Mastering Lower Lateral Brachial: Advanced Shoulder & Elbow Surgery
Key Takeaway
Here are the crucial details you must know about Mastering Lower Lateral Brachial: Advanced Shoulder & Elbow Surgery. The anterior approach to the shoulder, indicated for stabilization or arthroplasty, utilizes the deltopectoral interval to access the joint. Dissection requires careful identification and retraction of the pectoralis major and deltoid, protecting vital nerves like the axillary and musculocutaneous nerves. Awareness of the broader brachial plexus, impacting areas such as the lower lateral brachial region, is crucial to minimize neurological injury.
Introduction and Epidemiology
The evolution of surgical approaches to the upper extremity has fundamentally transformed the management of complex shoulder and elbow pathology. Mastery of the anterior, anterosuperior, and lower lateral brachial approaches is a prerequisite for orthopedic surgeons managing a diverse array of conditions, ranging from recurrent glenohumeral instability and rotator cuff arthropathy to complex periarticular fractures of the humerus. The incidence of surgical interventions in the upper extremity, particularly shoulder arthroplasty and internal fixation of humerus fractures, has seen an exponential increase over the past two decades. This epidemiological shift is driven by an aging demographic, increased participation in high-impact athletics, and advancements in implant tribology and biomechanical design.
Understanding the precise internervous planes and the intricate neurovascular anatomy of the brachium and shoulder girdle is critical for minimizing iatrogenic morbidity. The anterior approach to the shoulder remains the workhorse for glenohumeral joint access, providing an extensile route that can be extended distally into the lower lateral brachial approach for diaphyseal and distal humeral pathology. This continuum of surgical exposure allows for the seamless management of multi-segmental trauma and complex revision arthroplasty.

The anterosuperior approach, while more limited in its extensile nature, provides unparalleled access to the rotator cuff footprint and the superior glenoid, making it indispensable for reverse total shoulder arthroplasty and superior capsular reconstruction. As the complexity of these procedures increases, a profound understanding of the surgical anatomy, meticulous preoperative planning, and precise execution of the surgical dissection are paramount to achieving optimal functional outcomes and minimizing the risk of catastrophic neurovascular complications.
Surgical Anatomy and Biomechanics
The surgical anatomy of the shoulder and brachium is defined by a complex interplay of muscular envelopes, fascial septa, and critical neurovascular bundles. The anterior approach to the shoulder exploits the deltopectoral interval, a true internervous plane. The deltoid muscle is innervated by the axillary nerve, a terminal branch of the posterior cord of the brachial plexus, while the pectoralis major is innervated by the medial and lateral pectoral nerves.
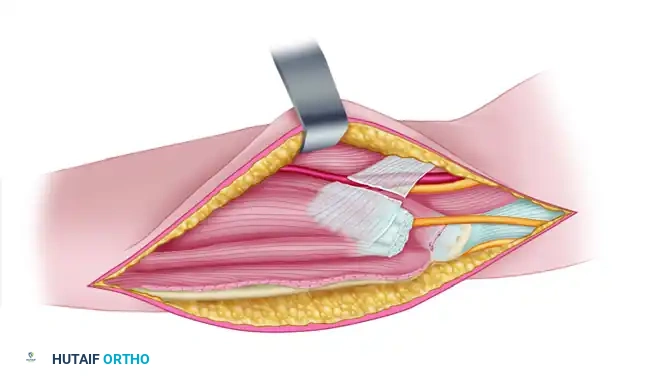
The cephalic vein serves as the primary anatomical landmark for the deltopectoral interval. Retraction of the cephalic vein is historically debated; however, lateral retraction is generally preferred as it preserves the predominant venous tributaries from the deltoid, thereby minimizing postoperative edema and venous congestion. Deep to this interval lies the conjoint tendon, comprising the short head of the biceps brachii and the coracobrachialis. Both structures are innervated by the musculocutaneous nerve. The musculocutaneous nerve typically penetrates the coracobrachialis 5 to 8 centimeters distal to the tip of the coracoid process, entering on its medial aspect. Overzealous medial and distal retraction of the conjoint tendon places this nerve at significant risk for neurapraxia.

