Surgical Approaches to the Elbow: Master Each Technique
Key Takeaway
Looking for accurate information on Surgical Approaches to the Elbow: Master Each Technique? Surgical approaches elbow are primarily divided into posterior, medial, and lateral methods, categorized by the deep surgical interval used. Posterior approaches include triceps-splitting and triceps-reflecting techniques, enabling exposure of the distal humerus and elbow joint. During these procedures, critical structures like the ulnar nerve are carefully visualized and protected to ensure patient safety and optimal outcomes.
Introduction and Epidemiology
The elbow is a highly constrained, complex hinge joint that presents unique challenges to the orthopedic surgeon. Surgical intervention around the elbow is indicated for a myriad of pathologies, ranging from complex intra-articular distal humerus fractures and terrible triad injuries to elective procedures such as total elbow arthroplasty and contracture release. The surgical exposures described for the elbow are broadly divided into posterior, medial, and lateral approaches. These descriptions denote the deep surgical interval employed rather than simply the cutaneous incision. Often, these deep approaches can be performed through a direct medial or lateral skin incision or a more versatile posterior midline incision, which allows access to both the medial and lateral columns by developing full-thickness fasciocutaneous flaps.
Epidemiologically, elbow trauma accounts for a significant portion of upper extremity injuries. Distal humerus fractures comprise approximately 2% of all adult fractures and 30% of elbow fractures. Radial head fractures are even more common, representing roughly one-third of all elbow fractures. The rising incidence of these injuries in both the young, high-energy trauma population and the elderly, osteoporotic population necessitates a thorough understanding of elbow surgical anatomy. Mastery of elbow approaches allows the surgeon to select the optimal window for fracture reduction, implant placement, or soft tissue reconstruction while minimizing iatrogenic injury to the dense neurovascular network surrounding the joint.
Surgical Anatomy and Biomechanics
A profound understanding of the osseous, ligamentous, and neurovascular anatomy of the elbow is the foundation of safe surgical exposure. The elbow joint comprises three distinct articulations: the ulnohumeral joint (a highly constrained hinge joint responsible for flexion and extension), the radiocapitellar joint, and the proximal radioulnar joint (which together facilitate forearm pronation and supination).
The distal humerus is formed by two columns (medial and lateral) that diverge from the humeral shaft, creating a triangular structure terminating in the articular segment. The medial column ends at the medial epicondyle, the origin of the flexor-pronator mass and the medial collateral ligament (MCL). The lateral column terminates at the lateral epicondyle, giving rise to the common extensor origin and the lateral collateral ligament (LCL) complex. The articular block consists of the trochlea medially and the capitellum laterally. The trochlea is spool-shaped and articulates with the greater sigmoid notch of the ulna, while the hemispherical capitellum articulates with the radial head.
Ligamentous stability is provided primarily by the MCL and the LCL complex. The anterior bundle of the MCL is the primary restraint to valgus stress and originates from the anterior inferior surface of the medial epicondyle, inserting onto the sublime tubercle of the coronoid. The LCL complex, specifically the lateral ulnar collateral ligament (LUCL), is the primary restraint to varus and posterolateral rotatory instability. It originates from the isometric point on the lateral epicondyle and inserts onto the supinator crest of the ulna.

Neurovascular anatomy dictates the safe zones and internervous planes of the elbow. The ulnar nerve courses posterior to the medial intermuscular septum, passing through the cubital tunnel behind the medial epicondyle before entering the forearm between the two heads of the flexor carpi ulnaris (FCU). The radial nerve spirals around the posterior humerus, pierces the lateral intermuscular septum, and courses anterior to the lateral epicondyle. It divides into the superficial sensory branch and the posterior interosseous nerve (PIN), which dives into the supinator muscle at the arcade of Frohse. The median nerve and brachial artery course anteriorly over the brachialis muscle, protected from posterior and lateral approaches but at risk during anterior capsular releases or when placing anterior hardware.
