Masterclass in Digital Amputations: Principles and Flap Coverage
Key Takeaway
Finger amputations require meticulous soft-tissue handling, nerve management, and bone contouring to ensure a painless, functional stump. Treatment of fingertip amputations depends on defect size, exposed bone, and patient age. Techniques range from secondary intention healing to complex local advancements like Kutler and Atasoy V-Y flaps, or regional adipofascial turnover flaps, prioritizing length preservation, durable volar padding, and optimal sensory recovery.
Principles of Finger Amputation
The primary objective of any digital amputation—whether performed in the acute trauma setting or as a secondary reconstructive procedure—is to provide a painless, sensate, and highly functional stump. The hand is an exquisitely specialized organ of interaction, and the preservation of functional length must always be balanced against the necessity of durable, well-padded soft-tissue coverage.
To achieve optimal outcomes, several immutable surgical principles must be observed:
- Flap Design and Volar Padding: The volar skin of the digit is glabrous, highly innervated, and specialized for pinch and grasp. Whenever possible, the volar skin flap should be designed long enough to cover the volar surface and the tip of the osseous structures, joining the dorsal flap without tension. When scarring or a traumatic skin defect makes the fashioning of a classic volar flap impossible, atypical flaps can be improvised, provided the bone end remains adequately padded.
- Nerve Management (Traction Neurectomy): Neuromas at the transected nerve ends are physiologically inevitable. The surgical goal is to ensure these neuromas develop in deeply padded, non-contact areas where they are unlikely to cause mechanical pain. The ends of the digital nerves must be dissected carefully from the volar flap, placed under gentle distal tension (avoiding rupture of more proximal axons), and sharply resected at least 6 mm proximal to the bone end.
- Vascular Control: Digital arteries should be meticulously isolated and cauterized using bipolar electrocautery to minimize thermal necrosis to adjacent structures.
- Tendon Management: Flexor and extensor tendons should be drawn distally, sharply divided, and allowed to retract proximally into their sheaths.
- Bone and Joint Contouring: When an amputation occurs through an interphalangeal joint, the prominent flares of the osseous condyles must be aggressively contoured (rongeured and rasped) to avoid a bulbous, "clubbed" stump, which is both cosmetically displeasing and functionally obstructive.
- Hemostasis: Before the wound is closed, the digital or arm tourniquet must be released. Meticulous hemostasis is mandatory; postoperative hematomas are intensely painful, increase the risk of infection, and severely delay wound healing.
Surgical Warning: Never suture the flexor tendon to the extensor tendon over the bone end. This historical practice tethers the deep flexor mechanism, leading to the "Quadriga Effect," which severely limits the flexion of adjacent, uninjured digits due to the shared muscle belly of the flexor digitorum profundus (FDP).
Fingertip Amputations: Evaluation and Decision Making
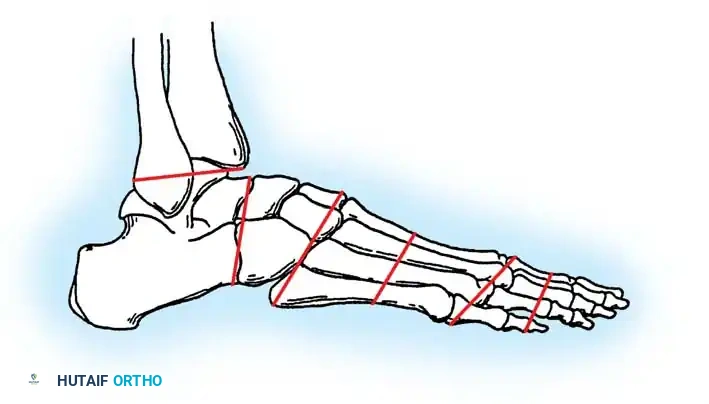
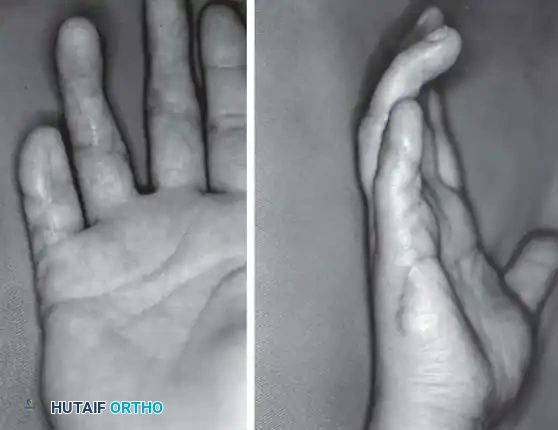
Amputations of the fingertips vary markedly depending on the geometry of the defect, the amount of skin lost, the depth of the soft-tissue defect, and whether the distal phalanx has been exposed or partially amputated. Proper treatment is dictated by the exact type of injury (transverse, volar oblique, or dorsal oblique) and the status of adjacent digits.
