Hip Disarticulation and Hemipelvectomy: A Master Surgical Guide
Key Takeaway
Major lower extremity exarticulations, including hip disarticulation and hemipelvectomy, are radical salvage procedures reserved for advanced malignancies, severe trauma, or intractable infections. This guide details the complex surgical anatomy, precise operative techniques, and critical soft-tissue reconstruction strategies required for these life-saving interventions. Mastery of neurovascular control, osteotomy principles, and myocutaneous flap coverage is essential for minimizing morbidity and optimizing functional rehabilitation in this challenging patient population.
Introduction to Major Pelvic and Proximal Femoral Exarticulations
Major exarticulations of the lower extremity—specifically hip disarticulation and hemipelvectomy (hindquarter amputation)—are among the most radical and technically demanding procedures in operative orthopaedics. Historically developed for the curative and palliative treatment of malignant neoplasms, these procedures have evolved significantly. Pioneering work by surgeons such as Gordon-Taylor, Boyd, and Pack established the anatomical foundations, while modern advancements in soft-tissue reconstruction, neurovascular management, and postoperative prosthetics have dramatically improved patient survival and functional outcomes.
Today, these procedures are reserved for clinical scenarios where limb salvage is impossible or contraindicated. This comprehensive guide details the indications, surgical anatomy, step-by-step operative techniques, and postoperative rehabilitation protocols for both hip disarticulation and hemipelvectomy, synthesizing decades of evidence-based practice into a definitive masterclass for the orthopaedic surgeon.
Indications and Patient Selection
The decision to proceed with a hip disarticulation or hemipelvectomy is life-altering and requires a multidisciplinary approach involving orthopaedic oncologists, vascular surgeons, plastic surgeons, and rehabilitation specialists.
Oncologic Indications
The primary indication for these radical amputations remains malignant neoplasms of the bone and soft tissues.
* Primary Bone Sarcomas: Osteosarcoma, chondrosarcoma, or Ewing sarcoma of the proximal femur or pelvis that cannot be resected with negative margins via limb-sparing techniques.
* Soft Tissue Sarcomas: Massive, high-grade soft tissue sarcomas of the thigh or gluteal region involving major neurovascular bundles (e.g., the femoral or sciatic nerves).
* Palliative Exarticulation: In cases of fungating, painful, or bleeding tumors where the primary goal is to improve the quality of life rather than achieve a cure.
Non-Oncologic Indications
- Severe Infection: Necrotizing fasciitis extending into the pelvis, or chronic, intractable osteomyelitis of the proximal femur and acetabulum.
- Decubitus Ulcers: As highlighted by Chan et al., hemipelvectomy may be indicated as a salvage procedure for severe, life-threatening decubitus ulcers in paraplegic patients with previous spinal cord injuries.
- Peripheral Vascular Disease: End-stage ischemia with massive gangrene extending to the proximal thigh, where a transfemoral amputation would not yield viable tissue for closure.
- Trauma: Severe crush injuries or traumatic avulsions (e.g., "open book" pelvic fractures with unsalvageable neurovascular disruption).
Clinical Pearl: In patients with peripheral vascular disease, preoperative angiography or transcutaneous oxygen tension (TcPO2) mapping is critical. Salvage of a failed transfemoral amputation often requires a hip disarticulation to reach tissue with adequate perfusion for wound healing.
Surgical Anatomy and Biomechanics
A profound understanding of pelvic and proximal femoral anatomy is non-negotiable. The surgeon must navigate complex neurovascular networks and massive muscular compartments.
Vascular Anatomy
- Anterior Circulation: The external iliac artery transitions into the common femoral artery deep to the inguinal ligament. It branches into the superficial femoral and profunda femoris arteries.
- Posterior/Medial Circulation: The internal iliac artery supplies the gluteal region (superior and inferior gluteal arteries) and the medial thigh (obturator artery).
- Venous Plexus: The pelvic venous plexuses (presacral, perivesical) are thin-walled and highly susceptible to catastrophic hemorrhage during hemipelvectomy.
Neural Anatomy
- Lumbar Plexus: Gives rise to the femoral nerve (anterior thigh) and obturator nerve (medial thigh).
