Medial Epicondylectomy: Surgical Technique & Ulnar Nerve Decompression

Key Takeaway
Medial epicondylectomy is a highly effective surgical intervention for cubital tunnel syndrome, designed to decompress the ulnar nerve by removing the medial epicondyle. This procedure eliminates the bony prominence causing friction and tension during elbow flexion. Careful preservation of the ulnar collateral ligament and meticulous smoothing of the osteotomy site are critical to preventing postoperative instability and recurrent neuropathy.
Introduction to Medial Epicondylectomy
Cubital tunnel syndrome is the second most common compression neuropathy of the upper extremity, characterized by entrapment or traction of the ulnar nerve at the medial elbow. While simple decompression and anterior transposition (subcutaneous, intramuscular, or submuscular) are frequently utilized, medial epicondylectomy remains a highly effective, time-tested surgical intervention.
By excising the medial epicondyle, the surgeon effectively removes the bony prominence that acts as a fulcrum for the ulnar nerve. This allows the nerve to glide anteriorly during elbow flexion, significantly reducing both intraneural pressure and longitudinal traction. Furthermore, medial epicondylectomy avoids the extensive soft-tissue dissection and potential devascularization associated with formal submuscular transpositions, making it an elegant solution for specific anatomical variants of ulnar neuropathy.
This comprehensive guide details the postgraduate-level surgical technique, biomechanical rationale, and critical anatomical considerations required to perform a safe and effective medial epicondylectomy.
Clinical Indications and Patient Selection
The decision to perform a medial epicondylectomy over alternative decompressive techniques relies on a thorough clinical evaluation, electromyography (EMG), and intraoperative findings.
Primary Indications
- Severe Cubital Tunnel Syndrome: Patients with advanced motor weakness, intrinsic muscle atrophy, or persistent sensory deficits who require more than a simple in situ decompression.
- Subluxating Ulnar Nerve: A nerve that snaps over the medial epicondyle during flexion is prone to friction neuritis. Removing the epicondyle eliminates this mechanical conflict.
- Bony Abnormalities: Post-traumatic cubitus valgus, osteophyte formation at the medial epicondyle, or heterotopic ossification impinging on the cubital tunnel.
- Failed Simple Decompression: Revision surgery where perineural fibrosis tethers the nerve against the epicondyle.
Contraindications
- Pre-existing Valgus Instability: Patients with a compromised ulnar collateral ligament (UCL) are poor candidates, as the procedure risks further destabilizing the medial elbow.
- Throwing Athletes: Overhead athletes (e.g., baseball pitchers) rely heavily on the anterior bundle of the UCL and the flexor-pronator mass for dynamic valgus stability. Medial epicondylectomy is generally contraindicated in this demographic.
💡 Clinical Pearl: The "Mini-Transposition" Effect
Medial epicondylectomy is often conceptualized as a "mini-transposition." By removing the bony prominence, the nerve naturally seeks a more anterior, tension-free position in the subcutaneous tissues without requiring the formal creation of a fascial sling or muscular bed.
Surgical Anatomy and Biomechanics
A profound understanding of medial elbow anatomy is non-negotiable to prevent catastrophic complications, particularly valgus instability and iatrogenic nerve injury.
The Ulnar Nerve and Compression Sites
The ulnar nerve transitions from the anterior compartment of the arm to the posterior compartment by piercing the medial intermuscular septum at the Arcade of Struthers (approximately 8 cm proximal to the medial epicondyle). It then travels behind the medial epicondyle through the cubital tunnel, roofed by Osborne’s fascia (the cubital tunnel retinaculum) and floored by the posterior band of the UCL and the joint capsule.
The Medial Epicondyle and the UCL
The medial epicondyle is the origin of the common flexor-pronator mass (pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris).
Crucially, the anterior bundle of the ulnar collateral ligament (UCL)—the primary restraint to valgus stress at the elbow—originates from the anteroinferior surface of the medial epicondyle, slightly deep and distal to the flexor-pronator origin.
🚨 Surgical Warning: UCL Preservation
The most devastating complication of a medial epicondylectomy is iatrogenic transection of the anterior bundle of the UCL. The osteotomy must be strictly limited to the medial epicondyle, preserving the sublime tubercle and the anteroinferior base where the ligament attaches.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or a regional brachial plexus block (supraclavicular or axillary) is utilized.
- Positioning: The patient is placed in the supine position. The operative arm is abducted and externally rotated onto a radiolucent hand table.
- Tourniquet: A sterile pneumatic tourniquet is applied high on the brachium. The arm is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or 100 mm Hg above systolic pressure).
