Limb Nerves: Know Where to Look & What to Ask the Patient
Key Takeaway
Looking for accurate information on Limb Nerves: Know Where to Look & What to Ask the Patient? The brachial plexus is a vital nerve network formed by cervical spinal nerve roots C5-T1, which consolidate into trunks and then divide into anterior and posterior divisions, supplying the upper limb. These structures are found from the scalene muscles to behind the clavicle. To accurately diagnose brachial plexus injuries, medical professionals must carefully ask the patient about their symptoms.
Comprehensive Introduction and Patho-Epidemiology
The management of peripheral nerve injuries, particularly those involving the brachial plexus, represents one of the most formidable challenges in modern orthopedic and reconstructive microsurgery. These injuries, often resulting from high-energy trauma, inflict devastating functional deficits on the upper extremity, effectively rendering a limb flail and insensate if left untreated. Understanding the intricate topography of the limb nerves, knowing precisely where to look during surgical exploration, and mastering what to ask the patient during the clinical examination are the foundational pillars of successful neuro-orthopedic management. The brachial plexus is a highly complex neural network, and its pathology requires a profound understanding of both macroscopic anatomy and microscopic fascicular architecture.



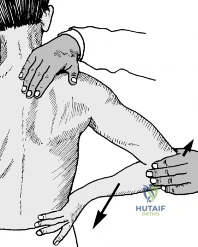
Pathophysiologically, brachial plexus injuries are broadly categorized into open and closed mechanisms. Open injuries, though less common, typically result from penetrating trauma such as stab wounds or high-velocity ballistic injuries, leading to direct laceration of the neural elements. Closed traction injuries, however, constitute the vast majority of adult brachial plexus lesions. The classic mechanism involves a violent depression of the shoulder girdle coupled with contralateral lateral flexion of the cervical spine, a kinematic sequence frequently observed in motorcycle collisions. This extreme tensile force propagates through the neural axis, resulting in a spectrum of injuries ranging from transient neurapraxia to catastrophic preganglionic root avulsions.



Epidemiologically, traumatic brachial plexus injuries predominantly afflict young adult males, correlating strongly with high-risk behaviors and high-speed motor vehicle accidents. Concomitant injuries are highly prevalent and must be meticulously excluded during the primary and secondary trauma surveys. These frequently include fractures of the clavicle, scapula, and cervical spine, as well as potentially life-threatening vascular injuries to the subclavian or axillary arterial axes. Furthermore, obstetrical brachial plexus palsy remains a significant clinical entity, occurring secondary to shoulder dystocia during difficult vaginal deliveries. While historical literature optimistically suggested that up to 80% of these birth injuries achieve spontaneous full recovery by 13 months, contemporary longitudinal studies have challenged this paradigm, revealing a higher incidence of persistent motor deficits, glenohumeral dysplasia, and complex secondary contractures.



Classifying the Nerve Injury Spectrum
Understanding the severity of the neural insult is critical for prognostication and surgical planning. In lesions in continuity, which comprise more than half of all plexus injuries, the nerve roots are typically affected postganglionically between the intervertebral foramina and the clavipectoral fascia. If the injury is a neurapraxia, the conduction block is transient, and full spontaneous recovery is anticipated. However, in axonotmesis, the axons degenerate distally via Wallerian degeneration. Provided the endoneurial tubes remain intact and the axons can penetrate the intraneural scar, regeneration proceeds at a predictable rate of approximately 1 mm per day.


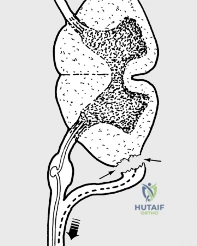
Conversely, ruptured nerve roots represent a complete disruption of the neural elements at the same anatomical level. These severe injuries offer no hope of spontaneous recovery and mandate surgical intervention. Even with advanced microsurgical nerve grafting, functional restoration may be severely compromised by extensive intraneural fibrosis. The most devastating variant is the complete avulsion lesion, wherein the nerve root is violently torn directly from the spinal cord. Because the motor cell bodies reside in the anterior horn of the spinal cord, motor axons undergo irreversible degeneration, yielding denervation fibrillation potentials on electromyography (EMG). Interestingly, because the sensory cell bodies reside in the dorsal root ganglion (which is typically pulled distally but remains intact), the sensory axons do not undergo Wallerian degeneration. This creates a diagnostic paradox in preganglionic lesions: the patient is completely insensate in the affected dermatome, yet sensory nerve action potentials (SNAPs) remain detectable via externally applied electrodes.