- Sacral Plexus: Gives rise to the sciatic nerve (L4-S3), which exits the pelvis via the greater sciatic foramen.
Surgical Warning: When transecting the sciatic nerve, it must be drawn distally, ligated securely, and allowed to retract deep into the pelvis to prevent the formation of a painful, superficial neuroma that would preclude prosthetic wear.
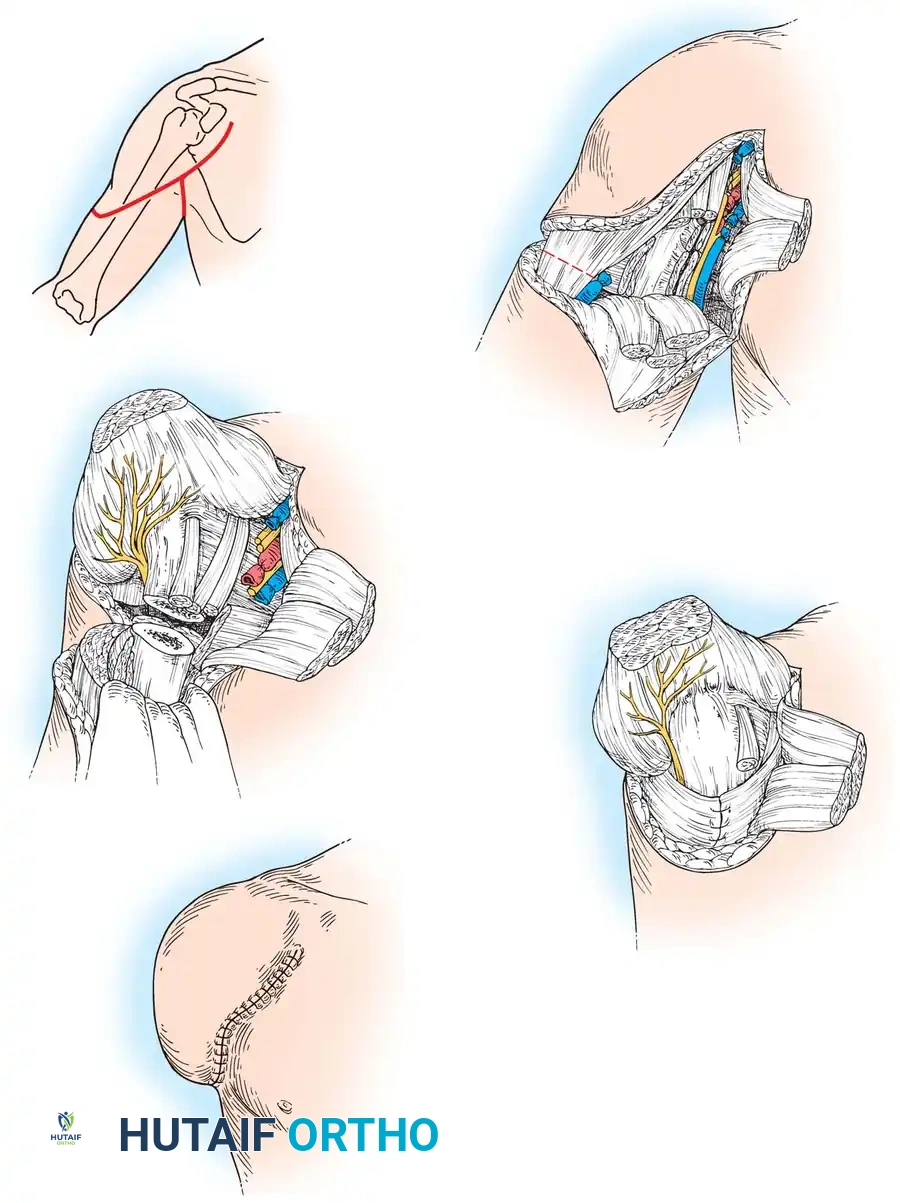
Hip Disarticulation: Operative Technique
Hip disarticulation involves the removal of the entire lower limb through the hip joint, preserving the pelvic ring. The classic approach utilizes an anterior racket incision, as popularized by Boyd.
