Major Lower Extremity Amputations: Principles, Techniques, and Outcomes
Key Takeaway
Major lower extremity amputations require meticulous surgical technique and precise level selection to optimize functional outcomes and prosthetic fitting. This comprehensive guide details the evidence-based indications, biomechanical considerations, and step-by-step surgical approaches for transtibial amputations, knee disarticulations, and transfemoral amputations. By integrating advanced perfusion assessment with meticulous soft-tissue handling, orthopedic surgeons can maximize wound healing, minimize complications, and facilitate successful postoperative rehabilitation for patients with severe ischemia, trauma, or infection.
Introduction and Epidemiology
Major lower extremity amputation remains a profound, life-altering intervention, primarily indicated for end-stage peripheral vascular disease (PVD), severe diabetic neuropathy with unsalvageable infection, devastating trauma, and malignant neoplasms. According to epidemiological data from the Centers for Disease Control (CDC) and the Amputee Coalition, dysvascular etiology accounts for the vast majority of lower limb amputations in the developed world.
The primary goal of amputation surgery is no longer merely the ablation of diseased or non-viable tissue; it is the reconstructive creation of a dynamic, sensate, and durable residual limb capable of interfacing seamlessly with a modern prosthesis. The orthopedic surgeon must balance the necessity of achieving primary wound healing with the biomechanical imperative of preserving maximal limb length and joint function.
Preoperative Assessment and Level Selection
The determination of the optimal amputation level is arguably the most critical preoperative decision. A level chosen too distally in an ischemic limb invites wound failure, necrosis, and the morbidity of revision surgery. Conversely, an unnecessarily proximal amputation drastically increases the metabolic cost of ambulation and decreases the likelihood of successful prosthetic rehabilitation.
Clinical Evaluation
Clinical assessment of tissue viability relies on skin temperature, capillary refill, the presence of dependent rubor, and the quality of palpable pulses. However, clinical judgment alone is notoriously inaccurate in predicting wound healing in dysvascular patients, necessitating objective physiological testing.
Objective Perfusion Assessment
Evidence-based practice mandates the use of objective hemodynamic parameters to guide level selection:
- Transcutaneous Oxygen Tension (TcPO2): The gold standard for predicting amputation wound healing. A TcPO2 > 30 mm Hg is generally associated with successful primary healing. Values < 20 mm Hg indicate severe ischemia, and primary healing at this level is highly unlikely without prior revascularization.
- Doppler Ultrasound and Segmental Pressures: Ankle-brachial indices (ABI) can be falsely elevated in diabetic patients due to medial arterial calcification (Mönckeberg's sclerosis). However, an absolute calf pressure > 70 mm Hg or an ankle pressure > 50 mm Hg suggests adequate perfusion for a transtibial amputation.
- Skin Perfusion Pressure (SPP): Utilizing photoelectric measurements or laser Doppler, an SPP > 30 mm Hg correlates strongly with successful healing.
- Fluorescein Angiography and Xenon-133 Clearance: While historically significant for mapping skin viability and capillary blood flow, these modalities have largely been superseded by TcPO2 and SPP in contemporary practice due to logistical constraints.
Clinical Pearl: Never rely solely on a single vascular parameter. Synthesize TcPO2, Doppler waveforms, and clinical examination. In borderline cases, intraoperative assessment of muscle viability (color, consistency, contractility, and capacity to bleed) remains the ultimate arbiter of the amputation level.
Transtibial Amputation (Below-Knee Amputation)
The transtibial amputation (TTA) is the workhorse of major lower extremity amputations. Preservation of the anatomical knee joint is paramount; it reduces the energy expenditure of ambulation by 40% compared to a transfemoral amputation and dramatically improves proprioception and functional independence.
Indications and Biomechanics
TTA is indicated for unsalvageable foot and ankle pathology where adequate perfusion exists at the mid-calf level. Biomechanically, the ideal residual tibia length is between 12 and 15 cm from the medial joint line. Stumps shorter than 5 cm lack the lever arm required for knee extension and are prone to flexion contractures, while excessively long stumps suffer from poor distal soft-tissue coverage and vascularity.
