Arthroscopic Olecranon Osteophyte Resection Guide
Key Takeaway
Valgus extension overload syndrome frequently results in the formation of posterior olecranon osteophytes, causing posterior impingement and pain in overhead athletes. Arthroscopic resection involves meticulous visualization of the posterior compartment, identification of the impinging osteophyte, and precise burring of 2 to 3 mm of the olecranon tip. This restores terminal extension while preserving the critical stabilizing anatomy of the ulnohumeral articulation.
INTRODUCTION AND PATHOMECHANICS
Posterior elbow impingement, frequently manifesting as Valgus Extension Overload (VEO) syndrome, is a well-documented clinical entity primarily affecting overhead athletes, such as baseball pitchers, javelin throwers, tennis players, and golfers. The repetitive, high-velocity valgus stress applied to the elbow during the acceleration and deceleration phases of throwing generates profound compressive forces across the radiocapitellar joint and the posteromedial ulnohumeral articulation.
Over time, this repetitive microtrauma leads to the formation of reactive osteophytes at the posteromedial tip of the olecranon. As the elbow is forced into terminal extension, these osteophytes impinge within the olecranon fossa, resulting in localized chondromalacia, loose body formation, and debilitating posterior elbow pain. Furthermore, the chronic inflammatory response can lead to capsular hypertrophy. A thickened posterolateral capsule—specifically a radiocapitellar plica—can become fibrotic and interpose within the joint, causing mechanical symptoms such as snapping or popping during extension.
Arthroscopic removal of the olecranon tip and associated osteophytes is a highly effective intervention for patients who have failed conservative management. However, the procedure demands a rigorous understanding of ulnohumeral biomechanics to prevent iatrogenic instability.
Surgical Warning: The olecranon tip is a critical secondary bony restraint to valgus stress. Resection of the olecranon osteophyte must be strictly limited to the pathological bone (typically 2 to 3 mm). Over-resection transfers excessive strain to the anterior bundle of the Medial Ulnar Collateral Ligament (MUCL), potentially precipitating catastrophic valgus instability in the throwing athlete.
CLINICAL EVALUATION AND DIAGNOSIS
Patient Presentation
Patients typically present with an insidious onset of posteromedial or posterolateral elbow pain that is exacerbated by the terminal extension phase of their respective sport. Key clinical findings include:
* Pain and Tenderness: Localized tenderness along the posteromedial olecranon, the radiocapitellar joint, and the anconeus fossa.
* Mechanical Symptoms: Intermittent catching, locking, or popping, which may indicate the presence of intra-articular loose bodies or a pathological radiocapitellar plica.
* Loss of Motion: A characteristic flexion contracture or pain upon forced terminal extension (the "valgus extension overload test").
Diagnostic Imaging
- Radiographs: Standard anteroposterior (AP), lateral, and axial views of the elbow are mandatory. The axial view is particularly useful for visualizing posteromedial olecranon osteophytes and loose bodies within the olecranon fossa.
- Magnetic Resonance Imaging (MRI): MRI or MR arthrography is highly sensitive for detecting chondral defects, loose bodies, and MUCL integrity. Crucially, persistent posterolateral pain may be attributed to a pathological plica; an MRI demonstrating capsular thickening of 3 mm or greater on axial views is highly indicative of a symptomatic posterolateral plica requiring arthroscopic debridement.
INDICATIONS FOR SURGERY
Initial management of posterior elbow impingement and plica syndrome should always be non-operative. Conservative modalities include:
1. Pharmacotherapy: A scheduled course of nonsteroidal anti-inflammatory drugs (NSAIDs).
2. Activity Modification: Relative rest and cessation of the offending athletic activity.
3. Physical Therapy: A structured flexibility and dynamic stabilization program focusing on the flexor-pronator mass and periscapular musculature.
4. Corticosteroid Injections: Intra-articular injection of corticosteroids into the posterolateral or radiocapitellar space can provide significant diagnostic and therapeutic relief.
Surgical Indications:
Arthroscopic intervention is indicated when a patient experiences persistent, activity-limiting pain and mechanical symptoms despite a minimum of 3 to 6 months of comprehensive conservative treatment, accompanied by radiographic evidence of impinging osteophytes, loose bodies, or a pathological plica.