1. Positioning and Preparation
- Position: The patient is placed in a lateral decubitus position or a "sloppy lateral" position, rolled 45 degrees away from the operative side. A beanbag is used for stabilization.
- Draping: The limb is draped free to allow for full manipulation during the procedure. The anus and genitalia are isolated with sterile adhesive drapes.
2. The Incision (Boyd's Racket Approach)
- The incision begins at the anterior superior iliac spine (ASIS), extends distally and medially parallel to the inguinal ligament, crosses the medial thigh 5 cm distal to the origin of the adductor muscles, continues across the posterior thigh 5 cm distal to the gluteal fold, and curves proximally to meet the starting point at the ASIS.
3. Anterior Dissection and Neurovascular Control
- The femoral triangle is exposed. The femoral sheath is opened.
- Ligation: The femoral artery is isolated, doubly ligated with heavy non-absorbable suture, and transected.
- Venous Control: The limb is elevated to exsanguinate it before ligating the femoral vein to preserve circulating blood volume.
- The femoral nerve is identified, placed under tension, sharply transected, and allowed to retract deep to the inguinal ligament.
4. Medial and Posterior Dissection
- The sartorius and rectus femoris are detached from the ASIS and AIIS, respectively.
- The pectineus and adductor muscle group are transected near their pubic origins. The obturator artery and nerve are identified and ligated.
- The limb is internally rotated. The short external rotators (piriformis, gemelli, obturator internus) are transected at their insertion on the greater trochanter.
- The gluteus maximus is elevated from its femoral insertion, preserving it as a large myocutaneous flap for closure.
- The sciatic nerve is identified, ligated, and transected sharply.
5. Capsulotomy and Disarticulation
- The hip capsule is incised circumferentially.
- The limb is forcefully externally rotated and abducted to dislocate the femoral head.
- The ligamentum teres is severed, and the remaining posterior capsular attachments are released, freeing the limb.
6. Closure and Myodesis
- Meticulous hemostasis is achieved. The acetabulum is inspected; the articular cartilage is typically left intact unless involved by disease.
- The massive gluteal flap is swung anteriorly and sutured to the origins of the pectineus and adductor muscles, creating a robust muscular cushion over the acetabulum.
- Closed suction drains are placed deep to the muscle layer.
- The skin is closed in a tension-free manner, resulting in a scar that lies anteriorly, away from the weight-bearing ischial tuberosity.
Hemipelvectomy (Hindquarter Amputation): Operative Technique
Hemipelvectomy (interinnominoabdominal amputation) involves the removal of the entire lower limb along with the ipsilateral hemipelvis. It is a massive physiological insult requiring meticulous surgical orchestration.
1. Positioning and Incision
- Position: True lateral decubitus position.
- Incision (Gordon-Taylor Approach): The anterior limb of the incision follows the iliac crest from the posterior superior iliac spine (PSIS) to the ASIS, then runs parallel to the inguinal ligament to the pubic tubercle. The posterior limb drops from the PSIS, follows the greater sciatic notch, and sweeps across the gluteal fold to meet the anterior incision at the perineum.
2. Abdominal Exploration and Vascular Control
- The abdominal wall musculature is detached from the iliac crest. The peritoneum is bluntly swept medially to expose the retroperitoneal space.
- The ureter is identified and protected.
- The common iliac artery and vein are exposed.
- Temporary Ligation: As described by Lazzari and Rack, temporary clamping of the common iliac artery can be utilized to minimize blood loss during the posterior dissection. Ultimately, the external iliac artery and vein (or common iliac, depending on tumor extent) are doubly ligated and divided.
Pitfall: Tearing the internal iliac vein or the presacral venous plexus can result in massive, uncontrollable hemorrhage. Dissection in the retroperitoneal space must be strictly blunt and meticulous.
3. Anterior Osteotomy (Symphysis Pubis)
- The spermatic cord or round ligament is retracted.
- The rectus abdominis is detached from the pubis.
- The symphysis pubis is divided using a Gigli saw, osteotome, or heavy scalpel (in younger patients with a cartilaginous symphysis).
4. Posterior Osteotomy (Sacroiliac Joint)
- The patient is rolled slightly forward. The posterior flap (gluteus maximus) is elevated if it is free of tumor. If the tumor involves the buttock, an anterior flap (quadriceps) must be designed.