Surgical Approaches and Flap Design
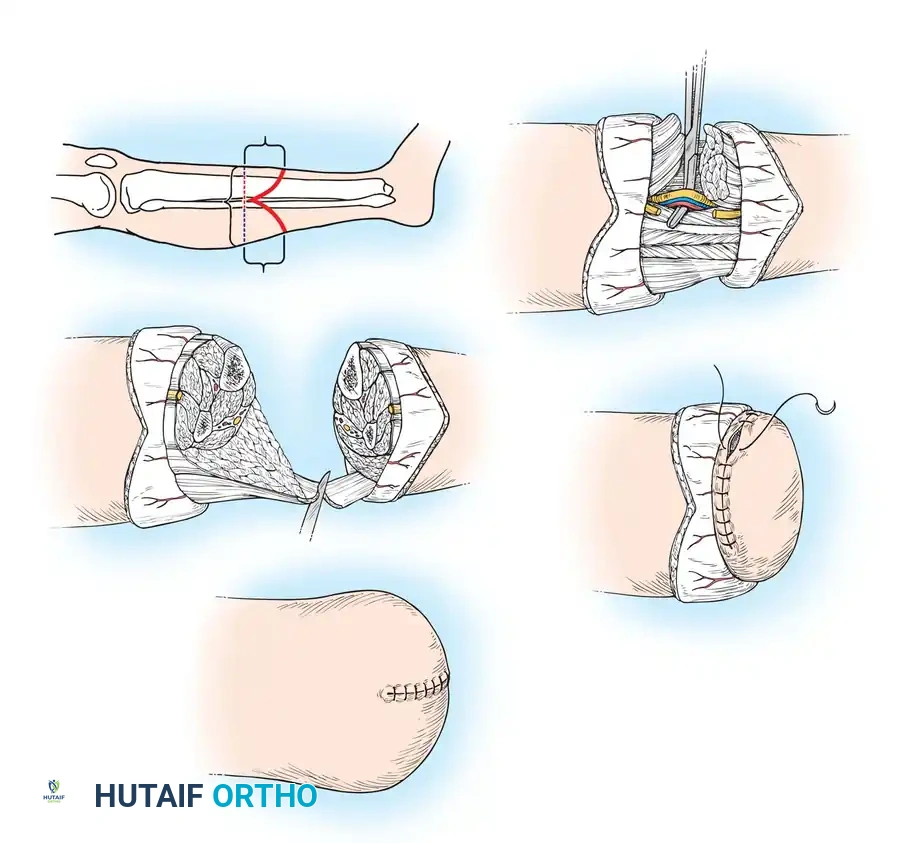
1. The Burgess Long Posterior Flap
Pioneered by Ernest Burgess, the long posterior myofasciocutaneous flap is the standard of care for dysvascular patients. The posterior calf tissues (gastrocnemius and soleus) have a robust collateral blood supply from the sural arteries, making this flap highly resilient to ischemia.
Step-by-Step Technique:
1. Incision: Outline an anterior transverse incision at the desired level of bone transection (typically 12-15 cm distal to the joint line). Extend the incision distally along the mid-medial and mid-lateral axes of the leg to create a posterior flap that is 1 cm longer than the anterior-posterior diameter of the calf.
2. Anterior Dissection: Deepen the anterior incision through the deep fascia. Identify and ligate the anterior tibial artery and vein. Transect the anterior compartment musculature and the deep peroneal nerve (which should be drawn distally, sharply transected, and allowed to retract deep into the muscle belly to prevent neuroma formation).
3. Bone Transection: Clear the periosteum circumferentially at the osteotomy site. Transect the tibia with an oscillating saw.
4. Tibial Beveling: Create a 45-degree anterior bevel on the distal tibia to prevent the sharp anterior crest from eroding through the anterior skin flap. Smooth the edges meticulously with a rasp.
5. Fibular Osteotomy: Transect the fibula 1.5 to 2 cm proximal to the tibial cut. Bevel the lateral border to prevent prominence.
6. Posterior Flap Creation: Dissect the posterior flap from proximal to distal. Ligate the posterior tibial and peroneal vessels. The soleus muscle, which is often poorly vascularized and bulky, is typically excised, leaving the highly vascular gastrocnemius to form the muscle cushion.