Fig. 14-2: Techniques useful in closing amputations of the fingertip. The choice of coverage is dictated by the level of amputation, the angle of the defect, and the necessity of preserving functional length.
Conservative Management: Secondary Intention
Injuries characterized by loss of skin alone, without exposed bone or tendon, can often heal remarkably well by secondary intention. This is particularly true in pediatric populations, where secondary intention wound closure can cover variable amounts of exposed bone in a remarkably short time, often regenerating a near-normal fingertip contour.
In adults, secondary intention is generally reserved for defects smaller than 1 cm² without exposed bone. The wound is managed with non-adherent dressings and heals via contraction and epithelialization.

Fig. 14-3A: Volar view soon after an abrasion injury to the left hand, demonstrating a 2 cm × 2 cm full-thickness pulp skin loss of the middle and ring fingers.

Fig. 14-3B: The same fingers undergoing local wound care at 4 weeks, showing robust granulation tissue and early marginal epithelialization.

Fig. 14-3C: The final result at 8 weeks with no operative intervention, demonstrating excellent contour and durable coverage.
Reamputation vs. Flap Coverage
If the soft-tissue defect is deep and the phalanx is exposed, deeper tissues and skin must be replaced. Reamputation (shortening the bone to allow primary closure) provides ample skin and soft tissue but sacrifices digital length.
Reamputation is often indicated if:
* Other parts of the hand are severely injured, and rapid mobilization is required.
* The patient is older than 50 years or suffers from underlying inflammatory arthritis, where prolonged immobilization for complex flap coverage would result in devastating global hand stiffness.
If length preservation is essential (e.g., thumb amputations, index finger amputations in manual laborers), flap coverage is indicated.
Skin Grafting Techniques
A free skin graft can be used for coverage, but normal sensibility is rarely restored.
* Split-Thickness Skin Grafts (STSG): Often sufficient if the bone is only slightly exposed and its end is nibbled off beneath the fat. STSGs contract significantly during healing (eventually becoming about half their original size), which is advantageous as it pulls sensate volar pulp tissue distally over the bone end.
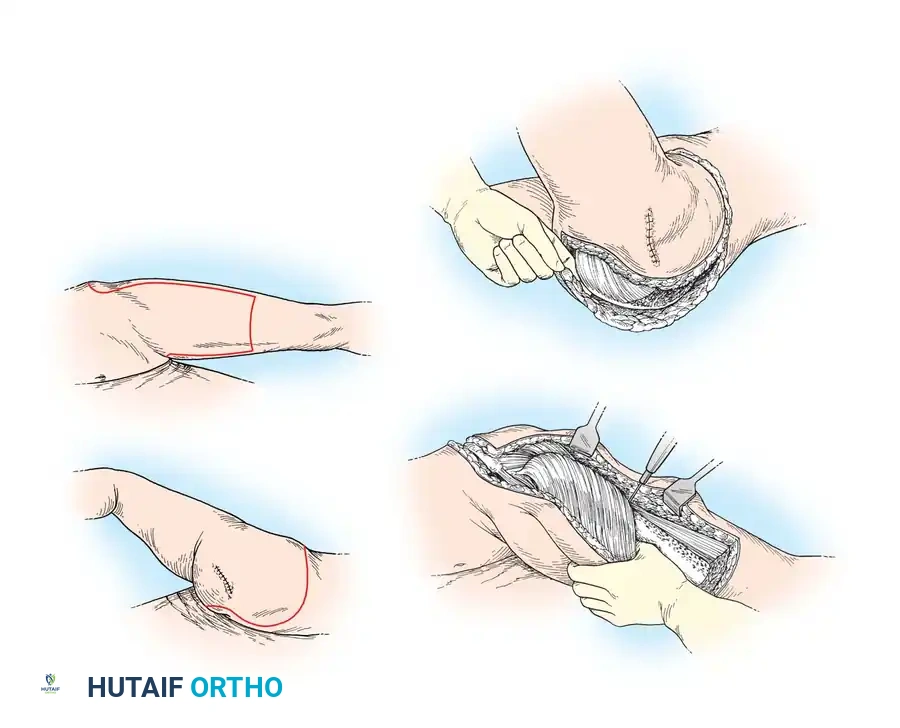
* Full-Thickness Skin Grafts (FTSG): Provide better durability and less contraction. Convenient donor sites include the hypothenar eminence, volar wrist crease, or the medial aspect of the arm just distal to the axilla. All subcutaneous fat must be meticulously excised from the deep surface of the graft to ensure inosculation.