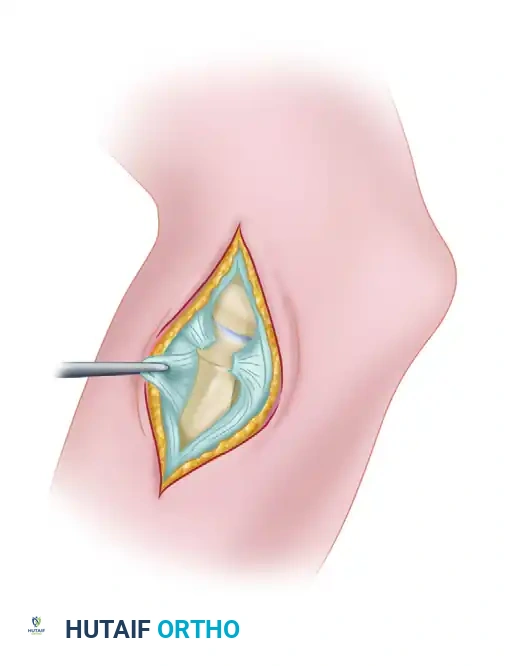
SURGICAL ANATOMY AND PORTAL PLACEMENT
A thorough understanding of the neurovascular anatomy surrounding the elbow is paramount to safely establishing arthroscopic portals.
- Proximal Anterolateral Portal: Located 2 cm proximal and 1 cm anterior to the lateral epicondyle. The radial nerve is the structure at risk; maintaining contact with the anterior humerus during trocar insertion minimizes this risk.
- Anteromedial Portal: Located 2 cm distal and 2 cm anterior to the medial epicondyle. The medial antebrachial cutaneous nerve and the median nerve are at risk. This portal is typically established under direct intra-articular visualization from the anterolateral portal.
- Posterior Portal: Located 3 cm proximal to the olecranon tip, directly in the midline over the triceps tendon.
- Posterolateral Portal: Located 2 to 3 cm proximal to the olecranon tip, just lateral to the triceps border. This portal provides excellent visualization of the olecranon fossa and the radiocapitellar articulation.
SURGICAL TECHNIQUE: REMOVAL OF OLECRANON TIP AND OSTEOPHYTES
Step 1: Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia, often supplemented with a regional supraclavicular or axillary nerve block for postoperative pain control.
The patient may be placed in the supine, prone, or lateral decubitus position based on the surgeon's preference:
* Supine Position: The arm is suspended using an overhead traction boom. This allows for excellent access to the anterior compartment but can make posterior access slightly more cumbersome.
* Prone Position: The arm is draped over a well-padded arm board. This position provides superior, unobstructed access to the posterior compartment and olecranon fossa, making it highly advantageous for VEO procedures.
* Lateral Decubitus: The arm is supported over a bolster. This offers a balance between anterior and posterior access.
A non-sterile tourniquet is applied high on the brachium, and the arm is prepped and draped in a standard sterile fashion.
Step 2: Anterior Compartment Diagnostic Arthroscopy
- Insufflate the joint with 20 to 30 mL of normal saline via the soft spot (center of the triangle formed by the lateral epicondyle, radial head, and olecranon tip) to distend the capsule and displace neurovascular structures anteriorly.
- Establish the proximal anterolateral portal using a superficial skin incision and blunt dissection with a mosquito hemostat down to the capsule. Insert the arthroscope.
- Establish the anteromedial portal under direct visualization using an outside-in spinal needle localization technique.
- Perform a systematic diagnostic sweep of the anterior compartment. Inspect the coronoid, the anterior radiocapitellar joint, and the anterior capsule. Remove any anterior loose bodies and debride any anterior capsular adhesions if a flexion contracture is present.
Step 3: Transition to the Posterior Compartment
- Once the anterior compartment has been fully addressed, turn attention to the posterior compartment.
- Establish the posterolateral portal for visualization and the direct posterior portal (trans-triceps) for instrumentation.
- Clear the olecranon fossa of any fibrotic tissue or synovitis using a 4.0-mm motorized shaver.
- Meticulously observe the posteromedial and posterolateral gutters, as well as the posterior aspect of the radiocapitellar joint. Ensure that there are no hidden loose bodies. If a thickened, fibrotic posterolateral plica (>3 mm) is identified snapping across the radiocapitellar joint, resect it using a combination of a shaver and radiofrequency ablation wand.