Detailed Surgical Anatomy and Biomechanics
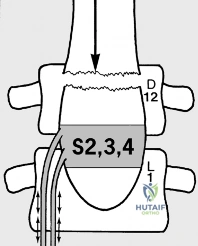
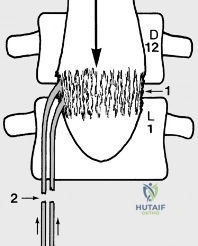
The brachial plexus is a formidable neurovascular structure with an extensive and highly organized distribution. The order in which nerves branch from the plexus is of immense clinical value in determining the exact topographical site of any lesion. The roots of the brachial plexus are formed by the anterior primary rami of C5 through T1 inclusive, with occasional anatomical variants demonstrating contributions from C4 (a "pre-fixed" plexus) or T2 (a "post-fixed" plexus). These roots emerge between the anterior and middle scalene muscles in the neck. It is paramount for the surgeon to distinguish the roots of the brachial plexus (which are extrathecal) from the roots of the segmental spinal nerves (which are intrathecal).



The Supraclavicular Plexus: Roots and Trunks
The first branches of the plexus arise directly from the nerve roots prior to trunk formation. The dorsal scapular nerve, supplying the rhomboids, arises solely from the C5 root. The long thoracic nerve, supplying the serratus anterior, is formed by contributions from C5, C6, and C7, with its most proximal segment arising in conjunction with the dorsal scapular nerve. Additionally, C5 contributes to the phrenic nerve, while C5 through C8 supply the scalenes and longus colli. Paralysis of the hemidiaphragm or winging of the scapula following trauma are critical localizing signs, strongly indicating a very proximal, likely preganglionic, root-level injury.
As the roots progress laterally into the posterior triangle of the neck, they coalesce to form three trunks. The C5 and C6 roots merge to form the upper trunk; the C7 root continues independently as the middle trunk; and the C8 and T1 roots combine to form the lower trunk. Notably, preganglionic sympathetic nerve fibers destined for the upper limb arise from T2–T6, ascend in the sympathetic chain, synapse in the cervicothoracic ganglia, and enter the limb primarily via the lower trunk. Fibers destined for the eye via the stellate ganglion arise specifically from T1; thus, the presence of a Horner’s syndrome (ptosis, miosis, anhidrosis) is a pathognomonic localizing sign for a T1 root avulsion. At the trunk level, only two branches are given off, both from the upper trunk: the suprascapular nerve (supplying the supraspinatus and infraspinatus) and the nerve to the subclavius.
The Infraclavicular Plexus: Divisions, Cords, and Terminal Branches
Behind the clavicle, each of the three trunks bifurcates into an anterior and a posterior division, reflecting the embryological separation of the limb musculature into flexor and extensor compartments. The three posterior divisions unite to form the posterior cord. The anterior divisions of the upper and middle trunks merge to form the lateral cord, while the anterior division of the lower trunk continues independently as the medial cord. As these cords enter the axilla, they intimately embrace the second part of the axillary artery (posterior to the pectoralis minor) in positions corresponding to their anatomical nomenclature.
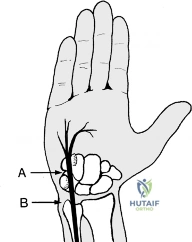
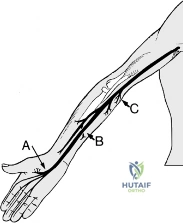
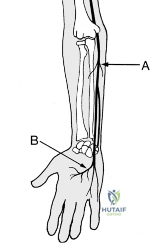
The branching pattern from the cords is highly consistent and clinically vital. The lateral cord (C5, 6, 7) gives rise to the lateral pectoral nerve, the musculocutaneous nerve, and the lateral root of the median nerve. The medial cord (C8, T1) yields the medial pectoral nerve, the medial cutaneous nerves of the arm and forearm, the ulnar nerve, and the medial root of the median nerve. The posterior cord (C5, 6, 7, 8, T1) provides the upper and lower subscapular nerves, the thoracodorsal nerve, the axillary nerve, and the radial nerve. Understanding this terminal arborization is essential when evaluating a patient with a suspected peripheral nerve or plexus lesion, as the specific pattern of motor and sensory deficits will precisely localize the level of disruption.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in brachial plexus injuries is complex, requiring a synthesis of clinical examination, electrodiagnostic data, and advanced imaging. The primary indication for acute surgical exploration (within 72 hours) is an open, sharp penetrating injury where direct primary repair of cleanly transected neural elements is feasible. Additionally, expanding hematomas, concomitant vascular injuries resulting in limb ischemia, and severe crush injuries with impending compartment syndrome represent absolute indications for immediate surgical exploration and decompression.


