
Applied Surgical Anatomy of the Deep Palmar Space
The palm is divided into spaces by fibrous septa that pass through it before attaching to the metacarpals. There are two major septa: The
thenar septum
originates from the palmar aponeurosis and inserts into the first metacarpal, separating the three muscles of the thenar eminence from the central palmar structures; and the
hypothenar septum
originates on the ulnar side of the palmar aponeurosis and inserts into the fifth metacarpal, separating the three muscles of the hypothenar eminence from the central palmar structures (see Figs. 5-41 and 5-79).
Thus, the palm is divided into three compartments: A thenar compartment, a hypothenar compartment, and a central compartment.
The central compartment contains the long flexor tendons to the fingers and the adductor pollicis muscle, as well as the digital nerves and vessels and the superficial and deep palmar arches.
Within the central compartment, a
potential deep space
exists between the undersurface of the flexor tendons and the upper surface of the interosseous and adductor pollicis muscles. This deep palmar space is divided into medial (midpalmar) and lateral (thenar) spaces by the
oblique septum
that arises from the connective tissue surrounding the middle finger flexor tendons and runs to the palmar surface of the middle metacarpal.44 This septum is the anatomic basis for the clinical division of deep palmar infection into two distinct, separate spaces.43
Lateral Space (Thenar Space)
The lateral space usually contains the first lumbrical muscle, which runs with the long flexor tendon to the index finger. Infections in the first web space may track down into the lateral space along the lumbrical muscle, although this is rare. Although lateral space infections may be drained through the first web space, such an incision is less effective than the procedure described in the previous section (see Figs. 5-84 to 5-87).
The space lies anterior to the adductor pollicis muscle. A second potential space exists behind that muscle and in front of the interossei. Infection of this “posterior adductor space” is very rare.45
Medial Space (Midpalmar Space)
The medial space contains the lumbrical muscles for the middle, ring, and little fingers, which run from the long flexor tendons of the middle, ring, and little fingers (the volar boundary of the space). The deep boundary is formed by the interossei and metacarpals of the third and fourth spaces. Thus, infection in the web spaces between the middle and ring fingers, and between the ring and little fingers, in theory, may spread to the medial space (see Fig. 5-79). The medial space may be drained through an incision in these webs, but the result is not as good as that obtained with direct drainage (see Figs. 5-80 to 5-83).
Drainage of the Radial Bursa
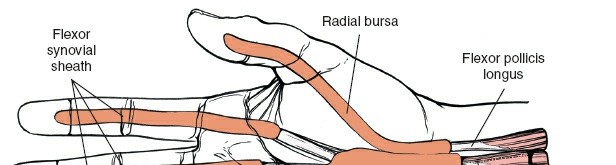
The long flexor tendon of the thumb is surrounded by a synovial sheath
that extends from the tendon’s insertion into the distal phalanx through the palm and carpal tunnel to the forearm just proximal to the proximal end of the flexor retinaculum. The proximal end of this sheath is known as the radial bursa (Fig. 5-88).
Infection of this space is diagnosed on the same clinical grounds as are infections of the synovial sheaths of the other fingers: Fusiform swelling of the thumb, with extreme pain on active or passive extension of the digit.
Position of the Patient
Place the patient supine on the operating table, with the arm on an arm board. A general anesthetic or an axillary or brachial block is essential. Use a nonexsanguinating tourniquet and have an excellent light source available (see Fig. 5-15).
Landmark and Incision
Landmark
The interphalangeal crease of the thumb is the surface marking for the interphalangeal joint of the thumb. It lies just proximal to the distal end of the fibrous flexor sheath of the thumb.
Incision
Two incisions are required for complete drainage. First, make a small longitudinal incision on the lateral side of the proximal phalanx of the thumb, just dorsal to the dorsal termination of the interphalangeal crease (Fig. 5-89). Then, make a second incision over the medial aspect of the thenar eminence (beware of the motor branch) or on the volar aspect of the wrist (the proximal end of the radial bursa).
Internervous Plane
There is no internervous plane in this approach. The skin incision in the finger lies between skin that is supplied by the dorsal digital nerves and skin that is supplied by the volar digital nerves.
Superficial Surgical Dissection
Deepen the wound in line with the first skin incision, remaining dorsal to the radial neurovascular bundle of the thumb. Identify the fibrous flexor sheath covering the flexor pollicis longus tendon and incise it
longitudinally, just proximal to the tendon’s insertion into the distal phalanx. Incise the synovium within the sheath to drain the pus.


Figure 5-88 Anatomy of the synovial sheaths of the fingers and the radial and ulnar bursae.


