and insert screws to achieve compression between the plate and bone.
- Locking screws: Drill and insert locking screws. These provide angular stability without compressing the plate to the bone, which is beneficial for maintaining blood supply and in comminuted fractures.
- Confirming Fixation: Use fluoroscopy to confirm satisfactory reduction, plate position, and screw lengths, ensuring no screw penetration into the joint or soft tissues.
Intramedullary Fixation
Less commonly used in adults for primary fixation due to rotational instability and higher rates of hardware migration or secondary displacement. Options include:
* Flexible intramedullary nails (e.g., Kirschner wires, Ender nails, titanium elastic nails): Primarily used in pediatric fractures or for select simple fracture patterns.
* Intramedullary screws: Limited use, mainly for simple oblique fractures.
Suture Button Constructs (for Lateral Clavicle Fractures)
For highly unstable lateral clavicle fractures (e.g., Neer Type II) with disruption of the coracoclavicular ligaments, suture button constructs are increasingly popular.
* Technique: A small incision is made inferiorly to the coracoid. A drill hole is made through the clavicle and the base of the coracoid process. High-strength suture (e.g., FiberWire) attached to buttons (one cortical button superiorly on the clavicle, one inferiorly on the coracoid) is passed through these holes. The sutures are then tensioned and tied over the buttons, compressing the clavicle to the coracoid and restoring CC ligament function. This may be combined with a small plate for added stability or in comminuted distal clavicle fractures.

Medial Clavicle Fracture Management
Operative management of medial clavicle fractures is rare due to the proximity of mediastinal structures. If indicated (e.g., open fracture, severe displacement with neurovascular compromise, irreducible sternoclavicular dislocation), careful planning and often a cardiothoracic surgeon or vascular surgeon on standby are advised. Fixation is challenging; small plates, tension band wiring, or suture repairs may be utilized.
Wound Closure
After achieving stable fixation, thoroughly irrigate the wound. If the platysma was incised, repair it carefully. Close the deep fascia and subcutaneous layers, followed by skin closure with sutures or staples. A sterile dressing is applied.
Complications and Management
Despite meticulous surgical technique, complications can arise following operative fixation of clavicle fractures. Recognizing and managing these complications effectively is crucial for optimal patient outcomes.
Common Complications
| Complication | Incidence (%) | Salvage Strategies / Management |
|---|---|---|
| Nonunion | 2-10% (operative) | Revision ORIF with plate exchange, bone grafting (autograft/allograft), biologics (PRP, BMPs), IM nail. Address mechanical and biological factors. |
| Malunion | 5-15% (operative) | If symptomatic (pain, impingement, neurovascular symptoms, cosmetic), corrective osteotomy and re-fixation. Otherwise, observation. |
| Infection | 1-5% (superficial) | Superficial: Oral antibiotics, wound care. Deep: Surgical debridement, IV antibiotics, irrigation, possible hardware removal (after union) or exchange. |
| Hardware Prominence | 10-25% | If symptomatic (pain, skin irritation), hardware removal after fracture union (typically 12-18 months). |
| Neurovascular Injury | <1% | Supraclavicular nerve: Observation (neuropraxia), neurolysis or neurectomy for persistent neuroma. Brachial plexus/subclavian vessels: Emergent surgical exploration and repair. |
| Pneumothorax/Hemothorax | <1% (medial third) | Chest tube insertion for drainage and lung re-expansion. Observation, if small. |
| Refracture | 1-3% (after hardware removal) | Re-ORIF with plate and screws, often with a stronger construct or bone grafting. Consider delaying hardware removal until robust cortical healing. |
| Post-traumatic Arthritis | Rare (AC/SC joint) | If symptomatic, AC joint excision (Mumford procedure), SC joint resection or reconstruction. |
| Complex Regional Pain Syndrome (CRPS) | Rare | Multidisciplinary approach: pain management, physical therapy, sympathetic blocks, psychological support. |
Detailed Management Strategies
Nonunion
Nonunion occurs when a fracture fails to heal within an expected timeframe (typically 6-9 months). Risk factors include inadequate fixation, poor biology (e.g., smoking, diabetes, malnutrition, extensive soft tissue stripping), and significant bone loss.