Deep to the conjoint tendon lies the subscapularis muscle, the primary internal rotator of the glenohumeral joint and a critical dynamic anterior stabilizer. The inferior border of the subscapularis is demarcated by the anterior humeral circumflex artery and its accompanying venae comitantes, colloquially referred to as the "three sisters." These vessels require meticulous identification and ligation or electrocautery to prevent obscuring hemorrhage during the arthrotomy. The superior border of the subscapularis blends with the supraspinatus tendon at the rotator interval, a triangular space containing the coracohumeral ligament, the superior glenohumeral ligament, and the intra-articular portion of the long head of the biceps tendon.

Transitioning to the lower lateral brachial anatomy, the lateral intermuscular septum divides the arm into anterior and posterior compartments. The lower lateral approach utilizes the plane between the brachialis (innervated dually by the musculocutaneous and radial nerves) and the triceps brachii (innervated by the radial nerve). The radial nerve transitions from the posterior compartment to the anterior compartment by piercing the lateral intermuscular septum approximately 10 centimeters proximal to the lateral epicondyle. Mastery of this anatomical transition zone is critical when extending shoulder approaches distally or when addressing distal third humeral shaft fractures.
Indications and Contraindications
The selection of a surgical approach is dictated by the underlying pathology, the required extent of exposure, and the patient's specific anatomical constraints. The anterior (deltopectoral) approach is highly versatile and is indicated for surgical stabilization of recurrent dislocations, subscapularis and biceps tendon repairs, anatomical and reverse shoulder arthroplasty, and the fixation of proximal humerus fractures. The anterosuperior approach is typically reserved for rotator cuff repairs, subacromial decompression, acromioclavicular reconstructions, greater tuberosity fractures, and specific techniques in reverse shoulder arthroplasty. The lower lateral brachial approach is indicated for distal humerus diaphyseal fractures, exploration of the radial nerve, and lateral column distal humerus fixation.
Contraindications to these approaches are generally relative and include active localized infection, severe medical comorbidities precluding anesthesia, and compromised soft tissue envelopes (e.g., severe burns or prior radiation therapy) that may dictate an alternative surgical trajectory.

| Pathology | Operative Indications | Non Operative Indications |
|---|---|---|
| Proximal Humerus Fractures | Displaced 3 or 4-part fractures, head-splitting fractures, fracture-dislocations, severe varus/valgus angulation. | Nondisplaced or minimally displaced fractures, poor surgical candidates, isolated greater tuberosity fractures < 5mm displacement. |
| Glenohumeral Osteoarthritis | Intractable pain, significant functional deficit, failure of conservative management, intact rotator cuff (for anatomic TSA). | Mild to moderate symptoms, medically unfit, active joint infection, neuropathic joint (Charcot). |
| Rotator Cuff Tear Arthropathy | Pseudoparalysis, intractable pain, combined with significant glenohumeral arthritis (indication for Reverse TSA). | Tolerable symptoms, functional compensation, isolated deltoid paralysis (absolute contraindication for RTSA). |
| Anterior Shoulder Instability | Recurrent dislocations, significant glenoid bone loss (>15-20%), engaging Hill-Sachs lesion, high-demand athletes. | First-time dislocation without significant structural damage, voluntary dislocators, multidirectional instability (initially). |
| Distal Humerus Diaphyseal Fractures | Open fractures, vascular compromise, unacceptable alignment, floating elbow, radial nerve palsy after manipulation. | Acceptable alignment (varus/valgus < 20 degrees, anterior/posterior angulation < 20 degrees, shortening < 3 cm). |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of successful upper extremity surgery. Standard radiographic evaluation should include a true anteroposterior (Grashey) view, an axillary lateral view, and a scapular Y view. For complex fractures and arthroplasty, non-contrast computed tomography (CT) with three-dimensional reconstructions is mandatory to assess glenoid morphology, bone stock, and fracture comminution. Magnetic resonance imaging (MRI) is utilized to evaluate the integrity of the rotator cuff musculature, fatty infiltration (Goutallier classification), and labral pathology.

