Advanced Reconstruction of Ankle and Hindfoot Malunions: Osteotomies and Arthrodesis
Key Takeaway
Reconstructive surgery for ankle and hindfoot malunions requires precise restoration of biomechanical alignment. This guide details the surgical management of calcaneal malunions via subtalar arthrodesis and corrective osteotomies, alongside fibular lengthening techniques for bimalleolar malunions. Emphasizing evidence-based indications, step-by-step surgical approaches, and postoperative protocols, it provides orthopedic surgeons with a comprehensive framework for optimizing functional outcomes and mitigating posttraumatic arthritis.
Introduction and Epidemiology
Fractures of the ankle mortise represent one of the most common skeletal injuries evaluated and managed by orthopedic surgeons. Within this spectrum, medial malleolus fractures can occur as isolated entities or, more frequently, as components of bimalleolar, trimalleolar, or complex pilon-type fracture patterns. The injury is typically precipitated by rotational mechanisms, most commonly external rotation with the foot in a supinated position, which imparts sequential tension and compressive forces across the osseous and ligamentous structures of the ankle.
Understanding the precise epidemiological distribution and pathomechanical forces is critical for operative planning. Isolated medial malleolus fractures are relatively uncommon compared to lateral malleolus fractures, which represent the most commonly fractured structure in the ankle mortise. When the medial malleolus is compromised, it often signifies a disruption of the primary medial stabilizing structures of the ankle, necessitating meticulous anatomical restoration to prevent post-traumatic arthrosis and chronic instability.
Pathomechanics of Malleolar Trauma
The Lauge-Hansen classification system remains the most robust framework for understanding the rotational mechanisms that dictate malleolar fracture patterns. The system categorizes injuries based on the position of the foot at the time of injury (supination or pronation) and the direction of the deforming force (external rotation, adduction, or abduction).
In a Supination-External Rotation (SER) mechanism, the initial force typically causes failure of the anterior inferior tibiofibular ligament, followed by a spiral/oblique fracture of the lateral malleolus. If the energy continues, it propagates medially, resulting in either a transverse avulsion fracture of the medial malleolus or a rupture of the deltoid ligament. Conversely, a Supination-Adduction (SAD) mechanism drives the talus medially, creating a vertical shear fracture of the medial malleolus, which requires distinct fixation strategies, such as antiglide plating, compared to the standard lag screw constructs used for transverse avulsion fractures.


Surgical Anatomy and Biomechanics
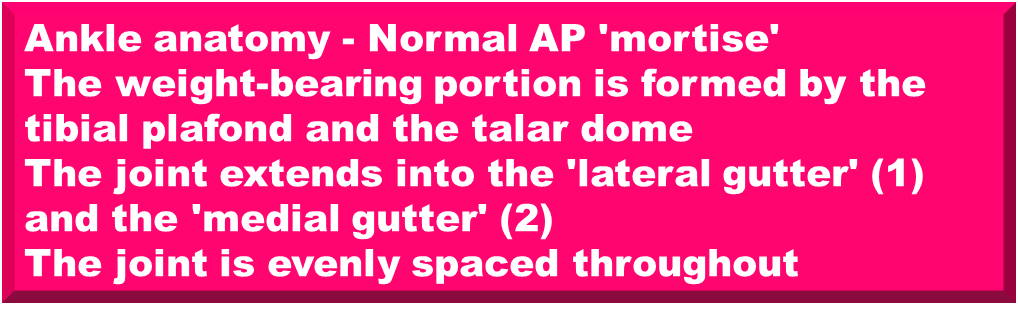
A profound comprehension of the osseous, ligamentous, and neurovascular anatomy of the ankle is non-negotiable for successful surgical intervention. The ankle mortise is a highly congruent, dynamic joint formed by the distal tibial articular surface (plafond), the medial malleolus, and the lateral malleolus, which articulates with the talar dome.
Osteology of the Ankle Mortise
The lateral malleolus represents the lateral flare of the distal fibula and sits within the incisura fibularis, a concave groove along the distal lateral tibia. The posterior malleolus, the posterior flare of the distal tibia, is critical for posterior joint stability and preventing posterior talar subluxation.
The medial malleolus is the medial flare of the distal tibia. Its inner articular surface is divided by an intercollicular groove that demarcates two distinct anatomic prominences: the anterior colliculus and the posterior colliculus. The anterior colliculus is physically larger and extends further distally than the posterior colliculus.