For the more common closed traction injuries, the approach is initially expectant but highly vigilant. Surgical exploration and reconstruction are indicated if there is no clinical or electromyographic evidence of spontaneous recovery by 3 to 6 months post-injury. Delaying surgery beyond 6 months significantly compromises outcomes due to the progressive, irreversible degradation of motor endplates and muscle atrophy. Specific reconstructive strategies, such as nerve transfers (neurotization), are unequivocally indicated in the presence of preganglionic root avulsions, where the proximal neural stump is unavailable for grafting. Common transfers include utilizing the spinal accessory nerve, intercostal nerves, or redundant fascicles of intact nerves (e.g., the Oberlin transfer) to reinnervate critical targets like the musculocutaneous and suprascapular nerves.

Contraindications to massive brachial plexus reconstruction must be carefully weighed. Absolute contraindications include severe, life-threatening polytrauma where prolonged microscopic surgery would compromise patient survival, and delayed presentations exceeding 12 to 18 months for proximal muscle targets, as the motor endplates will have undergone irreversible fibrosis. Relative contraindications encompass advanced patient age (due to diminished neuroplasticity and regenerative capacity), severe medical comorbidities, and profound psychiatric instability or non-compliance, as the postoperative rehabilitation protocol is exceptionally demanding and spans several years.
| Indication/Contraindication Parameter | Criteria for Surgical Intervention | Criteria for Non-Operative/Salvage Management |
|---|---|---|
| Timing of Injury | Open sharp injury (Immediate); Closed traction with no recovery at 3-6 months | Delayed presentation > 12-18 months (Consider tendon/muscle transfers instead) |
| Lesion Type | Postganglionic rupture (Grafting); Preganglionic avulsion (Nerve transfers) | Transient neurapraxia with early EMG recovery |
| Patient Factors | Young, motivated, compliant, adequate local tissue bed | Advanced age, severe comorbidities, non-compliant, active infection |
| Concomitant Trauma | Stable polytrauma, repaired vascular injury | Unstable hemodynamics, severe traumatic brain injury precluding rehab |

Pre-Operative Planning, Templating, and Patient Positioning
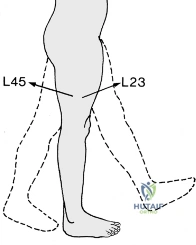
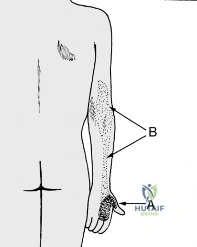
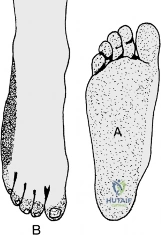
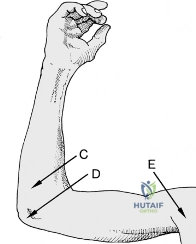
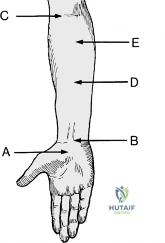
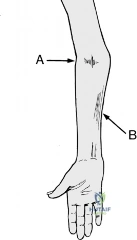
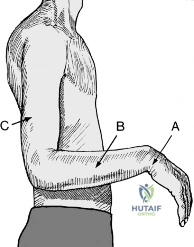
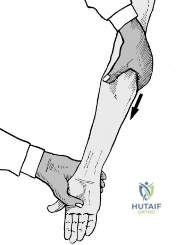
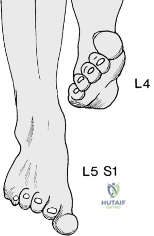
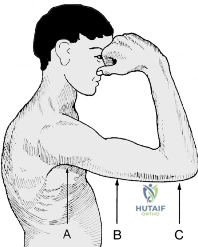
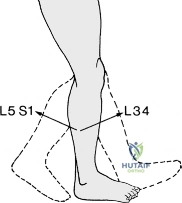
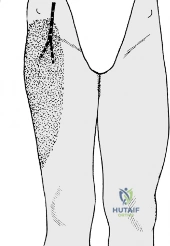
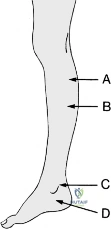
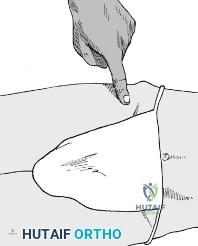
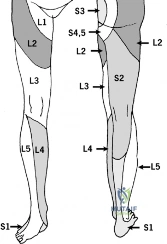
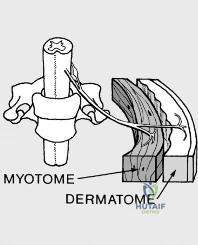
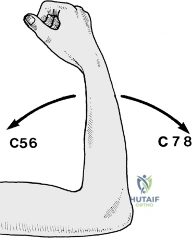
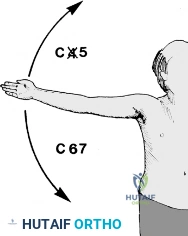
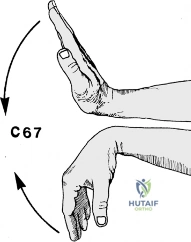
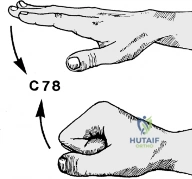
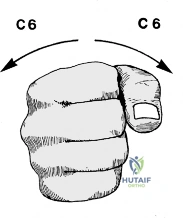
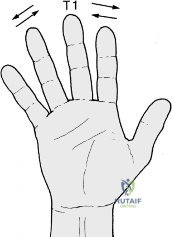
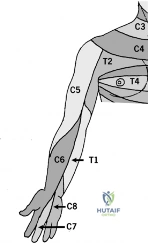
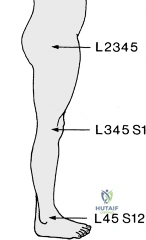
Pre-operative assessment begins with a meticulous clinical examination to determine the longitudinal and transverse extent of the lesion. The surgeon must systematically evaluate myotomes and dermatomes. Normally, two roots produce movement of a joint in one direction, and two in another. However, the upper limb is highly specialized. The shoulder is controlled primarily by C5 (abduction via deltoid and supraspinatus), while adduction is controlled by C6 and C7 (pectoralis major). At the elbow, flexion is C5/C6 (biceps), and extension is C7/C8 (triceps). Wrist dorsiflexion and palmar flexion are surprisingly both controlled by C6/C7. Finger flexion and extension are mediated by C7/C8, while the intrinsic muscles of the hand (abduction/adduction) are innervated solely by T1. Sensation must be mapped, noting that the middle finger represents the C7 dermatome.