Patient positioning significantly influences surgical exposure and the ease of intraoperative fluoroscopy. For the anterior and anterosuperior approaches to the shoulder, the patient is typically placed in a modified beach chair position. The head is secured in a specialized headrest to maintain neutral cervical alignment, and the operative arm is draped free to allow for unrestricted manipulation. A pneumatic arm positioner may be utilized to assist with dynamic retraction and limb positioning.
It is critical to ensure that the medial border of the scapula is fully supported by the operating table while the lateral border and the glenohumeral joint extend past the edge of the table, allowing for unobstructed extension of the arm. Arm extension is a vital maneuver for delivering the proximal humerus into the surgical field during arthroplasty and fracture fixation.
When planning a lower lateral brachial approach, the patient may be positioned supine with the arm resting on a radiolucent hand table, or in the lateral decubitus position with the arm draped over a bolster, depending on whether concurrent posterior access is required. Regardless of the position, meticulous padding of all bony prominences, particularly the contralateral ulnar nerve and the common peroneal nerve, is essential to prevent perioperative compression neuropathies. A regional interscalene or supraclavicular nerve block is highly recommended as an adjunct to general anesthesia to minimize volatile anesthetic requirements and provide robust postoperative analgesia.
Detailed Surgical Approach and Technique
Anterior Shoulder Approach
The anterior approach, utilizing the deltopectoral interval, provides extensile access to the anterior glenohumeral joint. The incision can be tailored based on the specific procedure and patient body habitus.
The standard anterior incision spans 10 to 15 centimeters along the deltopectoral interval. It begins just superior to the coracoid process and progresses distally and laterally toward the deltoid tuberosity. Alternatively, for cosmetic considerations in select patients, an axillary incision may be employed. This involves a vertical incision 8 to 10 centimeters long, beginning inferior to the tip of the coracoid and progressing toward the anterior axillary fold. While cosmetically superior, the axillary incision limits proximal and distal extensibility.
Following the skin incision, full-thickness fasciocutaneous flaps are developed. The deltopectoral interval is identified by the presence of the cephalic vein and a distinct fat stripe. The fascia is incised longitudinally. The internervous plane is established by retracting the pectoralis major medially and the deltoid laterally. As previously noted, the cephalic vein is preferentially retracted laterally with the deltoid to preserve its major tributaries.

Deep to the deltopectoral interval, the clavipectoral fascia is encountered and incised lateral to the conjoint tendon. The lateral border of the conjoint tendon is identified. The short head of the biceps and the coracobrachialis are gently displaced medially to expose the underlying subscapularis. Simple medial retraction of the conjoint tendon is often sufficient for subscapularis repair or capsulorrhaphy. If enhanced exposure of the inferior glenoid or brachial plexus is necessary, a coracoid osteotomy may be performed, detaching the conjoint tendon with the tip of the coracoid process.
During medial retraction, the surgeon must be acutely aware of the axillary artery and the cords of the brachial plexus, which lie posterior to the pectoralis minor. To minimize tension on the musculocutaneous nerve, which enters the medial aspect of the coracobrachialis, the arm should be kept adducted and internally rotated while working in the vicinity of the coracoid. Overly aggressive retraction with a self-retaining retractor can induce a profound neurapraxia.
External rotation of the arm brings the subscapularis tendon into the center of the operative field. This maneuver simultaneously increases the distance between the inferior border of the subscapularis and the axillary nerve, which traverses the quadrangular space inferior to the capsule. The inferior border of the subscapularis is identified by locating the "three sisters" (anterior humeral circumflex vessels), which run transversely and must be meticulously ligated or cauterized.
