Acute Ankle Fractures in Diabetic Patients: Advanced Surgical Management and Fixation Strategies
Key Takeaway
The operative management of acute ankle fractures in diabetic patients demands rigorous preoperative optimization and augmented surgical fixation. Due to the high risk of Charcot neuroarthropathy and wound complications, surgeons must employ robust constructs, including locking plates, multiple syndesmotic screws, and transarticular tibiotalar pinning. Postoperative protocols require extended immobilization and strict glycemic control to achieve a stable, plantigrade foot and prevent devastating morbidity or amputation.
ACUTE FRACTURES IN THE DIABETIC PATIENT
The management of acute ankle and foot fractures in patients with diabetes mellitus represents one of the most formidable challenges in orthopedic traumatology. Because operative treatment inherently carries higher complication rates in diabetic patients—especially those with compounding comorbidities such as peripheral arterial disease (PAD) and peripheral neuropathy—it is often tempting for the uninitiated surgeon to treat these fractures nonoperatively.
However, acute ankle fractures in diabetic patients must be approached with a strong bias toward operative fixation, utilizing principles similar to, but more robust than, those applied to nondiabetic patients. Nonoperative treatment in the neuropathic diabetic patient frequently leads to catastrophic loss of reduction, skin sloughing, ulceration, and the rapid onset of Charcot neuroarthropathy, ultimately resulting in a significantly higher rate of major limb amputation.
Clinical Pearl: The "diabetic paradox" in ankle trauma dictates that while surgery carries a high risk of wound complications and infection, nonoperative management carries a near-certainty of devastating mechanical failure and limb loss in the presence of neuropathy. Operative fixation is the definitive standard of care.
Preoperative Optimization and Risk Stratification
Before proceeding to the operating room, a rapid but thorough assessment of the patient's vascular and neurologic status is mandatory.
- Vascular Assessment: Palpable pulses do not rule out microvascular disease. Ankle-brachial indices (ABI) and toe-brachial indices (TBI) should be obtained if there is any clinical suspicion of ischemia. A TBI > 0.3 or a toe systolic pressure > 40 mm Hg is generally required for predictable wound healing.
- Neurologic Assessment: The presence of peripheral neuropathy (assessed via Semmes-Weinstein monofilament testing) fundamentally alters the biomechanical demands placed on the surgical construct. Neuropathic patients lack protective sensation and will inadvertently bear weight on the injured extremity, necessitating ultra-rigid fixation.
- Glycemic Control: Careful blood glucose control perioperatively can significantly decrease the incidence of surgical site infections and wound dehiscence. While long-term control (HbA1c) is a known predictor of complications, acute perioperative glucose management (maintaining levels between 140-180 mg/dL) is critical for acute fracture care.
BIOMECHANICS OF AUGMENTED FIXATION
Standard AO principles of internal fixation are frequently insufficient for the diabetic ankle. The combination of osteopenic bone, impaired cellular healing, and the patient's inability to offload the extremity demands augmented fixation techniques.
Principles of the Diabetic Construct
- Locking Plate Technology: Fixed-angle constructs are essential to prevent screw toggle and pullout in osteopenic bone.
- Increased Working Length: Plates should be longer than standard, utilizing more cortices proximal to the fracture to dissipate stress and prevent peri-implant fractures.
- Syndesmotic Augmentation: Even in the absence of frank syndesmotic instability, the syndesmosis in a diabetic patient should be stabilized with multiple (typically three or four) quadricortical screws to reinforce the mortise. These screws are generally not removed.
- Transarticular Fixation: In severe cases or highly noncompliant neuropathic patients, supplemental fixation with heavy Kirschner wires or Steinmann pins driven across the tibiotalar joint from the heel provides critical temporary stability.
SURGICAL APPROACHES AND TECHNIQUES
Standard Open Reduction and Internal Fixation (ORIF)
For the typical bimalleolar or trimalleolar equivalent fracture in a diabetic patient, a meticulous, soft-tissue-respecting approach is paramount.
Step 1: Positioning and Approach
The patient is positioned supine with a bump under the ipsilateral hip. A standard lateral approach to the fibula and a medial approach to the medial malleolus are utilized. Full-thickness fasciocutaneous flaps must be elevated without undermining the subcutaneous tissues to preserve the fragile microvascular supply.
Step 2: Fibular Fixation
The fibula is anatomically reduced. A long, lateral or posterolateral locking plate is applied. The plate should span significantly proximal to the fracture zone.
Step 3: Medial Malleolar Fixation
The medial malleolus is fixed using fully threaded, solid cortical screws or a medial buttress plate, as cancellous screws frequently fail to achieve adequate purchase in diabetic osteopenic bone.
Step 4: Syndesmotic and Transarticular Augmentation
Multiple syndesmotic screws are placed. If the construct feels tenuous, retrograde transarticular pins are driven from the plantar aspect of the calcaneus, through the talus, and into the distal tibia.
The following preoperative and postoperative radiographs demonstrate the successful application of augmented fixation in a young diabetic patient with a severe bimalleolar fracture-subluxation:


FIGURE 85-25 A and B: Preoperative radiographs of a highly unstable bimalleolar ankle fracture-subluxation in a 19-year-old man with a 12-year history of insulin-dependent diabetes mellitus.