Step 4: Identification and Resection of the Olecranon Osteophyte
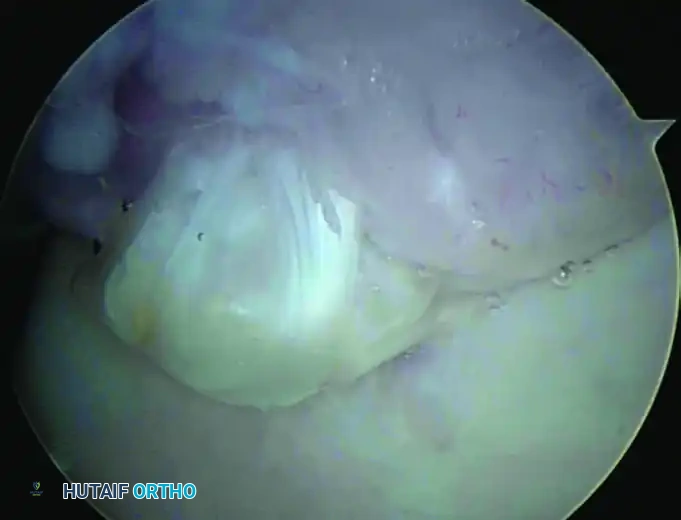
With the olecranon fossa cleared, bring the elbow into varying degrees of extension to dynamically observe the impingement of the olecranon tip against the fossa. The pathological osteophyte will typically be visible at the superior tip of the olecranon.
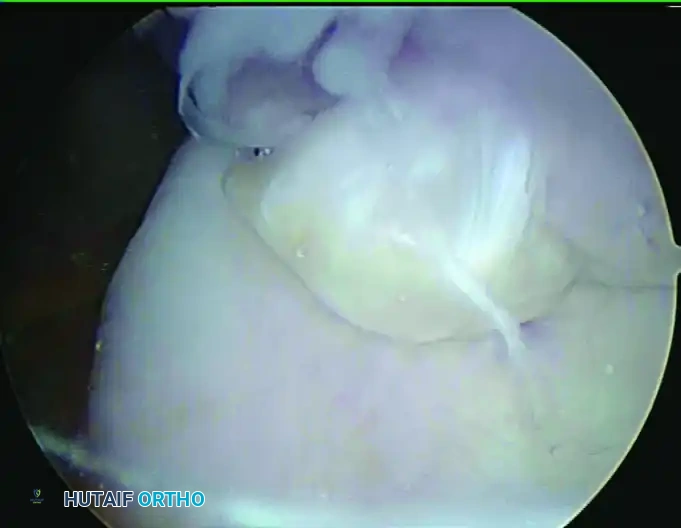
FIGURE 52-69 A and B: Arthroscopic visualization of the osteophyte at the tip of the olecranon superiorly. Note that the trochlea is oriented inferiorly in this supine patient setup.
- Introduce a small arthroscopic osteotome or a 4.0-mm hooded arthroscopic burr through the working portal.
- Begin resecting the identified osteophyte at the tip of the olecranon.
- Crucial Technical Pearl: Resection must be strictly limited. Remove only the impinging osteophytic bone. No more than 2 to 3 mm of bone should be removed. The normal contour of the olecranon must be preserved to maintain the bony congruency of the ulnohumeral joint.
- Dynamically test the elbow by bringing it into terminal extension. Ensure that the impingement has been completely resolved and that the newly contoured olecranon tip seats smoothly within the olecranon fossa without abutting the humerus.
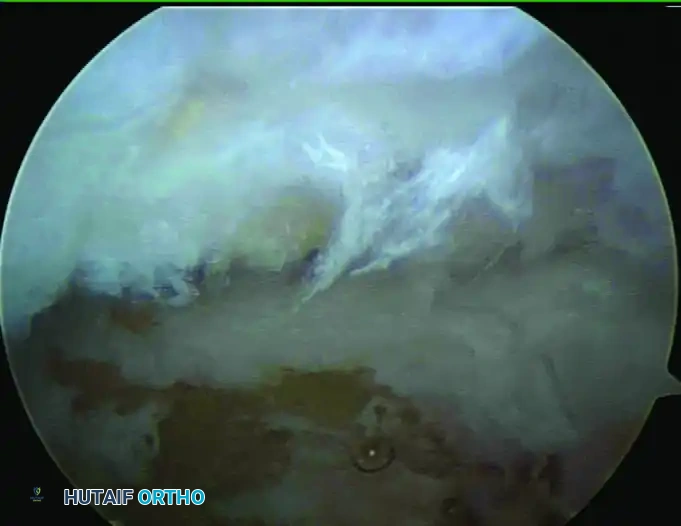
FIGURE 52-69 C: The tip of the olecranon after precise osteophyte resection. The normal anatomical contour has been restored without compromising the structural integrity of the ulnohumeral joint.