Ligamentous Anatomy and the Deltoid Complex
The collicular anatomy of the medial malleolus is inextricably linked to the origins of the deltoid ligament complex. The anterior colliculus serves as the primary attachment site for the superficial deltoid ligament (comprising the tibionavicular, tibiocalcaneal, and superficial tibiotalar ligaments). The superficial deltoid primarily restricts hindfoot eversion.
The posterior colliculus and the intercollicular groove serve as the attachment sites for the deep deltoid ligament (comprising the deep anterior and deep posterior tibiotalar ligaments). The deep deltoid is the primary medial stabilizer of the ankle mortise, preventing lateral talar excursion and external rotation of the talus. Due to this anatomic arrangement, an isolated fracture of the anterior colliculus may leave the deep deltoid intact (attached to the intact posterior colliculus), thereby preserving the medial stability of the mortise.


Ankle Joint Kinematics
The biomechanics of the ankle joint are dictated by the trapezoidal shape of the talar dome, which is significantly wider anteriorly than posteriorly. This anatomical feature mandates dynamic changes in the mortise during the gait cycle.
During dorsiflexion, the wider anterior portion of the talar dome engages the mortise, forcing the fibula laterally and into external rotation. Conversely, in plantarflexion, the narrower posterior talar dome occupies the mortise, and the talus rotates internally due to the checkrein action of the intact deltoid ligament.
Normal range of motion for the ankle joint consists of 30 degrees of dorsiflexion and 45 degrees of plantarflexion. However, the minimum functional range of motion required for a normal gait cycle is from 10 degrees of plantarflexion to 20 degrees of dorsiflexion. The transmalleolar axis of rotation is approximately 20 degrees externally rotated compared to the coronal axis of the knee joint.


Compartmental Anatomy of the Lower Leg
Surgical approaches to the ankle must respect the compartmental anatomy of the leg, which is divided into four distinct fascial compartments:
1. Anterior Compartment: Contains the tibialis anterior, extensor hallucis longus, extensor digitorum longus, peroneus tertius, anterior tibial vessels, and the deep peroneal nerve.
2. Lateral Compartment: Contains the peroneus longus, peroneus brevis, and the superficial peroneal nerve.
3. Deep Posterior Compartment: Contains the flexor digitorum longus, flexor hallucis longus, tibialis posterior, posterior tibial vessels, and the tibial nerve.
4. Superficial Posterior Compartment: Contains the gastrocnemius, plantaris, and soleus muscles.


Neurovascular Topography
Local structures surrounding the malleoli dictate safe surgical windows.
* Lateral Topography: The peroneal tendons pass posterior to the lateral malleolus, secured under the peroneal retinaculum. Superficial to the peroneal tendons at this level lie the sural nerve and the lesser saphenous vein.
* Medial Topography: Posterior to the medial malleolus lie the critical structures of the deep posterior compartment: the tibialis posterior, flexor digitorum longus, and flexor hallucis longus tendons, along with the posterior tibial vessels and tibial nerve. These structures pass securely under the laciniate ligament (flexor retinaculum), which spans from the medial malleolus to the calcaneus. Anterior to the medial malleolus run the great saphenous vein and the saphenous nerve, which are at high risk during medial approaches.
* Anterior Topography: Under the extensor retinaculum (spanning from the anteromedial tibia to the anterolateral fibula) lie the tibialis anterior, extensor hallucis longus, extensor digitorum longus, and peroneus tertius tendons, alongside the deep peroneal nerve and anterior tibial vessels.


Indications and Contraindications
The decision to proceed with operative fixation of a medial malleolus fracture depends on the fracture morphology, the stability of the ankle mortise, and patient-specific factors. Isolated medial malleolus fractures are rare; when they occur, one must maintain a high index of suspicion for a Maisonneuve fracture (proximal fibula fracture with syndesmotic disruption) or a lateral ligamentous injury.
| Indication Category | Specific Criteria |
|---|---|
| Operative Indications | Displaced medial malleolus fracture (>2mm step-off) |
| Bimalleolar or trimalleolar fracture patterns | |
| Talar shift or mortise widening on static or stress radiographs | |
| Vertical shear fractures of the medial malleolus (SAD mechanism) | |
| Open fractures | |
| Polytrauma requiring early mobilization | |
| Non-Operative Indications | Truly isolated, nondisplaced medial malleolus fractures |
| Anterior colliculus avulsion with an intact deep deltoid (stable mortise) | |
| Non-ambulatory patients | |
| Severe peripheral vascular disease precluding wound healing | |
| Active localized soft tissue infection |