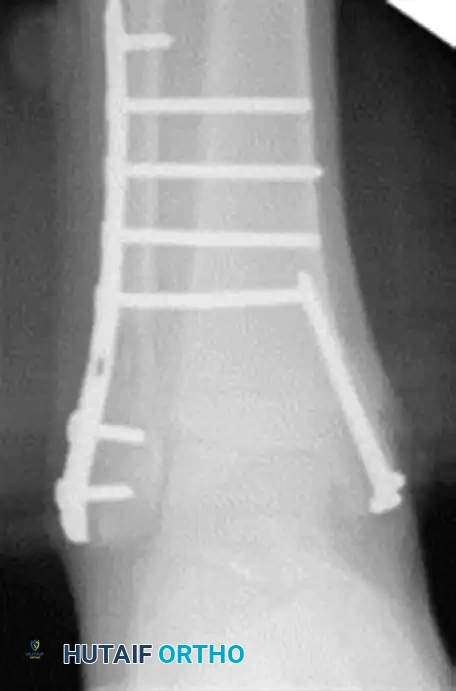
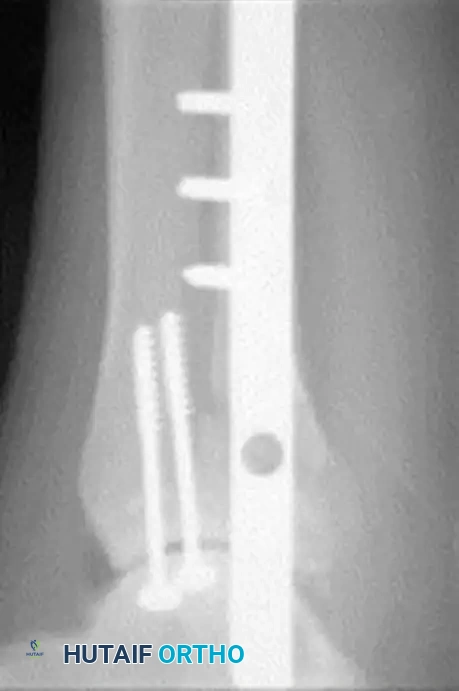
FIGURE 85-25 C-E: Postoperative fixation demonstrating robust fibular plating, medial malleolar screw fixation, and critical supplemental syndesmotic screws to reinforce the mortise.
Percutaneous Fixation Strategies
In patients with severe soft tissue compromise, massive fracture blisters, or profound vascular disease where open incisions carry an unacceptable risk of necrosis, percutaneous fixation may be considered. This technique relies on closed reduction and the strategic placement of percutaneous screws or transarticular pins. While it sacrifices anatomic reduction for soft tissue preservation, it provides the necessary stability to allow the soft tissue envelope to heal.



FIGURE 85-26 A-C: Percutaneous fixation of an ankle fracture in a diabetic patient, utilizing minimally invasive screw placement to stabilize the fracture while respecting a highly compromised soft tissue envelope.
MANAGEMENT OF CHARCOT NEUROARTHROPATHY
Acute fractures in diabetic patients can rapidly degenerate into Charcot neuroarthropathy if not rigidly stabilized. Conversely, patients may present with acute-on-chronic Charcot breakdown mimicking an acute fracture.
Surgical Warning: Misdiagnosing an acute Charcot event as a simple ankle sprain or standard fracture will lead to catastrophic joint destruction. Any diabetic patient presenting with a red, hot, swollen foot must be presumed to have Charcot arthropathy or deep infection until proven otherwise.
Tibiotalocalcaneal (TTC) Arthrodesis
When the ankle joint is unsalvageable due to severe Charcot destruction, realignment and extended fusion are required. A TTC arthrodesis utilizing a retrograde intramedullary nail provides a load-sharing construct that is biomechanically superior in the neuropathic patient.
Surgical Steps for TTC Nailing:
1. Preparation: The articular cartilage of the tibiotalar and subtalar joints is aggressively debrided down to bleeding subchondral bone.
2. Alignment: The foot is positioned in neutral dorsiflexion, 5 degrees of valgus, and 10 degrees of external rotation.
3. Implantation: A rigid retrograde intramedullary nail is introduced through the plantar aspect of the calcaneus, traversing the talus and into the tibial canal. Multiple locking screws are placed to secure the construct.