The superior border of the subscapularis blends with the supraspinatus at the rotator interval. The interval is opened to expose the intra-articular long head of the biceps tendon. The subscapularis can be managed via several techniques depending on surgeon preference and the planned procedure: an intratendinous tenotomy (1 to 2 centimeters medial to the lesser tuberosity), a subscapularis peel (detachment directly from the footprint), or a lesser tuberosity osteotomy (detaching the insertion with a bone flake). The underlying capsule is then incised longitudinally or via a T-capsulotomy to enter the glenohumeral joint.
Anterosuperior Shoulder Approach
The anterosuperior approach provides direct access to the superior aspect of the glenohumeral joint, the subacromial space, and the rotator cuff footprint.
An incision is made parallel to the lateral border of the acromion, beginning at the anterolateral corner and extending distally for approximately 4 to 5 centimeters. The subcutaneous tissues are divided to expose the underlying deltoid fascia. The approach utilizes a deltoid-splitting technique, separating the anterior and middle thirds of the deltoid muscle.

It is imperative to limit the distal extent of the deltoid split to no more than 5 centimeters from the lateral edge of the acromion. Extending the split further places the axillary nerve, which courses transversely across the deep surface of the deltoid approximately 5 to 7 centimeters distal to the acromion, at severe risk of transection. A stay suture is often placed at the distal apex of the split to prevent inadvertent propagation of the dissection.
Once the deltoid is split, the subacromial bursa is encountered and excised to expose the rotator cuff. For procedures requiring access to the glenohumeral joint, such as a reverse total shoulder arthroplasty, the supraspinatus tendon (or its remnant) is identified, and the joint is entered through the rotator interval or via a superior capsulotomy.
Lower Lateral Brachial Approach
The lower lateral brachial approach is an extensile continuation that allows for exposure of the distal humerus. The incision begins on the lateral aspect of the arm, in line with the lateral intermuscular septum, and extends distally toward the lateral epicondyle.
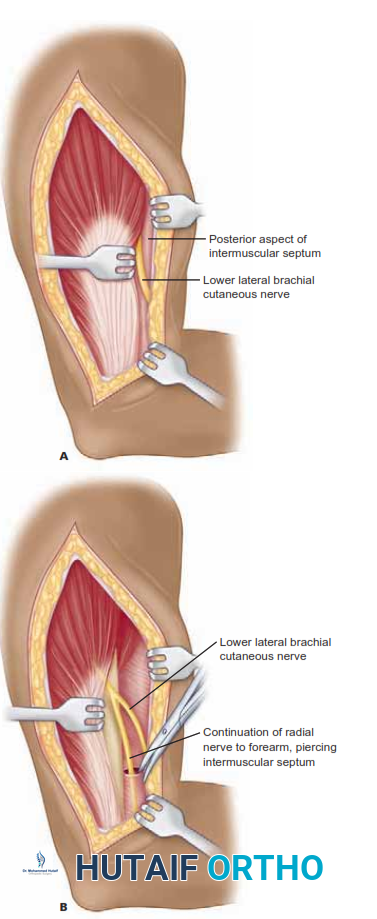
The deep fascia is incised, and the internervous plane between the brachialis anteriorly and the triceps posteriorly is developed. The critical step in this approach is the early identification and protection of the radial nerve. The nerve pierces the lateral intermuscular septum to enter the anterior compartment approximately 10 centimeters proximal to the radiocapitellar joint.
The dissection proceeds by elevating the triceps off the posterior aspect of the lateral intermuscular septum and the brachialis off the anterior aspect. The radial nerve is identified as it crosses the septum and is carefully mobilized and protected with a vessel loop. Once the nerve is secured, the brachialis can be elevated from the anterior humeral diaphysis, providing excellent exposure for the application of lateral column plates or the exploration of distal diaphyseal fractures.
Complications and Management
Surgical intervention in the shoulder and brachium carries inherent risks, primarily related to neurovascular injury, mechanical failure of repairs, and infection. A profound understanding of anatomical landmarks is the most effective prophylactic measure against these complications.
