Major Upper Extremity Amputations: Surgical Principles and Prosthetic Rehabilitation
Key Takeaway
Major upper extremity amputations require meticulous surgical planning to optimize functional outcomes and prosthetic integration. This comprehensive guide details the indications, biomechanics, and step-by-step surgical techniques for forequarter, shoulder, transhumeral, and forearm amputations. Emphasizing soft tissue management, targeted muscle reinnervation, and advanced myoelectric prosthetic rehabilitation, it provides orthopedic surgeons with evidence-based protocols to maximize patient independence and quality of life following devastating trauma or oncologic resection.
Introduction to Major Upper Extremity Amputations
Major upper extremity amputations are devastating, life-altering procedures reserved for scenarios where limb salvage is impossible, poses a severe threat to the patient's life, or would result in a non-functional, painful appendage. Unlike the lower extremity, where the primary biomechanical goal is weight-bearing and ambulation, the upper extremity is a highly complex instrument of prehension, tactile feedback, and spatial manipulation. Consequently, the surgical philosophy governing upper limb amputation heavily prioritizes the preservation of functional length, meticulous soft tissue handling, and the optimization of the residual limb for advanced prosthetic interfaces.
Drawing upon decades of surgical evolution—from the foundational forequarter techniques of Berger and Littlewood to modern advancements in myoelectric prostheses and targeted muscle reinnervation (TMR)—this masterclass delineates the indications, biomechanics, and step-by-step operative techniques for major upper extremity amputations.
Indications and Preoperative Considerations
The decision to proceed with a major upper extremity amputation is typically dictated by one of four primary pathologies:
- Severe Trauma: Crush injuries, massive avulsions, or thermal/electrical burns where neurovascular reconstruction and soft tissue coverage are unfeasible. Acute management of traumatic forequarter or proximal amputations requires aggressive resuscitation and rapid hemorrhage control.
- Oncology: High-grade malignant soft tissue sarcomas or primary bone tumors of the shoulder girdle and upper limb that cannot be resected with negative margins while preserving a functional limb.
- Vascular Compromise: Irreversible ischemia, often secondary to severe diabetic microvascular disease, embolic events, or compartment syndrome leading to gangrene.
- Sepsis/Infection: Necrotizing fasciitis or chronic, recalcitrant osteomyelitis precluding limb salvage.
Clinical Pearl: In oncologic resections, palliative major amputation may be indicated to alleviate intractable pain, manage fungating wounds, and improve the overall quality of life, even in the presence of metastatic disease.
Biomechanical and Prosthetic Planning
The functional outcome of an upper extremity amputee is directly proportional to the length of the preserved lever arm and the integrity of the surrounding soft tissue envelope.
* Lever Arm Kinematics: A longer residual bone provides a greater mechanical advantage for mobilizing a prosthesis and requires less energy expenditure.
* Socket Interface: The residual limb must withstand the shear and compressive forces of a prosthetic socket. Redundant, hypermobile soft tissue or adherent, invaginated scars will lead to skin breakdown and prosthetic abandonment.
General Surgical Principles
Regardless of the amputation level, several universal surgical tenets must be strictly adhered to:
Bone and Periosteal Management
Bones must be transected cleanly, with the distal ends meticulously contoured and beveled to prevent pressure points. The periosteum should be transected sharply 0.5 cm proximal to the osteotomy site to minimize the risk of terminal osteophyte formation.
Surgical Warning: Osseous overgrowth is a notorious complication in pediatric and congenital amputations. In these cases, autologous stump plasty (capping the bone end with an osteochondral graft) or the use of synthetic caps is highly recommended to prevent the bone from piercing the distal soft tissue.
Nerve Management
The prevention of symptomatic neuromas is paramount. Nerves should be isolated, gently distracted distally, ligated (if accompanied by large vessels), and transected sharply so they retract deep into healthy, well-vascularized muscle beds, away from the incision line and prosthetic contact areas. Modern techniques increasingly employ Targeted Muscle Reinnervation (TMR), where transected motor and sensory nerves are coapted to redundant motor branches of adjacent muscles, simultaneously preventing neuroma formation and providing intuitive control signals for myoelectric prostheses.