Step 5: Chondroplasty and Microfracture
- Inspect the articular surfaces of the olecranon and the corresponding olecranon fossa for chondral damage, which frequently accompanies VEO.
- Use a shaver or curette to debride any unstable, fibrillated cartilage flaps, creating stable, vertical margins (smooth chondral lesions).
- If areas of full-thickness cartilage loss with exposed subchondral bone are encountered, utilize a microfracture technique.
- Introduce an arthroscopic awl and create multiple fenestrations in the exposed subchondral bone plate, spaced approximately 3 to 4 mm apart. Penetrate to a depth of 2 to 3 mm until marrow fat droplets and blood are seen extruding from the holes upon lowering the arthroscopic fluid pressure. This stimulates the release of mesenchymal stem cells to form a fibrocartilage healing response.
Step 6: Closure
- Thoroughly irrigate the joint to remove all bone debris and cartilage fragments, which could act as a nidus for heterotopic ossification or third-body wear.
- Evacuate all fluid from the joint.
- Close the portal sites using non-absorbable simple sutures or adhesive skin closures.
- Apply a sterile, bulky compressive dressing to minimize postoperative hemarthrosis and swelling.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative rehabilitation following arthroscopic olecranon osteophyte resection is phased and tailored to the specific procedures performed (e.g., whether microfracture was required).
Phase I: Immediate Postoperative Phase (Days 1-10)
- Immobilization: The arm is placed in a sling for comfort only. Rigid immobilization is avoided to prevent arthrofibrosis.
- Range of Motion (ROM): Active and active-assisted ROM exercises for the elbow, wrist, and hand are initiated on postoperative day 1 or 2. The goal is to achieve full, symmetric ROM as quickly as tolerated.
- Inflammation Control: Cryotherapy and elevation are utilized aggressively to manage edema and pain.
- Note on Microfracture: If microfracture was performed, weight-bearing through the arm is strictly restricted, though early ROM remains critical to stimulate fibrocartilage maturation.
Phase II: Intermediate Phase (Weeks 2-6)
- Strengthening: Once full, painless ROM is achieved, progressive isotonic strengthening of the biceps, triceps, wrist flexors/extensors, and pronator/supinator muscle groups is initiated.
- Scapular Stabilization: Integration of periscapular and core strengthening is vital, particularly for overhead athletes, to ensure proper kinetic chain mechanics.
Phase III: Advanced Strengthening and Return to Sport (Weeks 6-12+)
- Plyometrics: Introduction of upper extremity plyometric exercises.
- Interval Throwing Program: For throwing athletes, a structured, progressive interval throwing program is initiated around week 8 to 10, provided they have full, painless ROM, normal strength, and no localized tenderness.
- Return to Play: Unrestricted return to competitive overhead sports is typically achieved between 3 to 5 months postoperatively, contingent upon the athlete passing sport-specific functional testing.
COMPLICATIONS AND PITFALLS
While arthroscopic resection of olecranon osteophytes is highly successful, surgeons must be vigilant regarding potential complications:
Clinical Pearl - Avoiding Iatrogenic Instability: The most devastating complication specific to this procedure is iatrogenic valgus instability. The olecranon tip provides significant resistance to valgus stress when the elbow is extended. Resecting more than 3 mm of the olecranon tip exponentially increases the tension on the anterior band of the MUCL. In a throwing athlete, this can rapidly lead to MUCL failure, necessitating complex ligamentous reconstruction. Always measure resection depth meticulously.
- Neurological Injury: The ulnar nerve is highly vulnerable during posterior and posteromedial portal placement and instrumentation. Transient ulnar neuropraxia can occur from fluid extravasation or direct trauma. Strict adherence to anatomical landmarks and the use of blunt dissection techniques are mandatory.
- Heterotopic Ossification (HO): Inadequate irrigation of bone debris following burring can lead to HO. Copious lavage at the conclusion of the procedure is essential. In high-risk patients, a short postoperative course of NSAIDs (e.g., Indomethacin) may be considered as prophylaxis.
- Incomplete Resection: Failure to adequately visualize and resect the entire impinging osteophyte will result in persistent mechanical symptoms and pain, often requiring revision surgery. Dynamic intraoperative testing is the best method to confirm adequate decompression.
You Might Also Like