7. Myodesis: Bring the posterior gastrocnemius flap anteriorly and secure it to the anterior tibial fascia and periosteum via drill holes in the anterior tibia. This tension myodesis stabilizes the muscle, prevents distal bone prominence, and provides a robust distal cushion.
Surgical Warning: Avoid excessive periosteal stripping of the tibia. Stripping devascularizes the bone, leading to ring sequestrum formation, chronic osteomyelitis, and delayed wound healing.
2. Alternative Flap Techniques
- Sagittal Flaps (Persson Technique): Equal medial and lateral flaps are useful in non-dysvascular patients or when posterior skin is compromised. It provides excellent contour but relies on the less robust anterior blood supply.
- Skew Flap (Robinson Technique): An anteromedial and posterolateral flap design that places the scar away from bony prominences and utilizes the collateral circulation effectively.
- Ertl Osteomyoplastic Reconstruction: Involves creating a synostosis (bone bridge) between the distal tibia and fibula using a periosteal sleeve or bone graft. This creates a broad, end-bearing residual limb and prevents fibular hypermobility. It is highly recommended for young, active trauma patients but is generally contraindicated in severe dysvascular disease due to the extensive dissection required.
Knee Disarticulation (Through-Knee Amputation)
Knee disarticulation (KD) is an often-underutilized procedure that offers distinct biomechanical advantages over transfemoral amputation, particularly for non-ambulatory patients or those with severe trauma.
Indications and Biomechanics
KD is indicated when a transtibial amputation is impossible due to proximal trauma, tumor, or ischemia, but the distal femoral soft tissues are viable.
Advantages:
* Provides a broad, end-bearing stump (the femoral condyles).
* Maintains the full length of the femoral lever arm, maximizing mechanical advantage.
* Preserves the adductor magnus insertion, preventing the abduction contracture commonly seen in transfemoral amputations.
* In pediatric patients, it preserves the distal femoral physis, allowing for continued longitudinal bone growth and preventing terminal bony overgrowth.
Disadvantages:
* The resulting stump is bulbous, which can create cosmetic challenges with prosthetic fitting.
* The prosthetic knee joint must be placed distal to the anatomical knee center, leading to an asymmetrical sitting appearance.
Surgical Approach
- Incision: Classic approaches utilize equal anterior and posterior flaps (fish-mouth) or equal sagittal flaps. The anterior flap should be left long enough to cover the femoral condyles without tension.
- Dissection: Deepen the incision to the joint capsule. Detach the patellar tendon from the tibial tubercle.
- Joint Disarticulation: Incise the anterior capsule and enter the joint. Transect the anterior and posterior cruciate ligaments at their tibial insertions. Divide the medial and lateral collateral ligaments.
- Neurovascular Management: Identify the popliteal artery and vein in the posterior aspect of the joint; doubly ligate and transect them. Identify the tibial and common peroneal nerves, draw them distally, ligate them to prevent bleeding from the vasa nervorum, and transect them sharply so they retract deep into the thigh musculature.
- Patellar Management: The patella is typically retained to provide an anterior bony shield and maintain the quadriceps mechanism.
- Myodesis/Myoplasty: Suture the patellar tendon to the remnants of the cruciate ligaments in the intercondylar notch. Bring the hamstrings forward and suture them to the patellar tendon and joint capsule to balance flexion and extension forces.
Pitfall: Failure to securely anchor the patellar tendon to the cruciate ligaments will result in proximal migration of the patella, loss of the anterior soft-tissue shield, and a poorly functioning quadriceps mechanism.
Transfemoral Amputation (Above-Knee Amputation)
Transfemoral amputation (TFA) results in the loss of the anatomical knee joint, increasing the metabolic cost of ambulation by up to 100%. Consequently, meticulous surgical technique is required to optimize the remaining biomechanical levers to facilitate prosthetic use.
Indications and Biomechanics
TFA is indicated for massive lower extremity trauma, proximal tumors, overwhelming necrotizing infections, or severe PVD where perfusion is inadequate for a more distal amputation.
The critical biomechanical challenge in TFA is the loss of the adductor magnus insertion. If the adductors are not surgically reattached, the unopposed hip abductors (gluteus medius and minimus) will drive the femur into a severe abduction contracture. This malalignment prevents the femur from loading the lateral wall of the prosthetic socket, leading to a Trendelenburg gait and massive energy inefficiency.