Soft Tissue and "Spare Parts" Coverage
Myodesis (securing muscle to bone via drill holes) or myoplasty (suturing antagonist muscles to each other over the bone end) is essential to provide a dynamic, robust soft tissue envelope. In cases of massive trauma, the "spare parts" concept should be utilized. Free fillet flaps harvested from the amputated, non-salvageable distal limb can provide durable, sensate coverage for the amputation stump, preserving critical bone length that would otherwise be sacrificed for primary closure.
Level-Specific Operative Techniques
Forequarter Amputation (Interscapulothoracic Amputation)
Forequarter amputation involves the removal of the entire upper extremity, including the scapula and a portion of the clavicle. It is most commonly indicated for high-grade malignant tumors of the shoulder girdle.
The Anterior (Berger) Approach
- Positioning: The patient is placed in the lateral decubitus position.
- Incision: A racquet-shaped incision is made. The anterior limb begins at the sternoclavicular joint, extends laterally along the clavicle, crosses the coracoid process, and descends into the axilla.
- Clavicular Osteotomy: The clavicle is exposed and osteotomized at the junction of its medial and middle thirds. The subclavius muscle is divided.
- Neurovascular Ligation: The subclavian artery and vein are isolated. The artery is doubly ligated and divided first to allow venous emptying of the limb, followed by the vein. The brachial plexus is identified, infiltrated with local anesthetic, and sharply transected high in the neck.
- Posterior Dissection: The patient is rolled slightly forward. The posterior incision connects the clavicular incision over the acromion and down the vertebral border of the scapula to meet the axillary incision.
- Muscular Detachment: The trapezius, levator scapulae, and rhomboids are detached from the scapula. The latissimus dorsi and serratus anterior are divided, freeing the forequarter.
- Closure: The pectoralis major, latissimus dorsi, and trapezius are approximated to form a muscular pad over the chest wall.
The Posterior (Littlewood) Approach
The Littlewood approach is often preferred for its simplicity and rapid access to the neurovascular bundle from a posterior trajectory, particularly when anterior tumor extension precludes the Berger approach.
1. Incision: Two incisions are made: a cervicoscapular incision and a pectoroaxillary incision.
2. Scapular Mobilization: The trapezius and latissimus dorsi are divided, exposing the entire scapula. The rhomboids and levator scapulae are transected.
3. Neurovascular Control: By elevating the scapula away from the chest wall, the brachial plexus and subclavian vessels are placed on tension and easily visualized from behind. They are ligated and divided under direct vision.
4. Clavicular Division: The clavicle is osteotomized, completing the amputation.
Shoulder Disarticulation
Shoulder disarticulation is indicated when the pathology extends to the level of the glenohumeral joint but spares the scapula and chest wall.
- Incision: A racquet incision is utilized, starting at the coracoid process, extending distally along the deltopectoral groove, curving around the surgical neck of the humerus, and returning through the axilla.
- Deltoid Flap: The deltoid muscle is detached from its humeral insertion and elevated as a large fasciocutaneous-muscular flap. This flap is critical for covering the glenoid fossa.
- Neurovascular Management: The axillary artery and vein are ligated below the pectoralis minor. The brachial plexus cords are transected and allowed to retract.
- Rotator Cuff and Capsule: The rotator cuff tendons (supraspinatus, infraspinatus, teres minor, subscapularis) are transected at their insertions. The joint capsule is incised circumferentially.
- Closure: The deltoid flap is brought down and sutured to the inferior capsule and the severed ends of the pectoralis major and latissimus dorsi.
Transhumeral (Above-Elbow) Amputation
Preservation of humeral length is vital for prosthetic control. The ideal transhumeral amputation preserves at least 50-70% of the humeral length.
