Shoulder Amputations and Disarticulations: Operative Techniques
Key Takeaway
Shoulder amputations and disarticulations are profound salvage procedures primarily indicated for malignant neoplasms, severe trauma, or unsalvageable infections. This comprehensive guide details the precise surgical techniques for amputation through the surgical neck of the humerus and true shoulder disarticulation. Emphasizing meticulous neurovascular management, myodesis, and soft-tissue coverage, these protocols ensure optimal functional and cosmetic outcomes while minimizing postoperative complications such as phantom limb pain.
Introduction to Proximal Upper Extremity Amputations
Amputations at the level of the shoulder—encompassing both amputation through the surgical neck of the humerus and true glenohumeral disarticulation—are radical, life-altering procedures. In contemporary orthopedic practice, these surgeries are relatively rare, primarily reserved for scenarios where limb-sparing techniques are oncologically or anatomically impossible.
The loss of the upper extremity at this proximal level results in profound functional impairment and significant alteration of body image. Consequently, the surgical approach must be meticulously planned not only to eradicate disease or non-viable tissue but also to optimize the residual shoulder contour for cosmetic symmetry and potential prosthetic fitting.
Clinical Pearl: Few patients with shoulder-level amputations regularly utilize a functional, body-powered, or myoelectric prosthesis due to the extreme weight, high energy expenditure, and limited functional return. However, a well-contoured cosmetic shoulder cap is highly beneficial for restoring the silhouette of the shoulder girdle, aiding significantly in the patient's psychological rehabilitation and clothing fit.
Indications and Contraindications
Primary Indications
- Malignant Neoplasms: The most common indication. High-grade bone sarcomas (e.g., osteosarcoma, Ewing sarcoma) or massive soft-tissue sarcomas of the proximal arm that involve the neurovascular bundle or extensive muscular compartments, precluding negative margins with limb-salvage surgery.
- Severe Trauma: Irreparable crush injuries, massive avulsions, or traumatic amputations with extensive soft-tissue and neurovascular destruction.
- Arterial Insufficiency: End-stage, irreversible ischemia of the upper limb, though less common in the upper extremity compared to the lower extremity.
- Fulminant Infection: Uncontrollable necrotizing fasciitis, severe gas gangrene, or chronic, life-threatening osteomyelitis that is unresponsive to aggressive debridement and targeted antimicrobial therapy.
Contraindications
- Inadequate Proximal Margins: In oncologic cases, if tumor extension involves the scapula, clavicle, or chest wall, a forequarter amputation (interscapulothoracic amputation) is required rather than a shoulder disarticulation.
- Hemodynamic Instability: In trauma settings, damage control orthopedics may dictate a rapid guillotine amputation followed by formal revision once the patient is physiologically optimized.
Preoperative Planning and Anesthesia Considerations
Imaging and Templating
Advanced imaging, including MRI with contrast and CT angiography, is mandatory for oncologic and vascular indications to precisely delineate the extent of the pathology. The surgeon must determine preoperatively whether the surgical neck of the humerus can be safely preserved. Preserving the humeral head is vastly superior cosmetically, as it maintains the natural lateral prominence of the shoulder.
Management of Phantom Limb Pain
Phantom limb pain is notoriously common and severe following proximal upper extremity amputations.
Surgical Warning: The prevention of phantom limb pain begins preoperatively. It is best managed through a multidisciplinary approach. The utilization of continuous proximal nerve blocks (e.g., interscalene or supraclavicular catheters) placed by a skilled regional anesthesiologist prior to surgical incision is highly recommended to prevent central sensitization.
Surgical Anatomy of the Shoulder Girdle
A thorough understanding of the axillary anatomy is paramount. The neurovascular bundle, exiting the apex of the axilla, is invested in the axillary sheath.
* Arterial Supply: The axillary artery, divided into three parts by the pectoralis minor muscle, gives off critical branches including the thoracoacromial trunk, subscapular artery, and the anterior/posterior circumflex humeral arteries.
* Brachial Plexus: The cords of the brachial plexus surround the second part of the axillary artery. Precise identification of the median, ulnar, radial, and musculocutaneous nerves is required to prevent painful neuroma formation.