Nerve injuries are among the most devastating complications. The axillary nerve is at risk during the deltoid split of the anterosuperior approach and during inferior capsular release in the anterior approach. The musculocutaneous nerve is vulnerable to traction injury during medial retraction of the conjoint tendon. The radial nerve is at high risk during the lower lateral brachial approach and during the placement of distal interlocking screws in intramedullary nailing or plating.
Vascular injuries, while less common, can result in significant morbidity. Failure to adequately ligate the anterior humeral circumflex vessels ("three sisters") can lead to postoperative hematoma formation, which increases the risk of infection and compromises wound healing.
Subscapularis failure following an anterior approach is a recognized complication, particularly in the setting of total shoulder arthroplasty. Failure of the repair leads to anterior instability, weakness in internal rotation, and poor functional outcomes. Meticulous repair techniques, whether utilizing transosseous sutures for a peel or robust fixation for an osteotomy, are critical.

| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Axillary Nerve Injury | 1% - 2% | Prevention: Limit deltoid split to <5cm from acromion; stay close to capsule during inferior release. Salvage: Observation for neurapraxia; nerve exploration and grafting if no clinical/EMG recovery at 3-6 months. |
| Musculocutaneous Neurapraxia | 2% - 5% | Prevention: Avoid aggressive medial retraction of conjoint tendon; keep arm adducted/internally rotated during exposure. Salvage: Usually transient; supportive care and physical therapy. |
| Radial Nerve Palsy | 3% - 10% (in distal humerus trauma) | Prevention: Direct visualization and protection during lower lateral approach; avoid blind retractor placement. Salvage: Tendon transfers (e.g., pronator teres to ECRB) if permanent; nerve exploration if transection suspected. |
| Subscapularis Repair Failure | 2% - 8% | Prevention: Robust transosseous repair or lesser tuberosity osteotomy; strict adherence to postoperative external rotation limits. Salvage: Revision repair; pectoralis major transfer for chronic, irreparable failure. |
| Postoperative Infection (P. acnes) | 1% - 3% | Prevention: Preoperative optimization; benzoyl peroxide prep; meticulous hemostasis; prophylactic antibiotics (including coverage for Cutibacterium acnes). Salvage: Irrigation and debridement; implant retention vs. two-stage revision depending on chronicity. |
Post Operative Rehabilitation Protocols
Postoperative rehabilitation is inextricably linked to the surgical approach and the specific structures repaired or reconstructed. Communication between the orthopedic surgeon and the physical therapy team is essential to ensure that the rehabilitation protocol protects the surgical repair while optimizing the return of functional range of motion and strength.
For procedures utilizing the anterior approach involving a subscapularis takedown and repair (e.g., anatomic total shoulder arthroplasty or open stabilization), the rehabilitation protocol must strictly protect the subscapularis during the initial healing phase.
Phase I: Protection Phase (Weeks 0-4)
The patient is immobilized in a sling. Passive range of motion (PROM) is initiated immediately but is strictly limited to prevent tension on the subscapularis. External rotation is typically limited to 30 degrees (or the safe limit determined intraoperatively), and forward elevation is limited to 90-120 degrees. Active internal rotation and extension are prohibited.
Phase II: Active-Assisted Range of Motion (Weeks 4-8)
The sling is discontinued. Active-assisted range of motion (AAROM) and active range of motion (AROM) are initiated. External rotation limits are gradually advanced. Isometric strengthening of the deltoid and intact rotator cuff musculature begins, but internal rotation strengthening is delayed until week 6 to 8 to ensure subscapularis tendon-to-bone healing.
Phase III: Strengthening Phase (Weeks 8-12)
Progressive resistive exercises are introduced. Focus is placed on periscapular stabilization, rotator cuff strengthening, and restoring full, symmetric active range of motion. Closed kinetic chain exercises may be incorporated to enhance proprioception.