Pre Operative Planning and Patient Positioning
Radiographic Evaluation
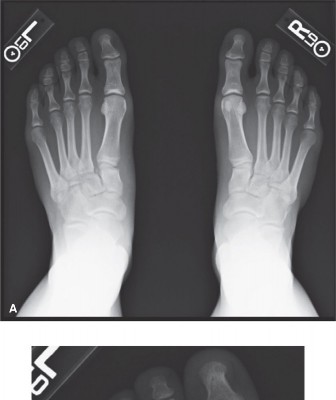
Standard radiographic evaluation includes weight-bearing (if tolerated) anteroposterior, lateral, and mortise views of the ankle. The mortise view, taken with the leg internally rotated 15 to 20 degrees, allows for the assessment of the medial clear space, which should be less than or equal to 4mm. A medial clear space greater than 4mm indicates lateral talar shift and mortise instability.
Computed Tomography (CT) is highly recommended for complex fracture patterns, particularly to evaluate marginal impaction of the tibial plafond, the size and orientation of a posterior malleolus fragment, and the exact trajectory of vertical shear medial malleolus fractures.
Operating Room Setup
The patient is typically positioned supine on a radiolucent operating table. For isolated medial malleolus fractures, a purely supine position is adequate. If a concurrent lateral malleolus or posterior malleolus fracture requires fixation, a bump is placed under the ipsilateral hip to internally rotate the leg, facilitating access to the lateral and posterior structures.
A well-padded thigh or calf tourniquet is applied to provide a bloodless surgical field. Fluoroscopy must be positioned to easily obtain true AP, lateral, and mortise views without compromising the sterile field. The C-arm typically enters from the contralateral side of the table.


Detailed Surgical Approach and Technique
Medial Surgical Approach
A direct medial or slightly anteromedial incision is utilized. The incision begins approximately 2 to 3 cm proximal to the tip of the medial malleolus, centered over the fracture line, and extends distally, curving slightly anteriorly toward the navicular to avoid crossing the flexor crease at a right angle.
Superficial dissection must be meticulous to identify and protect the great saphenous vein and the saphenous nerve, which typically cross the operative field anteriorly. Retraction of these structures should be gentle to prevent postoperative saphenous neuritis.
Deep dissection is carried down to the periosteum. The periosteum over the medial malleolus is often torn. It is imperative to minimize periosteal stripping to preserve the blood supply to the fracture fragments. The posterior aspect of the medial malleolus must be exposed with caution to avoid violating the laciniate ligament and injuring the tibialis posterior tendon or the underlying neurovascular bundle.
Fracture Reduction Strategies
Anatomical reduction of the articular surface is the primary goal. Medial malleolus fractures are notoriously difficult to reduce closed due to the interposition of soft tissue. The torn periosteum or, occasionally, the posterior tibial tendon can become incarcerated within the fracture site.
A dental pick or a Freer elevator is used to clear hematoma and interposed periosteum from the fracture bed. The joint is inspected to ensure no osteochondral fragments are present within the medial gutter. Reduction is achieved using a pointed reduction forceps (Weber clamp). One tine is placed on the distal tip of the medial malleolus and the other on the intact proximal tibial shaft. Compression is applied while ensuring the rotation of the fragment is anatomically aligned with the anterior and posterior cortices.


Internal Fixation Constructs
The choice of fixation is dictated by the fracture morphology, best described by the Herscovici classification system.
Transverse Avulsion Fractures (Herscovici Type B and C):
The gold standard for transverse medial malleolus fractures is fixation with two 4.0 mm partially threaded cancellous lag screws.
1. Guidewire Placement: Two 1.25 mm K-wires are advanced from the distal tip of the medial malleolus, directed perpendicularly to the fracture line into the dense metaphyseal bone of the distal tibia. The wires should be parallel to optimize compression.
2. Drilling and Tapping: A 2.5 mm drill is used over the K-wires. If the bone is dense, tapping with a 4.0 mm tap is performed.
3. Screw Insertion: Two 4.0 mm partially threaded screws (typically 40-45 mm in length) are inserted. Washers may be used in osteopenic bone. Unicortical fixation is generally sufficient, though bicortical fixation (engaging the lateral tibial cortex) can be utilized if pull-out strength is a concern.
Comminuted or Small Avulsion Fractures (Herscovici Type A):
When the distal fragment is too small or comminuted to accept two screws, a tension band wire construct is indicated. Two parallel K-wires are driven across the fracture site. A figure-of-eight stainless steel wire is passed through a drill hole in the distal tibial metaphysis and looped around the K-wires at the tip of the malleolus, converting tensile forces into compressive forces at the articular surface.
Vertical Shear Fractures (Herscovici Type D):
Vertical shear fractures, classically seen in SAD mechanisms, are poorly controlled with lag screws directed from distal to proximal, as this trajectory is parallel to the fracture line and fails to provide compression. These injuries require an antiglide buttress plate. A one-third tubular plate or a specialized medial distal tibia plate is applied to the medial surface of the tibia, acting as a buttress against proximal shear migration. Lag screws can be placed through the plate perpendicularly to the vertical fracture line.