- Incision: Equal anterior and posterior fish-mouth flaps are typically used.
- Neurovascular Control: The brachial artery and vein are ligated. The median, ulnar, radial, and musculocutaneous nerves are identified, distracted, and transected.
- Bone Section: The humerus is transected at the desired level. The edges are smoothed with a rasp.
- Myodesis/Myoplasty: The triceps tendon is brought forward over the bone end and sutured to the anterior periosteum and the brachialis/biceps fascia (myodesis). This creates a stable, dynamic pad.
Pitfall: Failure to perform a secure myodesis in a transhumeral amputation will result in a conical, atrophic stump that easily slips out of the prosthetic socket during shoulder abduction.
Elbow Disarticulation
Historically debated, elbow disarticulation is now highly favored over proximal transhumeral amputation. The preservation of the humeral condyles provides a bulbous distal end that allows for self-suspension of the prosthesis and, crucially, transmits rotational torque (internal/external rotation) directly to the prosthesis.
- Incision: A long posterior flap is preferred, as the anterior skin is thin and poorly suited for terminal weight-bearing or socket friction.
- Muscle Management: The flexor-pronator mass and the extensor-supinator mass are detached from the epicondyles.
- Joint Disarticulation: The anterior capsule is incised, and the collateral ligaments are divided. The triceps is detached from the olecranon.
- Condylar Preservation: The articular cartilage of the distal humerus is left intact to minimize bleeding and prevent heterotopic ossification. The epicondyles may be slightly trimmed if they are excessively prominent.
- Closure: The flexor and extensor muscle masses are sutured together over the distal humerus, and the posterior skin flap is brought anteriorly.
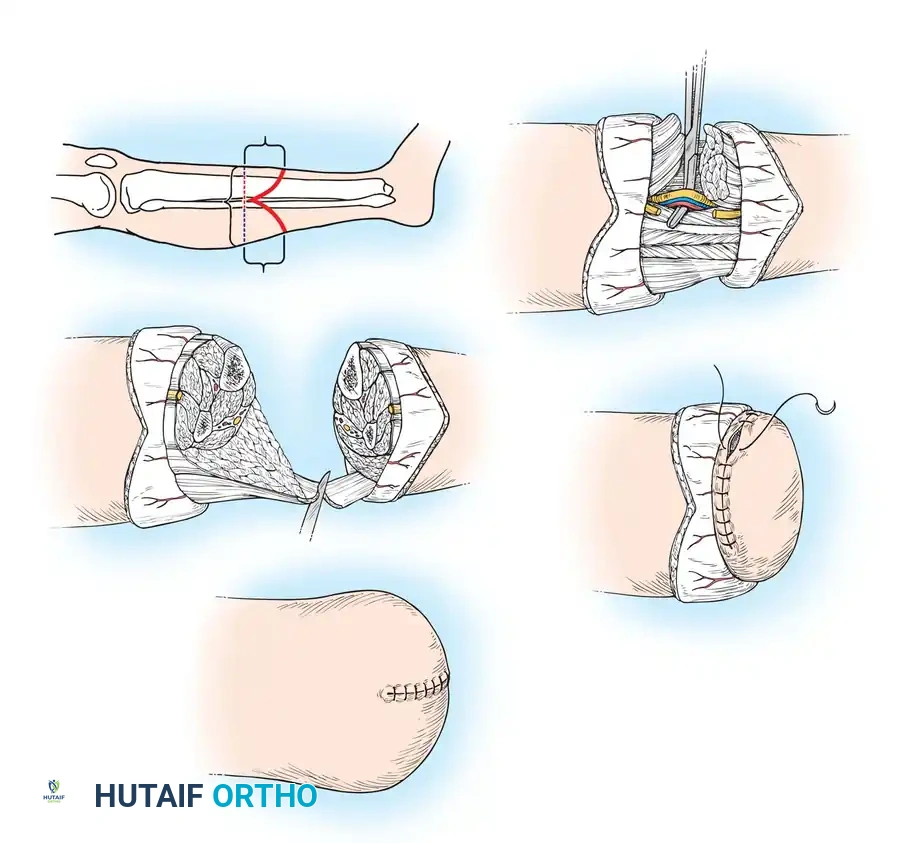
Transradial (Below-Elbow) Amputation
The transradial level is the most common major upper extremity amputation. The ideal length is in the distal third of the forearm, which preserves pronation and supination.