* Musculature: The deltoid provides the primary soft-tissue coverage. The pectoralis major, latissimus dorsi, and teres major act as powerful adductors and internal rotators that must be managed during myodesis.
Technique: Amputation Through the Surgical Neck of the Humerus
This technique is preferred when the proximal humerus is free of disease, as retaining the humeral head preserves the normal contour of the shoulder.
1. Patient Positioning
- Place the patient in a supine position.
- Place a sandbag or a radiolucent bump well beneath the affected shoulder, elevating the back to a 45-degree angle relative to the operating table. This allows circumferential access to the shoulder girdle and axilla.
- Drape the limb free to allow full manipulation during the procedure.
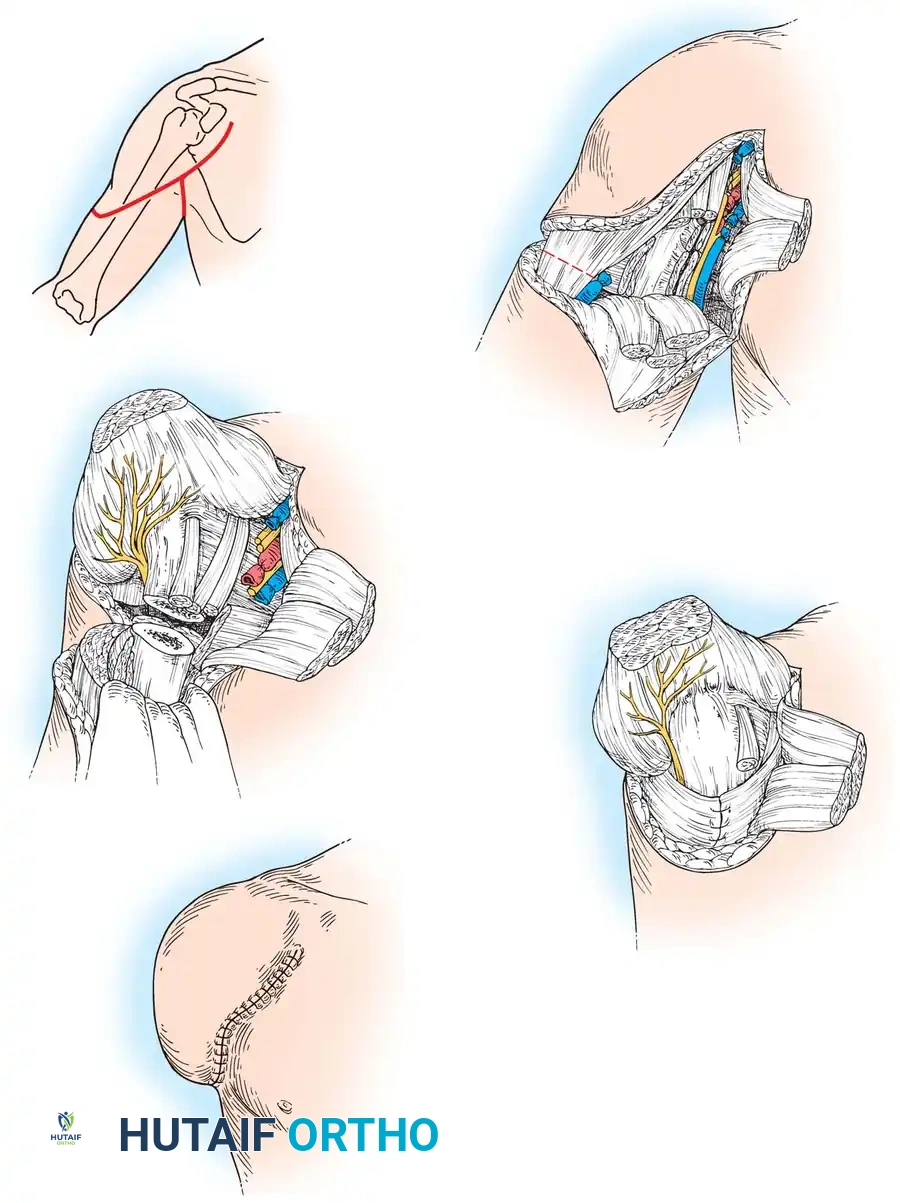
2. Incision and Flap Design
- Anterior Limb: Begin the skin incision anteriorly at the level of the coracoid process. Carry it distally along the anterior border of the deltoid muscle (following the deltopectoral groove) down to the deltoid insertion at the deltoid tuberosity.