Surgical Approach and the Gottschalk Principles
Gottschalk revolutionized the TFA by emphasizing the absolute necessity of an adductor myodesis to maintain the femur in its anatomical adducted position.
- Incision: A fish-mouth incision is standard, with the anterior and posterior flaps meeting at the mid-medial and mid-lateral lines. The flaps must be long enough to close without tension over the transected femur.
- Vascular Control: Isolate, doubly ligate, and transect the superficial femoral artery and vein within the adductor canal.
- Nerve Management: Identify the sciatic nerve. It is critical to ligate the nerve prior to transection to control the robust vasa nervorum. Transect the nerve high under tension so it retracts deep beneath the gluteal musculature, away from the distal weight-bearing surface.
- Femoral Osteotomy: Transect the femur at the desired level (ideally preserving at least 50% of femoral length). Smooth the distal edges with a rasp.
- Adductor Myodesis (Critical Step): Drill multiple osseous holes through the distal lateral femur. Advance the adductor magnus tendon across the distal end of the femur and suture it securely through these drill holes while holding the femur in maximum adduction. This restores the adductor moment arm.
- Quadriceps and Hamstring Myoplasty: Bring the quadriceps fascia over the distal femur and suture it to the posterior fascia of the hamstrings, creating a stable, balanced muscular envelope over the bone end.
Postoperative Protocols and Rehabilitation
The immediate postoperative phase is focused on edema control, wound healing, and contracture prevention.
- Rigid Dressings: The application of an immediate postoperative rigid dressing (IPORD) or a plaster-pylon technique protects the wound from trauma, significantly reduces edema, and accelerates maturation of the residual limb.
- Contracture Prevention: For TTA, the knee must be maintained in extension using a posterior splint or rigid dressing. For TFA, patients must avoid prolonged sitting and engage in prone lying to stretch the hip flexors.
- Prosthetic Fitting: Once the wound is primarily healed and edema has stabilized (typically 4 to 8 weeks postoperatively), the patient is fitted with a preparatory (temporary) prosthesis. Computer-aided design and manufacturing (CAD/CAM) have vastly improved the precision of socket fabrication, allowing for total-contact, anatomically contoured sockets that distribute weight-bearing forces evenly.
Complications and Salvage Techniques
Despite meticulous technique, complications can occur, particularly in the dysvascular population.
- Wound Dehiscence and Necrosis: Often the result of poor level selection or excessive tissue tension. Minor necrosis can be managed with local wound care and delayed secondary healing. Major necrosis requires revision to a higher anatomical level.
- Neuroma Formation: Symptomatic neuromas occur when nerves are transected too distally or become entrapped in the scar tissue. Prevention via high, sharp transection is paramount. Treatment involves targeted nerve blocks, radiofrequency ablation, or surgical excision and targeted muscle reinnervation (TMR).
- Traumatic Amputation Salvage: In cases of severe trauma where standard flaps are unavailable, advanced reconstructive techniques are employed to preserve joint levels. The calcaneal fillet flap or "filet of foot" free flap utilizes the uninjured plantar skin and soft tissue of a traumatically amputated foot, transferred as a pedicled or free microvascular flap, to provide durable, sensate coverage for a marginal transtibial stump, thereby saving the knee joint.
By adhering to strict biomechanical principles, utilizing objective perfusion data, and executing meticulous soft-tissue handling, the orthopedic surgeon transforms the amputation from a procedure of failure into the first critical step of the patient's functional rehabilitation.
📚 Medical References
- lower extremity amputation, J Foot Ankle Surg 37:181, 1998.
- Fujii H, Kazuteru D, Baliarsing A: Transtibial amputation with plantar fl ap for congenital defi ciency of the tibia, Clin Orthop Relat Res 403:186, 2002.
- Gallico GG, Ehrlichman RJ, Jupiter J, et al: Free fl aps to preserve below-knee amputation stumps: long-term evaluation, Plast Reconstr Surg 79:871, 1987.
- Georgiadis GM, Behrens FF, Joyce MJ, et al: Open tibial fractures with severe soft-tissue loss: limb salvage compared with belowthe-knee amputation, J Bone Joint Surg 75A:1431, 1993.
You Might Also Like