- Preparation: Standard orthopedic skin preparation and draping are performed, ensuring the elbow can be freely flexed and extended throughout the procedure.
Step-by-Step Surgical Technique
1. Skin Incision and Superficial Dissection
Make an 8-cm longitudinal skin incision along the anatomical course of the ulnar nerve. The incision should be centered directly over the posterior aspect of the medial epicondyle, extending 4 cm proximally and 4 cm distally.
FIGURE 62-34A: Skin incision centered over the posterior aspect of the medial epicondyle.
Carry the incision sharply through the subcutaneous tissue down to the deep fascia.
🚨 Pitfall: Cutaneous Nerve Injury
Extreme caution must be exercised during the superficial dissection to identify and protect the branches of the medial antebrachial cutaneous (MABC) nerve. The posterior branch of the MABC frequently crosses the operative field just distal to the medial epicondyle. Transection will result in a painful postoperative neuroma and numbness over the medial forearm.
2. Ulnar Nerve Identification and Neurolysis
Incise the deep fascia to expose the ulnar nerve proximal to the cubital tunnel. Identify the nerve and carefully free it from surrounding scar tissue and fascial adhesions.
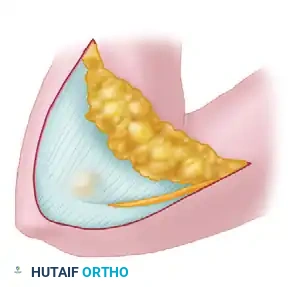
FIGURE 62-34B: Exposing and freeing the ulnar nerve from the proximal fascial layers.
Proceed distally to release Osborne’s fascia (the cubital tunnel retinaculum) and the tendinous arch between the humeral and ulnar heads of the flexor carpi ulnaris (FCU).
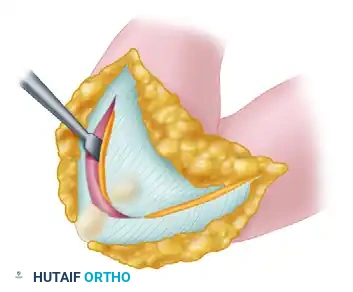
FIGURE 62-34C: The ulnar nerve is meticulously freed from scar tissue posterior to the medial epicondyle and from beneath the tendinous arch of the FCU.
During this exposure, retract the ulnar nerve posteriorly using a moistened Penrose drain or vessel loop. Do not apply excessive traction. It is imperative to protect the mesoneurium (the extrinsic longitudinal blood supply to the nerve) to prevent postoperative ischemic neuropathy.
3. Exposure of the Medial Epicondyle
With the ulnar nerve safely retracted posteriorly, direct your attention to the medial epicondyle. Expose the epicondyle subperiosteally. Carefully incise the common flexor-pronator origin longitudinally and elevate it anteriorly.
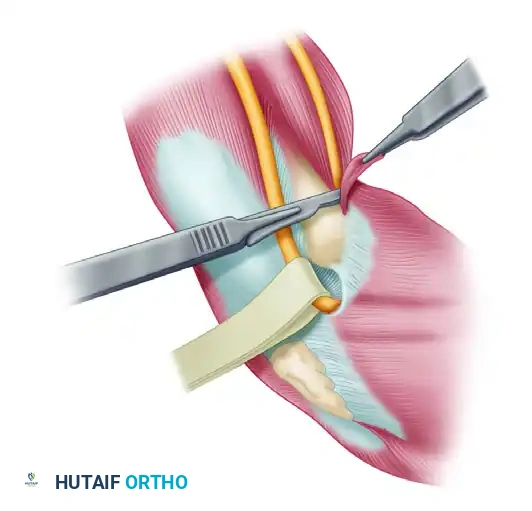
FIGURE 62-33A: The ulnar nerve is protected with a vessel loop, and the common flexor-pronator origin is elevated from the medial epicondyle, exposing the bone for osteotomy.
Maintain strict awareness of the UCL. The dissection should remain superficial to the joint capsule and the anterior bundle of the UCL.
4. The Osteotomy
This is the most critical step of the procedure. Using a sharp, broad osteotome or a rongeur, remove the entire medial epicondyle.
The trajectory of the osteotomy is paramount. The guide for the correct plane of the osteotomy is the medial border of the trochlea. The cut should be directed distally and slightly laterally, ensuring that the base of the epicondyle (where the anterior bundle of the UCL attaches) is left completely intact.