Indications and Contraindications
Selecting the appropriate surgical approach depends entirely on the pathology, the required visualization, and the planned fixation or reconstruction. Posterior approaches are the workhorse for distal humerus fractures, intra-articular nonunions, and total elbow arthroplasty. Lateral approaches are preferred for radial head and neck fractures, capitellum fractures, and LUCL reconstructions. Medial approaches are utilized for coronoid fractures, MCL reconstructions, and ulnar nerve transpositions.
| Pathology Category | Operative Indications | Non Operative Indications |
|---|---|---|
| Distal Humerus Fractures | Displaced intra-articular fractures, open fractures, vascular compromise, polytrauma | Nondisplaced fractures, severe dementia, non-ambulatory patients with prohibitive surgical risk |
| Radial Head Fractures | Mechanical block to rotation, >30% articular involvement, associated instability (terrible triad) | Isolated, nondisplaced or minimally displaced fractures (<2mm) with full active range of motion |
| Coronoid Fractures | Type II/III fractures with elbow instability, associated with terrible triad or varus posteromedial rotatory instability | Type I (tip) fractures in a stable joint, nondisplaced fractures with congruent joint on imaging |
| Elbow Stiffness | Functional deficit failing 6 months of conservative therapy, heterotopic ossification with mature bone | Active inflammatory phase, non-compliant patient, functional range of motion already present |
| Osteoarthritis / Rheumatoid | Severe pain and functional limitation, failed conservative management (Arthroplasty vs Interposition) | Mild to moderate symptoms, active infection, profound triceps insufficiency (relative contraindication) |
Contraindications to specific approaches are largely anatomical. For instance, a triceps-splitting approach may be contraindicated in a patient requiring a total elbow arthroplasty if a triceps-reflecting or triceps-sparing approach offers better extensor mechanism preservation. Similarly, lateral approaches utilizing the Kocher interval must be carefully considered if the patient has a known PIN palsy, to avoid further iatrogenic injury.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning involves advanced imaging, including orthogonal radiographs and computed tomography (CT) scans with 3D reconstructions for complex articular fractures. The CT scan is invaluable for understanding the comminution of the articular surface, particularly the presence of coronal shear fragments (capitellum/trochlea) and the exact morphology of coronoid fractures, which dictates whether a medial or lateral window is required.
Patient positioning is critical and must be tailored to the planned approach.

For posterior approaches, the lateral decubitus position is highly favored. The patient is placed in the lateral position with the operative arm supported over a padded post or an arm holder. This allows the elbow to flex past 90 degrees, utilizing gravity to help retract the triceps and providing excellent visualization of the articular surface. Alternatively, the prone position can be utilized, resting the arm on a short board, which also allows gravity-assisted elbow flexion.
For isolated lateral or medial approaches, the supine position is often adequate. The arm is placed on a radiolucent hand table. When utilizing a supine position for a medial approach, the shoulder is externally rotated, and the elbow is flexed. A sterile tourniquet is typically applied as high as possible on the brachium to maximize the surgical field. The limb is exsanguinated prior to tourniquet inflation unless there is an active infection or a malignant tumor.
Detailed Surgical Approach and Technique
Posterior Approaches to the Elbow
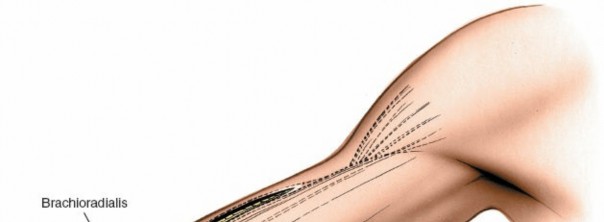
The universal posterior midline incision is the most versatile utility incision. It begins approximately 10 cm proximal to the olecranon, curves slightly laterally around the tip of the olecranon to avoid placing the scar directly over the bony prominence, and extends distally along the subcutaneous border of the ulna. Full-thickness fasciocutaneous flaps are elevated medially and laterally. The ulnar nerve must be identified early. It is located posterior to the medial epicondyle in the cubital tunnel. The nerve is decompressed by releasing the arcade of Struthers, the medial intermuscular septum, and the Osborne fascia. It is isolated with a vessel loop and protected throughout the procedure.
Releasing the triceps attachment to the olecranon directly is not advisable, owing to the difficulty of adequate repair and possible disruption during rehabilitation. Today, there are several choices of posterior exposure that manage the extensor mechanism differently.