Complications and Management
Despite anatomical reduction and stable fixation, complications following medial malleolus fractures can occur and require prompt recognition and management.
| Complication | Incidence | Etiology and Clinical Presentation | Salvage and Management Strategies |
|---|---|---|---|
| Nonunion | 5-10% | Inadequate reduction, interposed periosteum, poor vascularity. Presents with persistent medial pain and radiographic lucency. | Revision open reduction internal fixation (ORIF) with bone grafting. Consider transition to tension band or plate construct. |
| Malunion | 3-5% | Failure to anatomically reduce the articular step-off. Leads to altered joint kinematics. | Corrective osteotomy if symptomatic; arthrodesis if severe secondary arthrosis has developed. |
| Symptomatic Hardware | 15-20% | Prominent screw heads or K-wires irritating the subcutaneous tissues or posterior tibial tendon. | Hardware removal after complete radiographic union (typically >6-12 months post-op). |
| Saphenous Neuritis | 5-15% | Iatrogenic traction or transection during the surgical approach. Presents with medial dysesthesia. | Gabapentinoids, local desensitization, or surgical neurolysis/excision of neuroma for refractory cases. |
| Post-Traumatic Arthrosis | 10-30% | Cartilage impact at the time of injury or residual articular step-off. | Conservative management (bracing, injections). End-stage disease requires ankle arthrodesis or total ankle arthroplasty. |
Post Operative Rehabilitation Protocols
The rehabilitation protocol must balance the need for fracture site protection with the prevention of joint stiffness and soft tissue contracture.
Early Post Operative Phase
Immediately postoperatively, the ankle is immobilized in a well-padded posterior splint or a bulky Jones dressing with the ankle in neutral dorsiflexion. The patient is instructed to maintain strict non-weight-bearing status on the operative extremity. Elevation above the level of the heart is critical during the first 7 to 14 days to mitigate edema and minimize the risk of wound dehiscence.
At 10 to 14 days, the patient is evaluated in the clinic for suture removal. If the surgical incisions are well-healed, the patient is transitioned to a removable controlled ankle motion (CAM) boot.
Intermediate to Advanced Rehabilitation
Once in the CAM boot, early active range of motion (ROM) exercises are initiated. Patients are instructed to perform active dorsiflexion and plantarflexion out of the boot multiple times a day. Passive stretching is generally avoided in the early phases to prevent undue stress on the fixation construct. The goal is to rapidly achieve the minimum functional ROM of 10 degrees of plantarflexion to 20 degrees of dorsiflexion.
Weight-bearing status is typically advanced at 6 weeks postoperatively, contingent upon radiographic evidence of bridging callus and clinical absence of pain at the fracture site. Progression begins with partial weight-bearing (e.g., 25% to 50% of body weight) using crutches or a walker, advancing to full weight-bearing over the subsequent 2 to 4 weeks.
Physical therapy focuses on restoring proprioception, peroneal and posterior tibial tendon strengthening, and gait normalization. Return to high-impact athletic activities is generally permitted between 4 and 6 months, provided the patient has achieved symmetric strength and full, painless range of motion.
Summary of Key Literature and Guidelines
The management of medial malleolus fractures is heavily guided by historical biomechanical studies and evolving clinical classifications.
The Herscovici Classification (1994) remains the standard for categorizing medial malleolus fractures based on the level of the fracture line relative to the tibial plafond.
* Type A: Avulsion of the tip.
* Type B: Intermediate avulsion (between the tip and the plafond level).
* Type C: Transverse fracture at the level of the plafond.
* Type D: Vertical fracture extending proximal to the plafond.
This classification directly dictates fixation strategy, emphasizing that Type D fractures require buttress plating rather than simple lag screw fixation.
Literature regarding screw configuration (parallel vs. divergent) and thread engagement has been extensively studied. Tornetta et al. demonstrated that fully threaded screws can be used as lag screws (using an overdrill technique) and may provide superior biomechanical pull-out strength in osteopenic bone compared to traditional partially threaded screws. Furthermore, biomechanical analyses confirm that bicortical screw placement (engaging the lateral tibial cortex) significantly increases the construct's resistance to pull-out forces, which is highly relevant in elderly patients with compromised bone density.
Current guidelines from the Orthopaedic Trauma Association (OTA) and the American Orthopaedic Foot & Ankle Society (AOFAS) emphasize the absolute necessity of anatomic reduction of the medial clear space. Failure to restore the medial malleolus anatomically results in lateral talar shift. Ramsey and Hamilton famously demonstrated that a mere 1 mm lateral shift of the talus decreases the tibiotalar contact area by 42%, exponentially increasing peak articular contact stresses and accelerating the onset of post-traumatic arthrosis. Therefore, meticulous surgical technique, rigid internal fixation, and a thorough understanding of the surrounding compartmental and neurovascular anatomy remain paramount.
Clinical & Radiographic Imaging
You Might Also Like