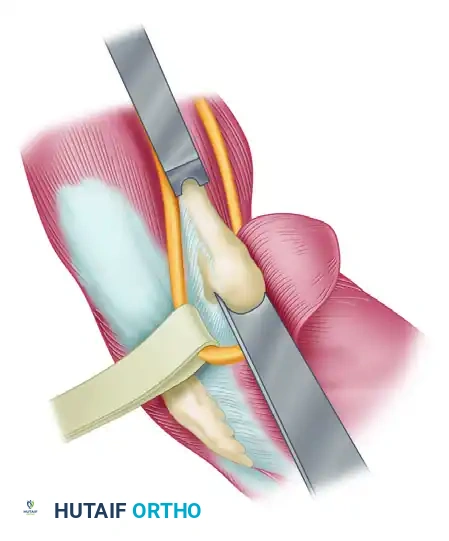
FIGURE 62-33B: The plane of the osteotomy aligns with the medial border of the trochlea. The sharp posterior edge of the osteotomy must be meticulously smoothed and rounded.
In addition to the epicondyle, remove a portion of the supracondylar ridge proximally to release the insertion of the medial intermuscular septum.
5. Proximal Release and Decompression
To ensure complete decompression, follow the ulnar nerve proximally. Expose and excise the medial intermuscular septum proximally up to the insertion of the coracobrachialis muscle. This step effectively releases the Arcade of Struthers, which is a frequent site of secondary compression, especially once the nerve shifts anteriorly following the epicondylectomy.
6. Bed Preparation and Soft Tissue Reconstruction
Following the osteotomy, the remaining bone will have sharp, raw cancellous edges. Using a bone rasp, aggressively smooth the osteotomy site. Ensure absolutely no bony ridges or spikes remain, as these will cause severe friction neuropathy when the nerve glides over the area.
Once the bone is smooth, reattach the periosteum and the deep fascia of the common flexor-pronator tendon over the osteotomy site. This step is critical: it separates the raw, bleeding cancellous bone surface from the ulnar nerve, preventing severe postoperative perineural fibrosis and tethering.
7. Nerve Relocation
Allow the ulnar nerve to seek its own position adjacent to the newly contoured medial humeral condyle. Because the bony prominence has been removed, the nerve will naturally translate anteriorly during elbow flexion without tension.
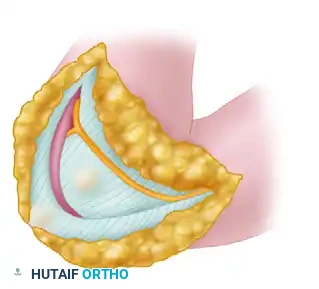
FIGURE 62-34D: The ulnar nerve has been allowed to transpose anteriorly into a tension-free environment following the removal of the medial epicondyle.
8. Hemostasis and Closure
Prior to closure, deflate the pneumatic tourniquet. Achieve meticulous hemostasis using bipolar electrocautery. The raw cancellous bone of the osteotomy site can bleed significantly; application of bone wax is generally avoided due to the risk of foreign body reaction near the nerve, but precise soft-tissue coverage usually tamponades the bleeding.
Irrigate the wound copiously with sterile saline. Close the subcutaneous tissues with interrupted absorbable sutures (e.g., 3-0 Vicryl), ensuring the MABC branches are not entrapped. Close the skin with a running subcuticular suture or interrupted nylon sutures based on surgeon preference.
Postoperative Care and Rehabilitation
The success of a medial epicondylectomy relies heavily on appropriate postoperative management to prevent stiffness and perineural scarring.
Phase 1: Immediate Postoperative (Days 1-10)
- Immobilization: The wound is protected in a soft, bulky compressive dressing. A posterior plaster splint may be applied with the elbow in 45 to 70 degrees of flexion to minimize tension on the wound and allow soft tissue healing.
- Edema Control: Strict elevation of the operative extremity above heart level.
- Digital ROM: Immediate active range of motion of the fingers and wrist is encouraged to prevent stiffness and promote nerve gliding.
Phase 2: Early Mobilization (Weeks 2-4)
- Suture Removal: Skin sutures are removed at 10 to 14 days.
- Range of Motion: The splint is discontinued. Early, active, and active-assisted range of motion of the elbow is allowed and progressed as tolerated.
- Nerve Gliding: Gentle ulnar nerve gliding exercises are initiated to prevent the nerve from adhering to the flexor-pronator fascial repair.
Phase 3: Strengthening (Weeks 4-8)
- Progressive Resistance: Once full, painless ROM is achieved, progressive strengthening of the flexor-pronator mass and elbow flexors/extensors begins.
- Return to Activity: Most patients can return to light duty by 4 weeks and heavy manual labor or unrestricted activities by 8 to 12 weeks, depending on the recovery of motor strength.