Triceps Splitting Approach
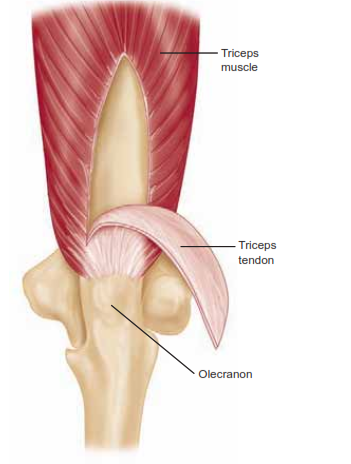
The triceps-splitting approach is excellent for extra-articular distal humerus fractures and simple intra-articular splits. The triceps tendon and muscle are split longitudinally in the midline, exposing the distal humerus. The anconeus is then reflected subperiosteally laterally, while the flexor carpi ulnaris is similarly retracted medially. The insertion of the triceps is carefully released from the olecranon, leaving the extensor mechanism in continuity with the forearm fascia and muscles medially and laterally. Closure of the triceps fascia is required only proximal to the olecranon, but the insertion should be repaired to the olecranon with a suture passed through the ulna via drill holes.
Triceps Splitting Tendon Reflecting Approach Van Gorder
A variation of the technique described earlier, the Van Gorder approach allows for lengthening of the triceps if necessary. A posterior midline incision begins 10 cm proximal to the olecranon and extends distally onto the subcutaneous border of the ulna between the anconeus and the flexor carpi ulnaris. The triceps fascia and aponeurosis are exposed along the tendinous insertion into the ulna. The tendon is reflected from the muscle in a proximal to distal direction, freeing the underlying muscle fibers while preserving the tendinous attachment to the olecranon. The triceps muscle is then split in the midline, and the distal humerus is exposed subperiosteally. The periosteum and triceps are elevated for a distance of about 5 cm proximal to the olecranon fossa, exposing the posterior aspect of the joint. The tendon slides distally from its initial position, and the proximal muscle and tendon are reapproximated in the lengthened relationship. This technique has been largely abandoned in favor of modern triceps-reflecting or osteotomy techniques due to extensor mechanism weakness.
Triceps Reflecting Approaches
The triceps mechanism may be preserved in continuity with the anconeus and simply reflected to one side or the other. Three primary surgical approaches have been described that preserve the triceps muscle and tendon in continuity with the distal musculature of the forearm fascia.
The Bryan-Morrey Posteromedial Triceps-Reflecting Approach was developed to preserve the continuity of the triceps with the anconeus and forearm fascia. The ulnar nerve is transposed. The medial aspect of the triceps is elevated from the medial intermuscular septum and posterior humerus. The dissection proceeds laterally, elevating the triceps tendon and anconeus subperiosteally off the olecranon as a continuous sleeve from medial to lateral. This provides excellent exposure for total elbow arthroplasty.
The Triceps Reflecting Anconeus Pedicle (TRAP) approach is an alternative that elevates the triceps and anconeus from distal to proximal. The interval between the anconeus and ECU is developed, and the anconeus is elevated off the ulna. The triceps is then sharply dissected off the olecranon, maintaining continuity with the anconeus.
Olecranon Osteotomy
For complex, highly comminuted intra-articular fractures (AO/OTA Type C), the transolecranon osteotomy remains the gold standard. After identifying and protecting the ulnar nerve, a chevron-shaped osteotomy is planned in the bare area of the greater sigmoid notch (approximately 2 cm from the olecranon tip). The osteotomy is pre-drilled for later repair. An oscillating saw is used to cut the dorsal cortex, and an osteotome is used to complete the articular cut to prevent thermal necrosis of the cartilage. The olecranon fragment with the attached triceps is reflected proximally, providing unparalleled visualization of the trochlea and capitellum.
Lateral Approaches to the Elbow
Lateral approaches are primarily utilized for access to the radiocapitellar joint and the lateral collateral ligament complex.