Local Advancement Flaps for Fingertip Coverage
When deeper tissues must be replaced to cover exposed bone, local advancement flaps are preferred as they utilize similar glabrous tissue and do not require immobilizing adjacent digits.
The Kutler V-Y Advancement Flap
The Kutler V-Y flap utilizes bilateral triangular advancement flaps from the lateral aspects of the digit. It is best suited for transverse or slightly volar-oblique fingertip amputations. While it involves the injured finger alone, it provides limited distal advancement and carries a risk of hyperesthesia at the tip.
Surgical Technique 14-1: Kutler V-Y Advancement
* Anesthesia & Preparation: Administer a digital block at the proximal phalanx and apply a digital tourniquet. Débride the tip of the finger of uneven edges of soft tissue and any protruding bone.
* Flap Design: Develop two triangular flaps, one on each side of the finger. The apex of each triangle is directed proximally and centered in the midlateral line of the digit. The sides should measure about 6 mm, and the bases slightly less.
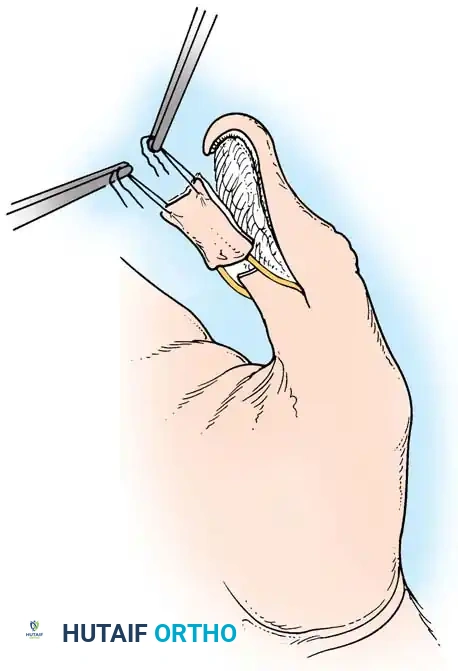
* Mobilization: Incise deeper toward the nail bed and volar pulp. Crucial Step: Do not pinch the flaps with forceps. Insert a skin hook near the base and apply slight distal traction. Using small scissors, divide the fibrous septa of the pulp at the apex just enough to allow the flaps to mobilize distally. Avoid dividing the distal pulp to preserve the neurovascular arborization.
* Bone Preparation: Round off the sharp corners of the distal phalanx to conform to the normal tuft.
* Closure: Approximate the bases of the flaps at the midline over the bone end and stitch them together with small interrupted nonabsorbable sutures. Suture the dorsal edges to the nail bed. The proximal V-shaped defects are closed in a Y-configuration. If tension is excessive, the lateral defects can be left to heal by secondary intention.