* Diagnosis: Persistent pain, motion at the fracture site, and radiographic evidence of persistent fracture line with sclerotic edges.
* Management: Revision surgery is often required. This typically involves:
* Thorough debridement of the nonunion site to remove fibrous tissue.
* Rigid re-fixation with a stable plate and screws, often requiring a longer, stronger plate or revision of plate position (e.g., from anteroinferior to superior).
* Bone grafting: Autologous cancellous bone graft (iliac crest) is considered the gold standard to provide osteoconductive, osteoinductive, and osteogenic properties. Allografts or synthetic bone substitutes may also be used.
* Addressing biological deficiencies (e.g., smoking cessation).
Malunion
Malunion is healing in an unacceptable anatomical position, leading to residual shortening, angulation, or rotation. While some malunions are asymptomatic, significant malunion can cause:
* Pain: From altered biomechanics or nerve impingement.
* Functional Limitations: Reduced range of motion, weakness (e.g., scapular dyskinesis, impingement symptoms).
* Neurovascular Symptoms: Rarely, compression of the brachial plexus or subclavian vessels.
* Cosmetic Deformity.
* Management: Asymptomatic malunions are typically observed. Symptomatic malunions may require corrective osteotomy to restore length and alignment, followed by stable internal fixation. This is a technically demanding procedure, particularly when significant shortening has occurred.
Infection
Surgical site infections can be superficial or deep.
* Superficial Infection: Usually managed with oral antibiotics, local wound care, and close monitoring.
* Deep Infection: Requires aggressive surgical debridement, thorough irrigation, and intravenous antibiotics guided by culture sensitivities. Hardware retention may be attempted if fixation is stable and union is progressing, but often, hardware removal is necessary after union, or in some cases, a staged approach (debridement, antibiotics, then re-fixation with new implants after infection control).
Hardware Prominence and Irritation
This is a common complaint, particularly with superiorly placed plates, due to the superficial location of the clavicle.
* Management: If symptomatic after fracture union (typically 12-18 months), hardware removal can be performed. Patients should be counseled on the risk of refracture after implant removal, though this risk is low if robust cortical healing is achieved.
Neurovascular Injury
- Supraclavicular Nerve Injury: The most common neurological complication, usually neuropraxia from retraction or direct injury. It results in numbness or dysesthesia over the shoulder/chest. Most cases resolve spontaneously. Persistent painful neuromas may require neurectomy.
- Brachial Plexus or Subclavian/Axillary Vessel Injury: These are rare but devastating complications, often associated with high-energy trauma or highly displaced fractures, particularly medial third. Symptoms include significant neurological deficits or signs of vascular compromise (absent pulses, pallor). Requires immediate surgical exploration and repair, often in conjunction with a vascular or neurosurgeon.
Pneumothorax/Hemothorax
Extremely rare with clavicle fractures, but a potential complication with severely displaced medial third fractures penetrating the pleural apex.
* Diagnosis: Respiratory distress, decreased breath sounds, radiographic findings (chest X-ray, CT scan).
* Management: Chest tube insertion for drainage and lung re-expansion.

Post Operative Rehabilitation Protocols
A structured and progressive postoperative rehabilitation protocol is crucial for optimizing functional recovery, preventing stiffness, and minimizing complications following clavicle fracture fixation. The timeline and intensity of rehabilitation are dictated by the stability of fixation, fracture healing progress, and individual patient factors.
Immediate Postoperative Phase (0-2 Weeks)
- Immobilization: The arm is typically placed in a sling for comfort and protection. The duration of sling use varies but is generally brief (1-2 weeks for comfort, potentially longer for less stable constructs or patient specific factors). The sling protects the repair site, but should not fully restrict passive motion.