Complications and Avoidance Strategies
While medial epicondylectomy is highly successful, technical errors can lead to significant morbidity.
1. Valgus Instability
- Cause: Over-resection of the medial epicondyle, violating the sublime tubercle and the origin of the anterior bundle of the UCL.
- Prevention: Always use the medial border of the trochlea as the absolute lateral limit of the osteotomy. Angle the osteotome away from the joint line.
2. Recurrent Neuropathy / Nerve Tethering
- Cause: Failure to cover the raw cancellous bone of the osteotomy site, leading to severe perineural scarring; or failure to smooth sharp bony ridges.
- Prevention: Meticulously rasp the bone. Always repair the flexor-pronator fascia over the bone to create a smooth, soft-tissue gliding bed for the nerve.
3. Medial Antebrachial Cutaneous (MABC) Neuroma
- Cause: Iatrogenic transection or suture entrapment of the MABC branches during superficial dissection or closure.
- Prevention: Perform blunt dissection in the subcutaneous tissues. Identify and protect the nerve branches with vessel loops early in the procedure.
4. Flexor-Pronator Weakness
- Cause: Excessive detachment or failure to adequately repair the common flexor-pronator origin.
- Prevention: Elevate only the amount of tendon necessary to expose the epicondyle. Perform a robust repair of the fascial sleeve post-osteotomy.
Conclusion
Medial epicondylectomy is a powerful, anatomically sound procedure for the treatment of cubital tunnel syndrome. By converting the convex surface of the medial epicondyle into a flat, smooth plane, the surgeon eliminates the mechanical tension and friction on the ulnar nerve. Mastery of the local anatomy—specifically the relationship between the epicondyle, the ulnar collateral ligament, and the ulnar nerve—is essential for executing this procedure safely and achieving excellent long-term clinical outcomes.
📚 Medical References
- medial epicondylectomy combined with decompression for the treatment of cubital tunnel syndrome, J Hand Surg 25A:1043, 2000.
- Braga-Silva J: The use of silicone tubing in the late repair of the median and ulnar nerves in the forearm, J Hand Surg 24B:703, 1999.
- Childress HM: Recurrent ulnar nerve dislocation at the elbow, J Bone Joint Surg 38A:978, 1956.
- Childress HM: Recurrent ulnar nerve dislocation at the elbow, Clin Orthop Relat Res 108:168, 1975.
- Chow JA, Sunderland S, Van Beek AL: Surgical signifi cance of the motor fascicular group of the ulnar nerve in the forearm, J Hand Surg 9A:605, 1985.
- Craven PR Jr, Green DP: Cubital tunnel syndrome: treatment by medial epicondylectomy, J Bone Joint Surg 62A:986, 1980.
- Dellon AL: Review of treatment results for ulnar nerve entrapment at the elbow, J Hand Surg 14A:688, 1989.
- Dellon AL, Chang E, Coert JH, et al: Intraneural ulnar nerve pressure changes related to operative techniques for cubital tunnel decompression, J Hand Surg 19A:923, 1994.
- Eaton RG, Crowe JF, Parkes JC III: Anterior transposition of the ulnar nerve using a noncompressing fasciodermal sling, J Bone Joint Surg 62A:820, 1980.
- Escobar PL: Short segment stimulations in ulnar nerve lesions around elbow, Orthop Rev 12:65, 1983.
- Feindel W, Stratford J: The role of the cubital tunnel in tardy ulnar nerve palsy, Can J Surg 1:287, 1958.
- Gabel GT, Amadio PC: Reoperation for failed decompression of the ulnar nerve in the region of the elbow, J Bone Joint Surg 72A:213, 1990.
- Göbel F, Musgrave DS, Vardakas DG, et al: Minimal medial epicondylectomy and decompression for cubital tunnel syndrome, Clin Orthop Relat Res 393:228, 2001.
- Haase SC, Chung KC: Anterior interosseous nerve transfer to the motor branch of the ulnar nerve for high ulnar nerve injuries, Ann Plast Surg 49:285, 2002.
- Jones RE, Gauntt C: Medial epicondylectomy for ulnar nerve compression syndrome at the elbow, Clin Orthop Relat Res 139:174, 1979.
- Kato H, Hirayama T, Nimami A, et al: Cubital tunnel syndrome associated with medial elbow ganglia and osteoarthritis of the elbow, J Bone Joint Surg 84A:1413, 2002.
- Mackinnon SE, Novak CB, Myckatyn TM, et al: Results of reinnervation of the biceps and brachialis muscles with a
You Might Also Like