Kocher Approach
The Kocher approach utilizes the internervous plane between the anconeus (supplied by the radial nerve) and the extensor carpi ulnaris (supplied by the posterior interosseous nerve). The incision is made obliquely from the lateral epicondyle toward the ulnar styloid. The fascia is incised, and the interval between the anconeus and ECU is developed. The joint capsule is incised anterior to the equator of the radial head to avoid injury to the LUCL, which lies posterior to the equator. This approach provides excellent access to the radial head and neck.
Kaplan Approach
The Kaplan approach utilizes the internervous plane between the extensor digitorum communis (EDC) and the extensor carpi radialis brevis/longus (ECRB/ECRL). Both muscles are innervated by the radial nerve, making this an intermuscular, rather than internervous, plane. The incision extends distally from the lateral epicondyle toward the Lister tubercle. The fascial interval is split, exposing the joint capsule. The critical danger in this approach is the posterior interosseous nerve (PIN), which crosses the radial neck anteriorly within the supinator muscle. Dissection must not proceed distal to the annular ligament without identifying and protecting the PIN. The Kaplan approach offers a more anterior view of the radial head and capitellum compared to the Kocher approach.
Medial Approaches to the Elbow
Medial approaches are essential for addressing coronoid fractures, medial epicondyle fractures, and MCL injuries. The patient is positioned supine with the arm externally rotated.

Over the Top Approach Hotchkiss
The Hotchkiss modification of the medial approach provides access to the coronoid and anterior capsule. An incision is made over the medial epicondyle. The ulnar nerve is identified and protected. The flexor-pronator mass is split longitudinally in line with its fibers, typically between the pronator teres and the flexor carpi radialis, or by elevating the entire flexor-pronator mass off the medial epicondyle. The brachialis muscle is retracted anteriorly, exposing the anterior capsule and the coronoid process.
Flexor Carpi Ulnaris Split
For access to the sublime tubercle and the posterior aspect of the coronoid (such as in posteromedial rotatory instability patterns), a split through the two heads of the flexor carpi ulnaris (FCU) is utilized. The ulnar nerve is decompressed and retracted. The interval between the humeral and ulnar heads of the FCU is separated, providing direct access to the sublime tubercle for MCL repair or fixation of anteromedial facet coronoid fractures.
Complications and Management
Surgical approaches to the elbow are fraught with potential complications due to the high density of neurovascular structures and the joint's propensity for stiffness. Meticulous surgical technique and a thorough understanding of three-dimensional anatomy are paramount to minimizing these risks.
| Complication | Incidence | Etiology and Risk Factors | Salvage and Management Strategies |
|---|---|---|---|
| Ulnar Neuropathy | 5% - 15% | Traction injury, direct contusion, compression from hardware, scar tethering in the cubital tunnel. | Intraoperative protection. Subcutaneous or submuscular transposition if tension is noted. Postoperative neurolysis if symptoms persist and EMG confirms focal entrapment. |
| Posterior Interosseous Nerve (PIN) Palsy | 1% - 5% | Retractor placement distal to the radial neck during lateral approaches (Kaplan > Kocher). | Avoid placing retractors over the anterior radial neck. Pronate the forearm during lateral exposure to move the PIN anteriorly. Observation for neurapraxia; surgical exploration if transection is suspected. |
| Heterotopic Ossification (HO) | 10% - 20% | Severe trauma, delayed surgery, traumatic brain injury, forceful passive manipulation. | Prophylaxis with Indomethacin or localized radiation therapy in high-risk patients. Surgical excision of mature bone (typically 6 months post-injury) if functional ROM is limited. |
| Triceps Weakness / Avulsion | 2% - 8% | Failure of triceps repair after splitting, reflecting, or osteotomy approaches. Non-compliance with post-op restrictions. | Secure transosseous repair using heavy non-absorbable sutures (Krackow technique). Revision surgery with Achilles tendon allograft augmentation for chronic insufficiency. |
| Olecranon Osteotomy Nonunion | 2% - 5% | Inadequate fixation, thermal necrosis from saw blade, early aggressive active extension. | Use a chevron osteotomy to increase surface area. Fixation with tension band wiring or pre-contoured anatomic plates. Revision with bone grafting and rigid plate fixation. |
| Elbow Stiffness | 15% - 30% | Prolonged immobilization, capsular contracture, intra-articular adhesions. | Early active ROM within a stable arc. Static progressive splinting. Open or arthroscopic capsular release if conservative management fails after 6 months. |
Infection is a devastating complication, particularly after total elbow arthroplasty or complex trauma fixation. The subcutaneous nature of the posterior elbow makes it highly susceptible to wound breakdown. Meticulous handling of soft tissue flaps, avoiding excessive electrocautery on the skin edges, and closing the wound in multiple layers over a closed suction drain are critical steps to prevent deep surgical site infections.