FIGURE 85-20 A and B: Severe Charcot arthropathy of the ankle with profound deformity and joint destruction.

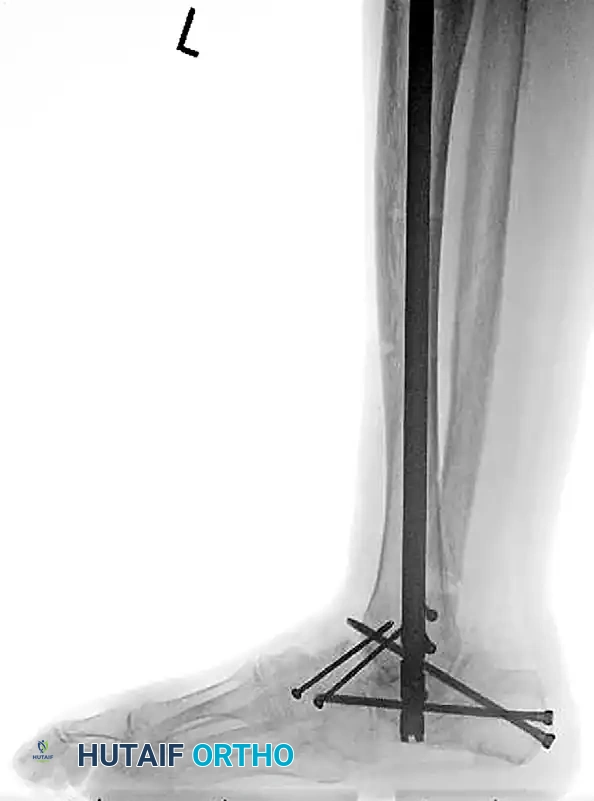
FIGURE 85-20 C and D: Postoperative radiographs following successful tibiotalocalcaneal (TTC) arthrodesis with a rigid retrograde intramedullary nail, restoring a plantigrade alignment.
Charcot Arthropathy with Superimposed Osteomyelitis
The presence of an open ulcer with underlying osteomyelitis in a Charcot ankle is a limb-threatening emergency. Internal fixation is strictly contraindicated in the setting of active infection.
Staged Reconstruction Protocol:
1. Radical Debridement: All infected bone and soft tissue must be excised. This frequently requires a complete talectomy if the talus is necrotic or heavily infected.
2. External Fixation: A hybrid or Ilizarov fine-wire external fixator is applied to span the defect, provide rigid stability, and allow for daily wound care and soft tissue reconstruction.


FIGURE 85-21 A and B: Charcot arthropathy of the ankle complicated by severe osteomyelitis.

FIGURE 85-21 C: Clinical appearance of the foot demonstrating a deep, probing medial ulcer.

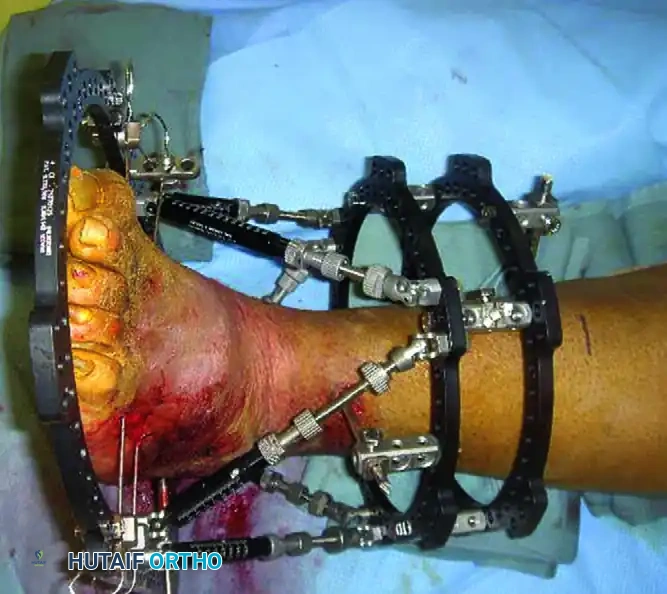
FIGURE 85-21 D and E: Intraoperative removal of the infected, necrotic talus (talectomy) to achieve source control.
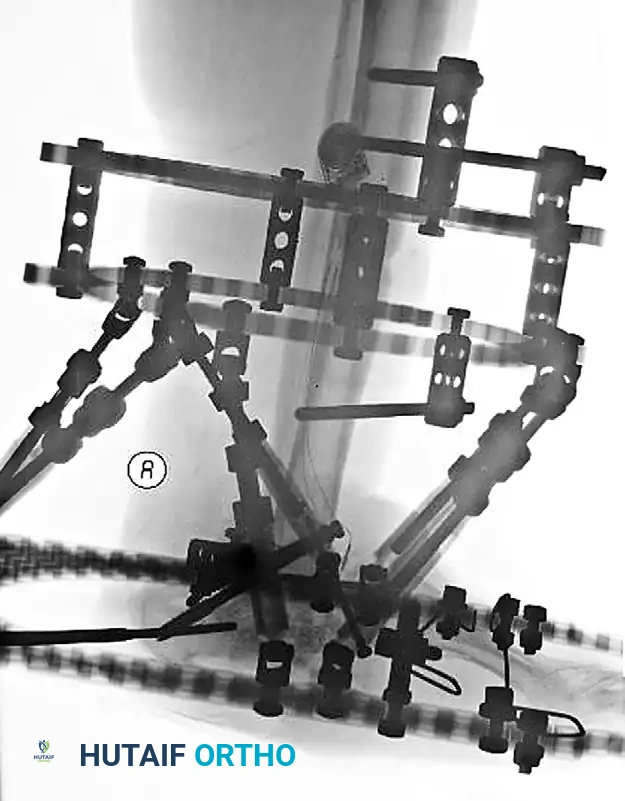
FIGURE 85-21 F: Application of a hybrid external fixator to stabilize the limb and maintain length following talectomy.