- The iliolumbar ligaments are divided.
- The sacroiliac joint is opened anteriorly, or a transiliac osteotomy is performed using a Gigli saw or osteotome just lateral to the SI joint, depending on oncologic margins.
5. Specimen Delivery
- The hemipelvis is hinged outward. The sacral nerve roots (L4, L5, S1-S3) forming the sciatic nerve are identified, ligated, and transected.
- The levator ani is divided near its pelvic attachment.
- The remaining soft tissues are severed, and the specimen is delivered.
6. Soft Tissue Reconstruction and Flap Coverage
- Flap Selection: The standard closure utilizes a posterior gluteal myocutaneous flap. However, if the gluteus is resected, alternative flaps are required.
- Advanced Flaps: Luna-Perez and Herrera described the use of a medial thigh myocutaneous flap. In extreme cases, a fillet flap from the amputated limb (harvesting healthy tissue distal to the tumor) can be utilized as a free flap to cover the massive defect, as described by Sara et al.
- The flap is sutured to the abdominal wall musculature (obliques and transversus abdominis) to prevent visceral herniation.
- Multiple large-bore drains are placed.
Postoperative Management and Rehabilitation
The postoperative phase following major exarticulation is fraught with physiological and psychological challenges.
1. Immediate Postoperative Care
- Hemodynamic Monitoring: Patients require ICU admission for aggressive fluid resuscitation and monitoring for occult hemorrhage.
- Wound Care: The massive flaps are at high risk for necrosis. Avoid pressure on the flap. The patient should be nursed on a pressure-relieving mattress and repositioned frequently.
- DVT Prophylaxis: Due to the extensive pelvic dissection and altered venous return, patients are at extreme risk for deep vein thrombosis and pulmonary embolism. Chemical prophylaxis is initiated as soon as surgical hemostasis is assured.
2. Pain Management
- Phantom Limb Pain: Nearly all patients experience phantom limb sensation, and a significant percentage develop phantom limb pain. Multimodal analgesia, including gabapentinoids, tricyclic antidepressants, and regional nerve blocks (e.g., continuous epidural or perineural catheters placed intraoperatively), is essential.
3. Prosthetic Rehabilitation
- Rehabilitation begins immediately. The principles of immediate postsurgical prosthetics, championed by Burgess et al., emphasize early mobilization to improve psychological well-being and reduce deconditioning.
- Hip Disarticulation Prosthesis: Utilizes a Canadian-style socket that captures the ischial tuberosity and iliac crest for suspension.
- Hemipelvectomy Prosthesis: Highly complex, requiring a socket that encases the lower thorax and remaining abdomen for suspension, as the ischial weight-bearing surface is absent. Weight is transferred through the soft tissues of the abdominal wall and the contralateral hemipelvis.
- As noted by Dénes and Till, successful rehabilitation depends heavily on the patient's preoperative cardiovascular fitness, core strength, and motivation. Many older patients or those with severe comorbidities may ultimately choose to mobilize via a wheelchair rather than expend the massive energy required for prosthetic ambulation.
Complications and Salvage Strategies
- Flap Necrosis: Marginal necrosis is common. It is managed with aggressive debridement. If deep infection occurs, vacuum-assisted closure (VAC) therapy and secondary skin grafting or rotational flaps are required.
- Infection: The proximity of the incision to the perineum increases the risk of fecal contamination. Preoperative bowel preparation and diverting colostomy (in highly selected cases of massive perineal involvement) may be considered.
- Herniation: Failure to securely anchor the myocutaneous flap to the abdominal fascia can result in a perineal or abdominal hernia, requiring synthetic mesh reconstruction.
Conclusion
Hip disarticulation and hemipelvectomy remain formidable procedures in the orthopaedic armamentarium. While the anatomical loss is profound, meticulous adherence to surgical principles—precise neurovascular control, oncologically sound osteotomies, and robust soft-tissue reconstruction—can yield life-saving outcomes. As surgical techniques and prosthetic technologies continue to advance, the focus remains not only on maximizing survival but on restoring dignity, mobility, and quality of life to this highly vulnerable patient population.
📚 Medical References
You Might Also Like