- Pain Management: Multimodal analgesia, including NSAIDs, acetaminophen, and short-term opioids, is essential. Regional nerve blocks can also contribute to immediate postoperative comfort.
- Early Range of Motion (ROM):
- Elbow, Wrist, Hand: Active range of motion exercises for the elbow, wrist, and hand should begin immediately to prevent stiffness and promote circulation.
- Pendulum Exercises: Gentle pendulum exercises, initiated within a few days postoperatively, help maintain glenohumeral joint mobility without actively engaging shoulder muscles that cross the fracture site.
- Passive Range of Motion (PROM): Very gentle passive forward flexion and external rotation may be initiated, staying within a pain-free arc and typically not exceeding 90 degrees of flexion, avoiding any active lifting of the arm or pushing through pain.
- Wound Care: Regular dressing changes and monitoring for signs of infection.
Early Rehabilitation Phase (2-6 Weeks)
- Progressive ROM: As pain subsides and radiographic signs of early healing appear (typically around 4-6 weeks), the intensity of PROM and assisted active range of motion (AAROM) exercises is gradually increased.
- Assisted Active Elevation: Using the contralateral arm or a pulley system to gently increase forward flexion and abduction.
- External Rotation: Gradually increasing external rotation exercises.
- Scapular Stabilization: Initiate gentle scapular retraction and protraction exercises to maintain scapular mobility and prepare for shoulder girdle strengthening.
- Avoidance of Stress: Patients are instructed to avoid active lifting, pushing, pulling, or overhead activities with the affected arm. Weightbearing on the affected arm is strictly prohibited.
Intermediate Rehabilitation Phase (6-12 Weeks)
- Active Range of Motion (AROM): Once there is clinical and radiographic evidence of bridging callus formation and early union, active range of motion exercises are fully initiated. The goal is to regain full, pain-free AROM in all planes.
- Gentle Strengthening: Initiate isometric strengthening exercises for the rotator cuff and deltoid, progressing to light resistance with elastic bands. Focus on pain-free movements and proper form.
- Proprioception and Neuromuscular Control: Exercises to restore proprioception and neuromuscular control of the shoulder girdle.
- Weight Restrictions: Lifting restrictions are gradually eased, but heavy lifting (e.g., >5-10 lbs) and impact activities are still avoided.
- Cardiovascular Fitness: Maintaining general fitness with activities like walking or cycling (avoiding impact to the shoulder) is encouraged.
Advanced Rehabilitation and Return to Activity (12+ Weeks)
- Progressive Strengthening: Once clinical and radiographic union is robust (typically 12-16 weeks), aggressive strengthening exercises are implemented. This includes isotonic exercises with increasing resistance for all major shoulder and scapular muscles.
- Sport-Specific Training: For athletes, sport-specific drills and progressive return to activity protocols are initiated under the guidance of a physical therapist.
- Return to Full Activity: Full return to unrestricted activities, including contact sports and heavy lifting, is typically allowed only after complete radiographic union, full strength, and pain-free range of motion are achieved. This often occurs between 3 to 6 months post-surgery, but can vary widely.
- Hardware Removal Consideration: If hardware is prominent or causing symptoms, removal may be considered after solid radiographic union, typically 12-18 months post-fixation. Patients should be aware of a small risk of refracture after hardware removal, particularly if the bone is not fully remodeled.
Throughout all phases, patient education regarding expected recovery, activity precautions, and adherence to the rehabilitation program is paramount. Regular follow-up with the surgeon and physical therapist ensures appropriate progression and addresses any emerging issues.
Summary of Key Literature and Guidelines
The management of clavicle fractures has evolved significantly over the past two decades, largely driven by landmark clinical trials and subsequent meta-analyses. While non-operative treatment remains viable for many fracture patterns, there is a clear trend towards operative fixation for specific indications, particularly displaced middle third fractures in adults.