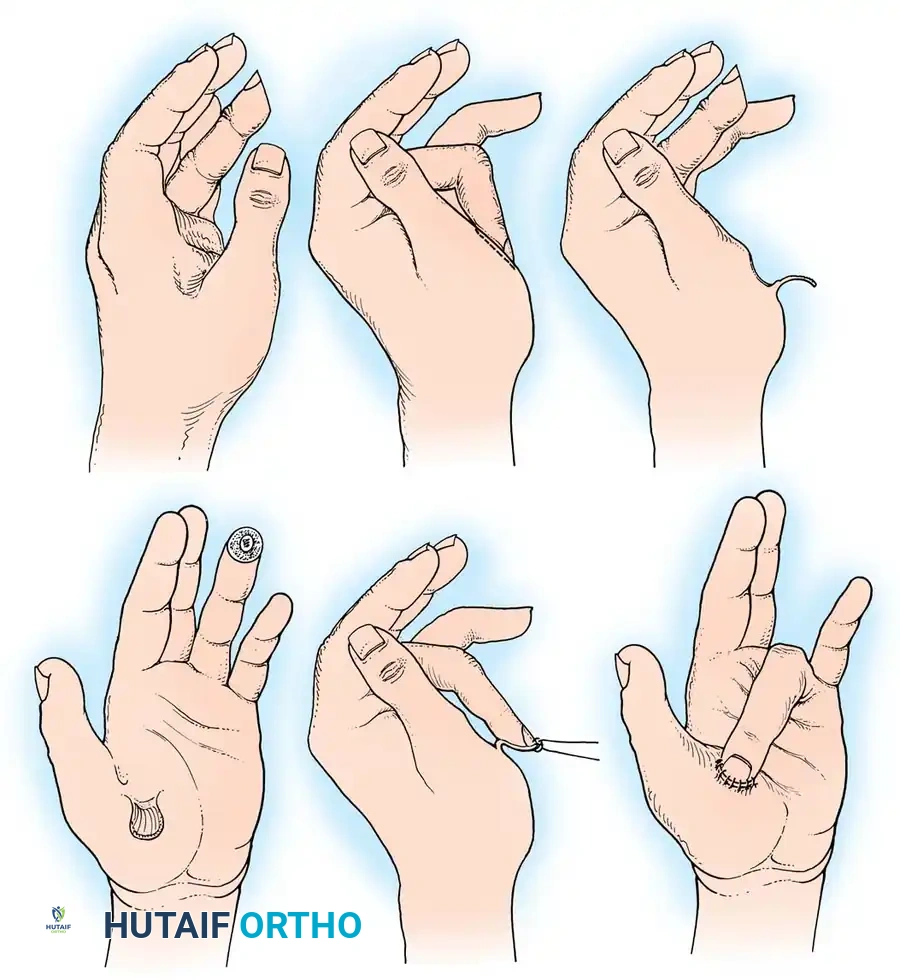
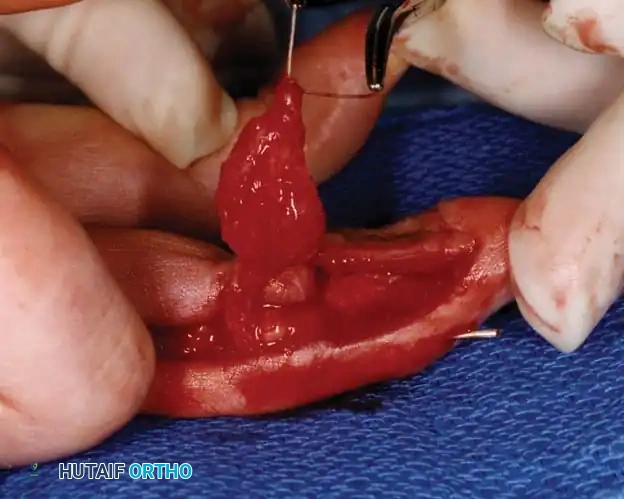
Clinical demonstration of local flap mobilization, highlighting the delicate handling of the neurovascular pedicle during advancement.