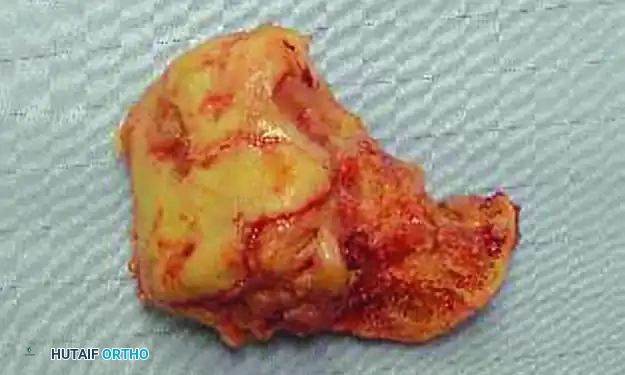
FIGURE 85-21 G and H: Postoperative radiographs showing the hybrid fixator in place, providing rigid stabilization while the soft tissue envelope heals.
Midfoot and Forefoot Charcot Reconstruction
Charcot breakdown is not limited to the ankle. Midfoot collapse (rocker-bottom deformity) and forefoot destruction are common. Surgical reconstruction in the midfoot often relies on the tension band principle. By placing a robust locking plate on the plantar surface of the midfoot, the hardware resists the immense tensile forces generated during the stance phase of gait.

FIGURE 85-22 A: Preoperative radiograph demonstrating severe Charcot arthropathy of the midfoot with classic rocker-bottom deformity.

FIGURE 85-22 B: Postoperative reconstruction utilizing a heavy plate on the plantar surface, taking advantage of the tension band principle to provide vastly stronger fixation.
Forefoot Charcot arthropathy similarly requires meticulous realignment and often extended fusions or resections to prevent recurrent ulceration beneath prominent metatarsal heads.


FIGURE 85-24 A and B: Radiographic examples of advanced Charcot arthropathy affecting the forefoot, requiring complex realignment to restore a braceable architecture.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of the diabetic patient is just as critical as the surgical execution. Standard rehabilitation timelines must be discarded.
- Extended Immobilization: Diabetic patients require significantly longer periods of immobilization. A minimum of 8 to 12 weeks of strict non-weight-bearing is standard, often double the time required for a healthy patient.
- Total Contact Casting (TCC): Once surgical incisions have healed, transitioning the patient to a Total Contact Cast is the gold standard for offloading the foot and preventing early hardware failure.
- Protected Weight-Bearing: When radiographic union is confirmed, the transition to weight-bearing must be gradual, utilizing a Charcot Restraint Orthotic Walker (CROW) boot or a custom-molded ankle-foot orthosis (AFO).
- Hardware Management: Transarticular pins are typically removed at 6 to 8 weeks in the clinic. Internal hardware (plates and syndesmotic screws) is left in place indefinitely unless it becomes prominent, symptomatic, or infected.
CONCLUSION
The treatment of diabetic patients with acute foot and ankle fractures or Charcot neuroarthropathy is exceptionally difficult, high-risk, and time-consuming. Thorough, documented explanations are required preoperatively so that patients and their families fully
You Might Also Like