Middle Third Clavicle Fractures
Historically, displaced middle third clavicle fractures were largely treated non-operatively, despite reported nonunion rates of up to 15-20% and symptomatic malunion rates reaching 30-40%. A pivotal shift in practice occurred with the publication of the Canadian Orthopaedic Trauma Society (COTS) study in 2007. This multicenter randomized controlled trial compared non-operative treatment with plate fixation for displaced middle third clavicle fractures. The study demonstrated that operative fixation resulted in significantly lower rates of nonunion (2.1% vs. 13.9%), improved functional outcomes (DASH scores), and a higher rate of satisfactory cosmetic results at one year. While operative fixation carried a higher risk of early complications (primarily hardware irritation), the overall benefits in terms of union and function have led many surgeons to favor operative treatment for significantly displaced middle third fractures in active adults.
Subsequent meta-analyses and systematic reviews have generally supported the COTS findings, highlighting the benefits of primary plate fixation for displaced middle third fractures, especially those with greater than 2 cm of shortening, 100% displacement, or significant comminution. These studies consistently report improved union rates, better functional scores, and reduced incidence of symptomatic malunion with operative intervention.
Lateral Clavicle Fractures
The management of lateral clavicle fractures is largely guided by the Neer classification system, which categorizes fractures based on their relationship to the coracoclavicular (CC) ligaments.
* Type I: Nondisplaced, lateral to the CC ligaments. Managed non-operatively with excellent outcomes.
* Type II: Fractures medial to the CC ligaments, resulting in detachment of the medial fragment from the stable scapuloclavicular unit. These are inherently unstable due to the upward pull of the trapezius on the medial fragment and high rates of nonunion (up to 30%). Operative fixation (e.g., hook plate, CC ligament repair/reconstruction with suture buttons) is generally recommended for Type II fractures to restore stability and promote union.
* Type III: Fractures through the AC joint, stable with intact CC ligaments. Often managed non-operatively, but may require surgery if significant articular displacement or AC joint instability is present.
* Type IV & V: Complex patterns (medial displacement into trapezius, comminuted) that typically warrant operative fixation.
Recent literature on lateral clavicle fractures emphasizes the effectiveness of CC ligament repair or reconstruction using suture button techniques, either alone or in conjunction with small plates, to achieve stable fixation and restore kinematics, particularly for Neer Type II fractures.
Medial Clavicle Fractures
Medial clavicle fractures are rare, comprising only 2-5% of all clavicle fractures. They are often associated with high-energy trauma and carry a higher risk of complications due to the proximity of vital mediastinal structures. Due to their rarity, strong evidence-based guidelines for operative fixation are limited. Most stable medial clavicle fractures are managed non-operatively. Operative intervention is typically reserved for highly selected cases, such as:
* Open fractures.
* Fractures with significant displacement causing neurovascular compromise (e.g., subclavian vessel compression) or tracheal impingement.
* Irreducible sternoclavicular joint dislocations or unstable physeal injuries (in skeletally immature patients).
Operative fixation in this region is technically challenging and carries significant risks, often necessitating a multidisciplinary approach with cardiothoracic or vascular surgeons.
Current Trends and Guidelines
Current consensus from organizations such as the American Academy of Orthopaedic Surgeons (AAOS) and the Orthopaedic Trauma Association (OTA) generally supports:
* Non-operative management for non-displaced or minimally displaced middle third fractures, most pediatric fractures, and stable lateral or medial third fractures.
* Operative fixation for significantly displaced middle third fractures, unstable lateral clavicle fractures (Neer Type II and V), and specific cases of medial clavicle fracture with vital structure compromise.
The ongoing evolution in implant design, particularly pre-contoured locking plates and suture button constructs, has further refined surgical techniques, offering improved stability and patient comfort. However, the decision to operate must always be balanced against potential complications, patient comorbidities, and individual patient preferences, emphasizing shared decision-making. Future research will likely focus on optimizing rehabilitation protocols, understanding the long-term implications of hardware retention, and exploring biological augmentation for challenging nonunions.
Clinical & Radiographic Imaging
You Might Also Like