Post Operative Rehabilitation Protocols
Rehabilitation following elbow surgery must balance the competing demands of tissue healing and the prevention of joint stiffness. The protocol is heavily dictated by the specific surgical approach utilized and the stability of the fracture fixation or ligamentous reconstruction.
Phase 1: Immediate Post-Operative (Weeks 0-2)
In the immediate postoperative period, the elbow is typically immobilized in a well-padded posterior splint. The position of immobilization depends on the pathology. For isolated lateral column procedures or radial head fixations, the elbow is splinted in 90 degrees of flexion with neutral rotation. If an LUCL repair was performed, the forearm is pronated to relax the lateral ligamentous complex. Conversely, if an MCL repair was performed via a medial approach, the forearm is supinated. If the triceps was detached and repaired (e.g., triceps-reflecting or olecranon osteotomy), active extension is strictly prohibited. However, gravity-assisted passive extension and active flexion are initiated as soon as pain allows, typically within 3 to 5 days, provided the fixation is rigid.
Phase 2: Intermediate ROM and Early Strengthening (Weeks 2-6)
Sutures are removed at 10 to 14 days. The patient is transitioned to a hinged elbow brace. Active and active-assisted range of motion exercises are emphasized. For triceps-sparing approaches, active extension can be progressed. For triceps-detaching approaches, active extension against gravity is avoided until 6 weeks to allow for tendon-to-bone or bone-to-bone healing. Static progressive splinting (turnbuckle splints) may be introduced at 4 to 6 weeks if the patient is failing to achieve functional range of motion (defined as a 100-degree arc from 30 degrees of extension to 130 degrees of flexion).
Phase 3: Strengthening and Return to Function (Weeks 6-12+)
Radiographic healing is typically assessed at 6 weeks. Once osseous union and soft tissue healing are confirmed, the hinged brace is discontinued. Progressive resistance exercises are initiated. Isometric strengthening transitions to isotonic and eventually isokinetic strengthening. Full return to heavy manual labor or contact sports is generally restricted until 4 to 6 months postoperatively, depending on the severity of the initial injury and the return of objective motor strength.
Summary of Key Literature and Guidelines
The evolution of elbow surgical approaches is well-documented in the orthopedic literature, with several landmark papers shaping current clinical practice.
The seminal work by Bryan and Morrey in the 1980s revolutionized posterior access to the elbow. Their description of the posteromedial triceps-reflecting approach provided a reproducible method for exposing the entire joint for total elbow arthroplasty while minimizing the risk of postoperative triceps insufficiency compared to older triceps-splitting techniques like the Van Gorder approach.
O'Driscoll's extensive research on elbow biomechanics and instability patterns fundamentally changed the approach to lateral elbow surgery. His detailed anatomical studies of the lateral ulnar collateral ligament (LUCL) emphasized the critical importance of preserving this structure during the Kocher approach, leading to the recommendation to stay anterior to the radial head equator during capsulotomy.
Jupiter and colleagues have contributed extensively to the management of complex distal humerus fractures. Their guidelines advocate for the transolecranon osteotomy for AO Type C3 fractures, demonstrating that orthogonal or parallel dual-plating techniques through an osteotomy provide the biomechanical stability necessary for early range of motion, which is the cornerstone of preventing postoperative stiffness.
Current guidelines from the American Academy of Orthopaedic Surgeons (AAOS) and the Orthopaedic Trauma Association (OTA) emphasize that the choice of surgical approach should be dictated by the fracture morphology identified on preoperative CT imaging. The trend in modern elbow surgery continues to shift toward triceps-sparing and internervous plane approaches whenever feasible, prioritizing early rehabilitation and the mitigation of iatrogenic morbidity.
You Might Also Like