Advanced Imaging and Electrodiagnostics
Electrodiagnostic studies (EMG and NCS) are indispensable, typically performed at 3 to 4 weeks post-injury to allow for complete Wallerian degeneration, and repeated sequentially. As previously noted, the presence of SNAPs in an anesthetic dermatome is the hallmark of a preganglionic avulsion. High-resolution MRI neurography has revolutionized pre-operative planning, allowing direct visualization of neuromas, root continuity, and regional edema. CT myelography remains the gold standard for diagnosing root avulsions, classically demonstrating pseudomeningocele formation where the root has been violently extracted from the spinal cord, though a pseudomeningocele can occasionally exist with an intact root.


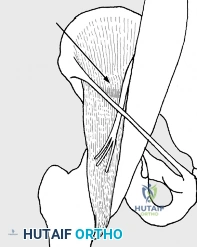
Patient positioning in the operating theater must facilitate simultaneous access to the neck, the entire upper extremity, and potential nerve graft donor sites. The patient is positioned supine with a bump under the ipsilateral scapula to project the shoulder forward. The head is turned to the contralateral side to open the posterior triangle of the neck. The entire ipsilateral upper extremity is prepped free to allow for intraoperative manipulation and assessment of evoked motor responses. Both lower extremities are typically prepped to allow for simultaneous harvesting of the sural nerves, which serve as the primary autologous cable grafts in extensive reconstructions.


Step-by-Step Surgical Approach and Fixation Technique
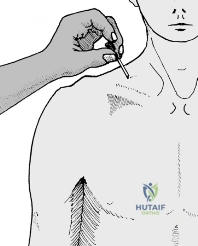
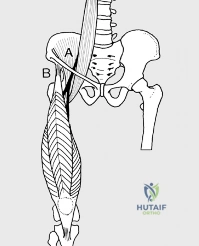
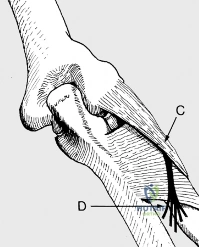
Surgical exploration of the brachial plexus requires an extensile approach capable of exposing the neural elements from the intervertebral foramina down to the axillary terminal branches. The classic supraclavicular incision begins at the posterior border of the sternocleidomastoid muscle, extending transversely across the posterior triangle, parallel and superior to the clavicle. The platysma is divided, and the external jugular vein is either retracted or ligated. Careful identification and preservation of the spinal accessory nerve and the transverse cervical vessels are mandatory. The omohyoid muscle is frequently divided to enhance exposure. The anterior scalene muscle is identified, and the phrenic nerve, which courses obliquely across its anterior surface from lateral to medial, must be meticulously protected.


Intraoperative Assessment and Microsurgical Reconstruction
Once the roots and trunks are exposed, intraoperative nerve stimulation is utilized to assess for continuity and functional conduction. Neuromas-in-continuity present a significant reconstructive dilemma. If conduction is absent, the neuroma must be resected back to healthy, bleeding fascicular tissue under the operating microscope. The "bread-loafing" technique is employed until a normal fascicular architecture is visualized. If the resulting gap cannot be closed without tension—which is almost universally the case in the brachial plexus—autologous cable grafting is performed. Sural nerve grafts are reversed to minimize axonal loss through branching and are
Clinical & Radiographic Imaging Archive