- Posterior Limb: From the deltoid insertion, curve the incision superiorly along the posterior border of the deltoid muscle, terminating at the posterior axillary fold.
- Axillary Connection: Connect the anterior and posterior limbs with a second, transverse incision passing directly through the axilla.
- Note: The extent of the amputation and the design of these skin flaps must often be modified based on the zone of injury or tumor margins.
3. Superficial Dissection and Venous Control
- Identify the cephalic vein within the deltopectoral groove.
- Carefully isolate, ligate, and divide the cephalic vein to prevent troublesome bleeding during the deeper dissection.
- Separate the deltoid and pectoralis major muscles. Retract the deltoid muscle laterally to expose the deeper structures of the anterior shoulder.
4. Deep Dissection and Neurovascular Management
- Divide the pectoralis major muscle at its tendinous insertion on the lateral lip of the bicipital groove. Reflect the muscle belly medially.
- Develop the interval between the pectoralis minor and the coracobrachialis muscles to expose the main neurovascular bundle.
- Vascular Control: Isolate the axillary artery and axillary vein immediately inferior to the pectoralis minor. Doubly ligate these vessels with heavy non-absorbable suture (e.g., 0-Silk) and divide them.
- Nerve Management: Isolate the median, ulnar, radial, and musculocutaneous nerves.
- Crucial Step: Gently draw each nerve distally into the wound, apply gentle traction, and divide them sharply with a fresh scalpel blade. This allows the proximal nerve stumps to retract well proximal to the pectoralis minor, burying them deep within the soft tissues to minimize the risk of symptomatic neuroma formation.
5. Muscular Sectioning and Bone Resection
- Divide the deltoid muscle at its insertion on the humerus and reflect it superiorly, keeping it attached to the lateral skin flap to preserve its vascularity.
- Identify the teres major and latissimus dorsi muscles near their insertions at the medial lip and floor of the bicipital groove, respectively, and divide them.
- At a point exactly 1.9 cm distal to the intended level of the bone section, sever the long and short heads of the biceps, the triceps, and the coracobrachialis. Leaving this extra length is critical for the subsequent myodesis.
- Osteotomy: Section the humerus at the level of the surgical neck using an oscillating saw.
- Smooth the cut end of the humerus meticulously with a rasp to remove any sharp cortical edges that could compromise the overlying soft tissues or cause pain.
6. Myodesis and Closure
- Myodesis: Bring the sectioned ends of the long head of the triceps, both heads of the biceps, and the coracobrachialis over the smoothed end of the humerus. Suture them securely to the bone or to each other over the bone end to provide a robust soft-tissue cushion.
- Swing the previously reflected pectoralis major muscle laterally and suture it to the end of the bone, further reinforcing the distal coverage.
- Flap Tailoring: Drape the lateral skin flap and the underlying deltoid muscle over the reconstruction. Tailor the flap to allow accurate, tension-free apposition of the skin edges.
- Insert Penrose drains or closed-suction plastic tubes deep to the muscle layer and at the end of the bone to prevent hematoma formation.
- Close the skin edges with interrupted nonabsorbable sutures.
Technique: Disarticulation of the Shoulder
True disarticulation is indicated when the pathology extends to the proximal humerus, necessitating the complete removal of the bone while leaving the glenoid and scapula intact.
1. Patient Positioning and Incision
- Position the patient supine with a sandbag under the affected shoulder, elevating the back to a 45-degree angle, identical to the surgical neck amputation.
- The skin incision follows the exact same landmarks: beginning at the coracoid, extending distally along the anterior deltoid, curving up the posterior deltoid to the posterior axillary fold, and connecting through the axilla.