- Incision: Equal volar and dorsal flaps are created.
- Neurovascular Control: The radial and ulnar arteries are ligated. The median, ulnar, and superficial radial nerves are meticulously managed. The posterior interosseous nerve must also be identified and resected to prevent deep stump pain.
- Bone Section: The radius and ulna are transected at the same level. In very short stumps, preserving even 3-5 cm of bone below the biceps tuberosity is critical to maintain elbow flexion.
- Advanced Techniques for Short Stumps: If the residual forearm is excessively short, Ilizarov lengthening of the stump can be employed postoperatively to create a lever arm sufficient for prosthetic fitting. Alternatively, conservation of short stumps by tendon section (releasing the biceps insertion to allow the stump to drop into extension) can be considered.
- Closure: A myoplasty of the volar flexors to the dorsal extensors is performed over the bone ends.
Prosthetic Rehabilitation and Postoperative Care
The ultimate success of an upper extremity amputation is defined by the patient's integration with their prosthesis. The "golden window" for prosthetic fitting is within 30 days post-amputation; delays significantly increase the rate of prosthetic rejection.
Postoperative Protocols
- Rigid Dressings: Immediate application of a rigid cast dressing controls edema, protects the wound, and reduces phantom limb pain.
- Immediate Postoperative Prosthesis (IPOP): Where resources permit, an IPOP can be applied in the operating room. This provides immediate psychological benefit and initiates early bimanual rehabilitation.
Prosthetic Selection
The rational selection of treatment and prostheses depends on the patient's cognitive status, bilateral vs. unilateral amputation, and vocational needs.
- Body-Powered Prostheses: Utilize a figure-of-eight harness and cable system. Glenohumeral flexion and biscapular abduction generate tension on the cable to operate the terminal device (e.g., a split hook). These are highly durable, provide excellent proprioceptive feedback (extended physiological proprioception), and are ideal for heavy manual labor.
- Myoelectric Prostheses: Utilize surface electromyography (EMG) electrodes embedded in the socket to detect muscle action potentials from the residual limb. These signals are amplified to drive electric motors in the prosthetic hand, wrist, or elbow. Myoelectric devices offer superior cosmesis, a greater range of motion without harnessing, and increased grip strength.
- Aesthetic Prostheses: Passive silicone restorations that provide no active prehension but offer unparalleled anatomical realism. These are crucial for patients whose primary concern is body image and psychosocial integration.
Advanced Concepts: Sensory Substitution and TMR
The frontier of upper limb prosthetics involves closing the feedback loop. Sensory substitution systems translate pressure at the prosthetic fingertips into vibrotactile or electrocutaneous stimuli on the residual limb. Furthermore, Targeted Muscle Reinnervation (TMR) not only treats neuromas but creates distinct, amplified EMG signals. By reinnervating the pectoralis or residual arm muscles with the median, ulnar, and radial nerves, patients can operate advanced bionic arms using intuitive, physiological thought processes (e.g., thinking "close hand" fires the reinnervated muscle, which the prosthesis reads and executes).
Conclusion
Major upper extremity amputations demand a paradigm shift from simple tissue ablation to complex reconstructive engineering. By adhering to meticulous surgical principles—optimizing bone length, executing precise soft tissue myodesis, proactively managing nerves, and integrating early with advanced prosthetic technologies—the orthopedic surgeon can profoundly restore function, independence, and dignity to the amputee.
📚 Medical References
You Might Also Like