The Atasoy V-Y Triangular Advancement Flap
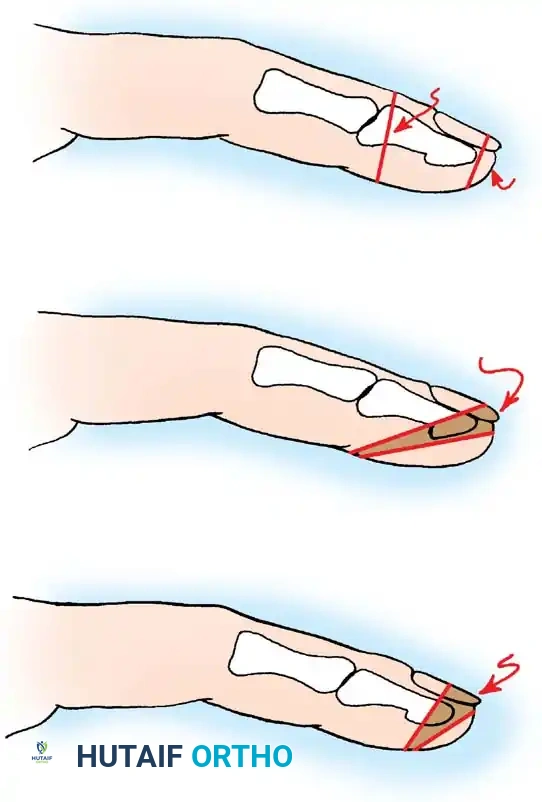
The Atasoy technique utilizes a single, volar-based V-Y advancement flap. It is the workhorse flap for dorsal oblique fingertip amputations where there is adequate volar pulp remaining.
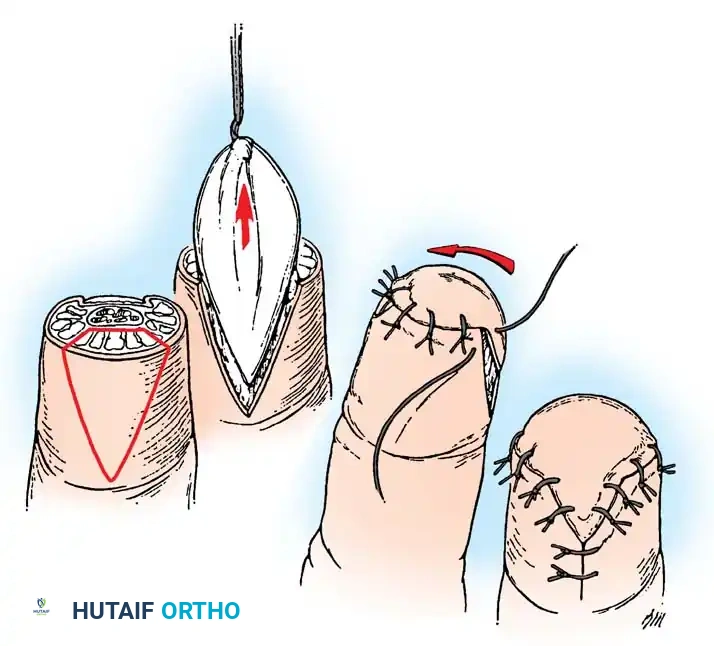
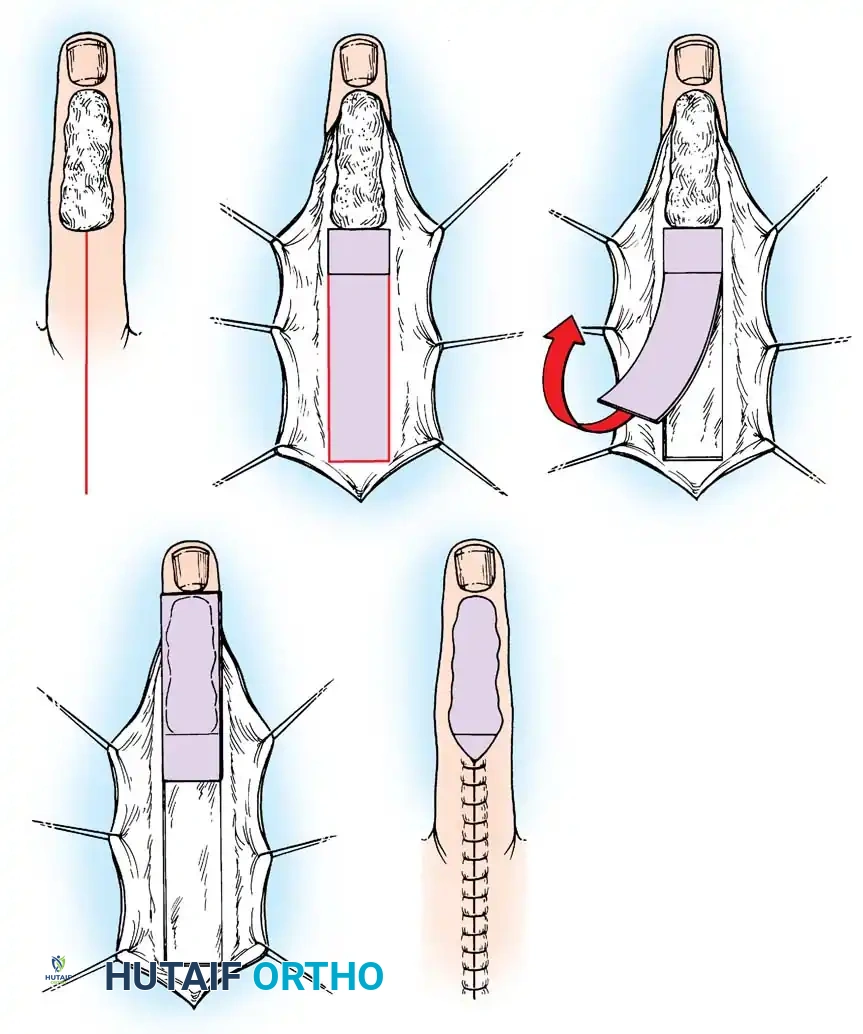
Fig. 14-5: Atasoy V-Y technique. A, Skin incision and mobilization of the triangular flap. B, Advancement of the flap. C, Suturing the base to the nail bed. D, Closure of the defect in a V-Y fashion.
Surgical Technique 14-2: Atasoy V-Y Technique
* Incision: Under tourniquet control, cut a distally based triangle through the pulp skin only. The base of the triangle should equal the width of the cut edge of the nail.