2. Anterior Dissection and Vascular Control
- Identify, ligate, and divide the cephalic vein in the deltopectoral groove.
- Separate the deltoid and pectoralis major; retract the deltoid laterally.
- Divide the pectoralis major at its insertion and reflect it medially.
- Develop the interval between the coracobrachialis and the short head of the biceps to expose the neurovascular bundle.
- Vascular Ligation: Isolate, doubly ligate, and divide the axillary artery and vein.
- Additional Step: In a disarticulation, identify the thoracoacromial artery, doubly ligate, and divide it. Allow the ligated vessels to retract superiorly beneath the pectoralis minor muscle.
3. Nerve Management
- Identify and isolate the median, ulnar, musculocutaneous, and radial nerves.
- Gently draw them inferiorly into the wound and divide them far proximally, ensuring they retract deeply beneath the pectoralis minor, well away from the future skin closure and potential prosthetic contact areas.
4. Muscular Release and Capsulotomy
- Divide the coracobrachialis and the short head of the biceps near their origins on the coracoid process.
- Free the deltoid muscle entirely from its insertion on the humerus and reflect it superiorly to expose the capsule of the glenohumeral joint.
- Divide the teres major and latissimus dorsi muscles near their insertions.
- Posterior Release: Place the arm in internal rotation. This maneuver exposes the short external rotator muscles (infraspinatus, teres minor) and the posterior aspect of the shoulder joint capsule. Divide all of these structures sequentially.
- Anterior Release: Place the arm in extreme external rotation. This exposes the anterior aspect of the joint capsule and the subscapularis muscle. Divide these structures to open the joint anteriorly.
- Section the triceps muscle near its origin/insertion, and divide the inferior capsule of the shoulder to completely sever the limb from the trunk.
5. Glenoid Management and Closure
- Filling the Defect: The removal of the humeral head leaves a significant cosmetic hollow. To mitigate this, reflect the cut ends of all available muscles (rotator cuff remnants, biceps, coracobrachialis) into the glenoid cavity. Suture them into the cavity to help fill the dead space.
- Acromioplasty: Inspect the acromion. Partially excise any unduly prominent acromion process using an oscillating saw or rongeur to give the residual shoulder a more smoothly rounded, natural contour.
- Carry the deltoid muscle flap inferiorly and suture it just inferior to the glenoid, securing it to the inferior capsular tissues or chest wall fascia.
- Insert closed-suction drains deep to the deltoid flap.
- Trim the skin flaps for an accurate, dog-ear-free fit, and close the edges with interrupted nonabsorbable sutures.
Postoperative Protocols and Rehabilitation
Immediate Postoperative Care
- Dressings: Apply a mildly compressive, soft dressing. Avoid excessive pressure that could compromise the vascularity of the skin flaps, particularly at the distal apex of the deltoid flap.
- Drain Management: Maintain closed-suction drainage until output is minimal (typically less than 30 cc over a 24-hour period) to prevent hematoma, which is a primary risk factor for deep infection and wound dehiscence.
- Analgesia: Continue regional anesthesia via indwelling catheters for 48 to 72 hours postoperatively. Transition to a multimodal oral pain regimen, heavily incorporating gabapentinoids (e.g., gabapentin or pregabalin) and SNRIs (e.g., duloxetine) to combat neuropathic and phantom limb pain.
Long-Term Rehabilitation
- Physical Therapy: Initiate early mobilization of the scapulothoracic articulation to prevent stiffness and maintain muscle tone in the remaining shoulder girdle. Posture training is critical, as the loss of limb weight often leads to an elevation of the ipsilateral shoulder and subsequent cervical/thoracic spine pain.
- Prosthetics: Once the surgical site is fully healed and edema has subsided (typically 6 to 8 weeks), refer the patient to a specialized prosthetist. While functional prostheses are challenging, the fabrication of a custom, lightweight cosmetic shoulder cap should be offered to restore the shoulder silhouette.
- Psychological Support: The psychological impact of a proximal amputation cannot be overstated. Routine integration of psychiatric or psychological counseling is a mandatory component of the holistic care pathway for these patients.
You Might Also Like