Phase IV: Return to Activity (Weeks 12+)
Advanced strengthening and sport-specific or occupation-specific functional training are emphasized. Return to heavy lifting or high-impact activities is generally delayed until 4 to 6 months postoperatively, contingent upon the achievement of symmetric strength and the absence of pain.
For procedures utilizing the anterosuperior approach (e.g., rotator cuff repair), the protocol is dictated by the size of the tear and the tension of the repair. Protection of the supraspinatus requires delayed active forward elevation and abduction. For the lower lateral brachial approach involving fracture fixation, early active range of motion of the elbow and wrist is encouraged to prevent stiffness, provided the osseous fixation is biomechanically stable.
Summary of Key Literature and Guidelines
The foundational techniques for the surgical approaches described herein are deeply rooted in the anatomical studies and clinical series of early pioneers in orthopedic surgery. The deltopectoral approach, originally popularized by Neer in the 1970s for the insertion of the first generation of shoulder prostheses, remains the gold standard for anterior access. Neer's emphasis on the preservation of the deltoid origin and insertion revolutionized the functional outcomes of shoulder arthroplasty.
Subsequent literature has heavily focused on the management of the subscapularis tendon during the anterior approach. Gerber et al. have published extensively on the biomechanical and clinical outcomes of subscapularis repair, demonstrating that failure of the repair correlates directly with poor functional outcomes and anterior instability. The debate between subscapularis tenotomy, peel, and lesser tuberosity osteotomy remains prominent in the literature. Recent meta-analyses suggest that lesser tuberosity osteotomy may provide superior bone-to-bone healing and a lower rate of structural failure, although clinical outcome scores often remain comparable across techniques when performed meticulously.
The anatomical nuances of the anterosuperior approach and the critical importance of protecting the axillary nerve have been well-documented by Hoppenfeld and deBoer in their seminal texts on surgical exposures. Their cadaveric studies define the safe zone for the deltoid split, establishing the 5-centimeter rule that is universally taught in orthopedic training programs today.
For the lower lateral brachial approach, recent guidelines from the Orthopaedic Trauma Association (OTA) and the American Academy of Orthopaedic Surgeons (AAOS) emphasize the necessity of direct visualization of the radial nerve during the management of distal humerus fractures. Literature regarding iatrogenic radial nerve palsy underscores that while the majority of traction injuries recover spontaneously, direct surgical exploration is mandated if the nerve is not visualized during the initial exposure or if there is a sharp, penetrating mechanism of injury.
Mastery of these surgical approaches requires a synthesis of this established literature, an intimate knowledge of three-dimensional anatomy, and rigorous adherence to precise surgical technique. As implant technology and surgical indications continue to expand, the foundational principles of the anterior, anterosuperior, and lower lateral brachial approaches will remain the bedrock of advanced shoulder and elbow surgery.
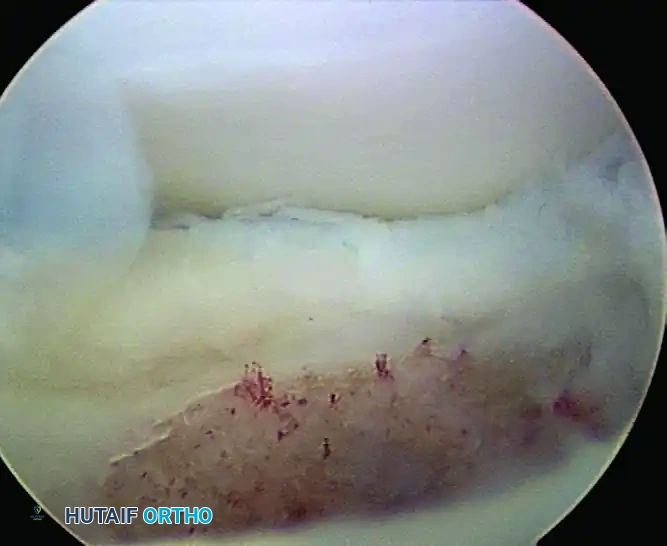
Clinical & Radiographic Imaging
You Might Also Like