* Dissection: Develop a full-thickness flap, preserving the nerves and blood supply. Carefully separate the fibrofatty subcutaneous tissue from the periosteum and the flexor tendon sheath using sharp dissection.
* Release: Selectively cut the vertical fibrous septa that tether the flap to the deep structures, allowing the flap to advance distally without tension.
* Fixation: Suture the distal skin edge of the flap to the sterile matrix or nail. The proximal defect is closed in a Y-configuration.
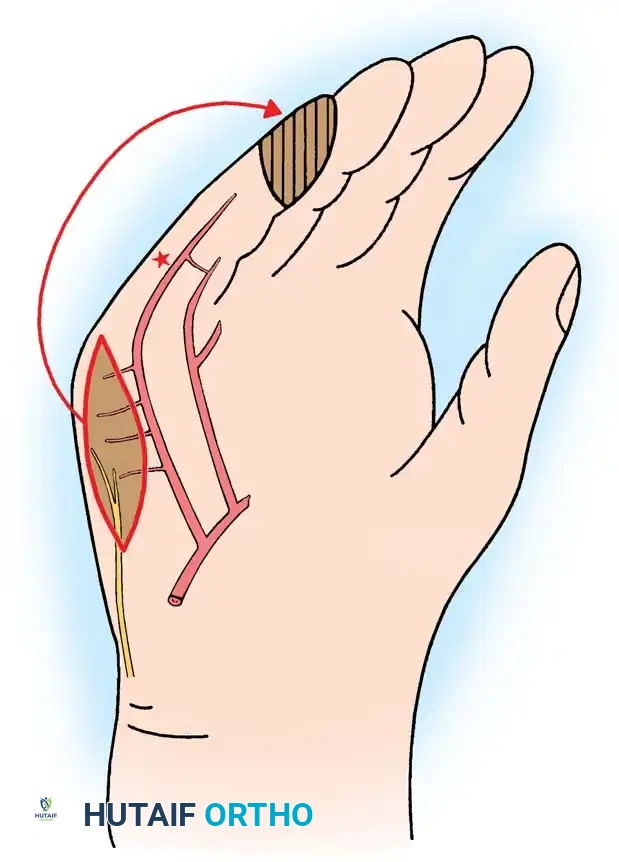
Regional and Complex Flap Coverage
When local tissue is insufficient, regional flaps from the same digit, adjacent digits, or the hand must be employed. Advantages of same-digit coverage include avoiding a second operation for flap division and preventing adjacent finger stiffness.