Figure 5-89 Incision for drainage of the radial bursa. Two incisions are required
for complete drainage. Distally, make a small longitudinal incision on the lateral side of the proximal phalanx of the thumb, just dorsal to the interphalangeal crease. Make a second incision over the medial aspect of the thenar eminence on the volar aspect of the wrist, and carry the incision proximally to the end of the radial bursa. Care must be taken to protect the median nerve and its motor branch to the thenar muscles.
Now, pass a probe proximally along the flexor sheath until the point of the probe can be felt on the volar aspect of the wrist. Make a small longitudinal skin incision over this point and dissect carefully down to the probe. The tip of the probe may be proximal to the proximal end of the flexor retinaculum, or it may be actually in the carpal tunnel itself. If it is in the carpal tunnel, then formally incise the flexor retinaculum, taking great care not to damage the underlying median nerve with its motor branch to the thenar eminence. This is the only situation in which the median nerve is approached necessarily from its radial aspect in the carpal tunnel.
As is the case in the treatment of tendon sheath infections, a small catheter may be left in the distal end of the flexor sheath to irrigate the flexor tendon (Fig. 5-90).
Dang
If the midlateral approach to the thumb is made too far in a volar direction, its radial neurovascular bundle may be incised accidentally.
Special Points
Do not cut blindly down on the tip of the probe at the wrist; the median nerve, the motor branch of the median nerve, or the palmar cutaneous branch of the median nerve may be cut (see Applied Surgical Anatomy of the Volar Aspect of the Wrist).
How to Enlarge the Approach
This approach cannot be enlarged effectively by either local or extensile measures.


Figure 5-90 Identify the fibrous flexor sheath covering the flexor pollicis longus tendon and incise it longitudinally just proximal to the tendon’s insertion into the distal phalanx. Incise the synovium in the sheath to drain the pus and then pass a probe proximally along the flexor sheath. Make a small longitudinal incision over the probe at the level of the wrist to ensure complete drainage.
Drainage of the Ulnar Bursa
The synovial sheath surrounding the flexor tendons to the little finger extends from the insertion of the profundus tendon on the distal phalanx of the little finger to the volar aspect of the wrist, just proximal to the proximal end of the flexor retinaculum. The flexor tendons to the index, middle, and ring fingers also are invested by this layer of synovium as they pass through the carpal tunnel. The distal extension of the synovial compartment ends at the origin of the lumbrical muscle from the tendons to the ring, middle, and index fingers. It is known as the ulnar bursa (see Fig. 5-88).
Infection of the synovial sheath of the little finger may lead to infection of the ulnar bursa. The physical signs include a tenosynovitis affecting the
little finger, with active or passive extension producing extreme pain. In addition, pain may be referred to the palm when the other fingers are extended.
Position of the Patient
Place the patient supine on the operating table, with the arm extended on an arm board. Use a nonexsanguinating tourniquet and either a general anesthetic or a proximal local block (an axillary or brachial block).
Landmark and Incision
Landmark
The distal interphalangeal crease of the little finger is the surface marking for the distal interphalangeal joint. It lies just proximal to the distal end of the fibrous sheath of the little finger.
Incision
Make a short midline incision on the ulnar side of the little finger over the distal end of the middle phalanx (Fig. 5-91,
inset
). The incision should be just dorsal to the line connecting the dorsal termination of the proximal and distal interphalangeal creases. Make a second longitudinal incision on the lateral aspect of the hypothenar eminence at the level of the wrist.
Internervous Plane
There is no internervous plane. The finger skin incision lies between skin that is supplied by the dorsal digital nerves and skin that is supplied by the volar digital nerves.
Superficial Surgical Dissection
Deepen the approach in line with the incision, staying to the dorsal side of the neurovascular bundle. Identify the fibrous flexor sheath and incise it longitudinally. Next, incise the synovium to allow drainage of the pus. Pass a probe gently along the tendon until it can be felt on the volar aspect of the wrist, just proximal to the proximal end of the flexor retinaculum.
Carefully incise the skin longitudinally over the probe and dissect down to it layer by layer. The probe should be just proximal to the proximal end of the flexor retinaculum. It may be in the carpal tunnel, however, in which case, the flexor retinaculum will have to be incised
meticulously, taking care to avoid damage to the underlying median nerve. If the probe is lying in the forearm, then take great care not to damage the ulnar nerve and artery, which are very close to the flexor digitorum superficialis tendon to the little finger (see Fig. 5-91).
As is true in the case of other tendon sheath infections, a small catheter may be inserted in the distal wound to allow continuous or intermittent irrigation of the tendon sheath.
Dang
The digital nerve to the ulnar side of the little finger is in danger if the skin incision on the finger is made too far in a volar direction. The distal vessels run with the nerves.
How to Enlarge the Approach
The approach cannot be enlarged effectively by either local or extensile measures.


Figure 5-91 Drainage of the ulnar bursa. Make a short midline incision on the ulnar side of the little finger over the distal end of the middle phalanx. Make a second longitudinal incision over the lateral aspect of the hypothenar eminence at the level of the wrist. Pass a probe from the distal aspect to the proximal aspect,
and cut down onto the probe at its proximal end, a point that marks the proximal end of the ulnar bursa.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding applied-surgical-anatomy-of-the-deep-palmar-space