Dorsal Pedicle and Adipofascial Turnover Flaps
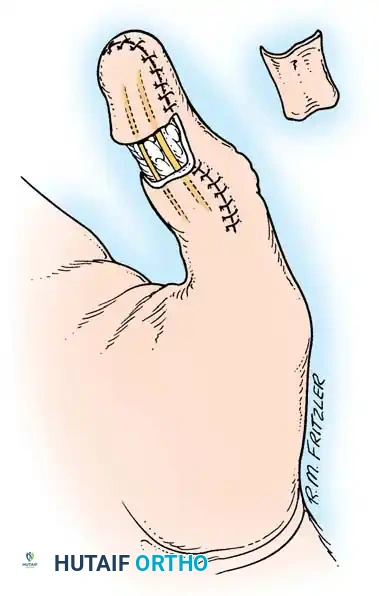
The dorsal pedicle flap is useful when a finger has been amputated proximal to the nail bed, and length preservation is paramount. It can be raised from the dorsum of the injured finger and carried distally.
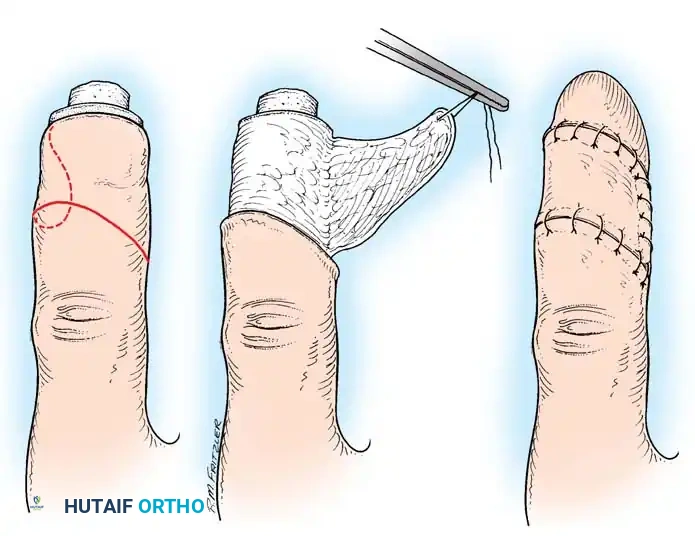
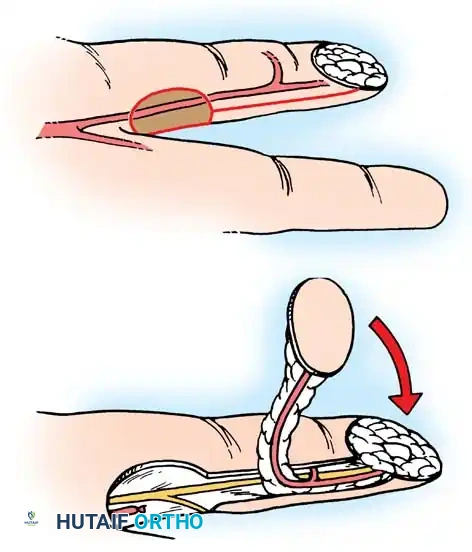
Fig. 14-6: Dorsal pedicle flap useful for amputations proximal to the nail. The flap is elevated on a single pedicle, sutured over the stump, and the donor defect is covered with a split-thickness skin graft.
Dorsal defects may also be managed by adipofascial turnover flaps. The proximal subdermal adipofascial tissues are flipped distally over a vascularized zone to cover exposed bone or tendon, followed by skin grafting.





You Might Also Like