Coracoclavicular Suture Fixation and Upper Extremity Instability Management
Key Takeaway
Coracoclavicular suture fixation and acromioclavicular joint reconstruction are critical procedures for managing high-grade AC joint separations. This comprehensive guide details the Stewart technique, utilizing transacromial Kirschner wire fixation, and the Weaver-Dunn method, which transfers the coracoacromial ligament to the distal clavicle. Proper patient positioning, meticulous soft tissue handling, and strict postoperative protocols are essential to restore shoulder biomechanics and prevent recurrent instability.
INTRODUCTION TO ACROMIOCLAVICULAR INSTABILITY
Acromioclavicular (AC) joint separations are common orthopedic injuries, frequently resulting from a direct blow to the superior aspect of the shoulder with the arm adducted. The biomechanical stability of the AC joint relies on a complex interplay between the static stabilizers—namely the acromioclavicular ligaments (providing horizontal stability) and the coracoclavicular (CC) ligaments (the conoid and trapezoid, providing vertical stability)—and the dynamic stabilizers, including the deltotrapezial fascia.
While low-grade injuries (Rockwood Types I and II) are universally managed nonoperatively, high-grade separations (Types IV, V, and VI) necessitate surgical intervention to restore shoulder kinematics. The management of Type III injuries remains controversial, though operative intervention is generally favored in elite athletes, heavy manual laborers, and patients with significant scapular dyskinesia.
This masterclass details the operative management of AC joint instability, focusing on Coracoclavicular Suture Fixation via the Stewart technique and the classic Weaver-Dunn Procedure, alongside critical considerations for associated upper extremity instability patterns.
PREOPERATIVE EVALUATION AND IMAGING
A meticulous clinical and radiographic evaluation is paramount. Patients typically present with localized pain, swelling, and a visible step-off at the AC joint.
Clinical Pearl: Always assess the integrity of the deltotrapezial fascia. A severe Type V injury is characterized by a >100% superior displacement of the clavicle relative to the acromion, often stripping the deltoid and trapezius from the distal clavicle, leading to profound scapular ptosis.
Standard radiographic evaluation must include:
* Anteroposterior (AP) View: To assess general shoulder anatomy.
* Zanca View: A 10- to 15-degree cephalad tilt view, utilizing 50% standard penetration, which isolates the AC joint without superimposition of the scapular spine.
* Axillary Lateral View: Critical for identifying anterior or posterior displacement of the distal clavicle (Type IV injuries).
SURGICAL TECHNIQUE 1: THE STEWART TECHNIQUE (CORACOCLAVICULAR SUTURE FIXATION)
The Stewart technique combines distal clavicle excision, direct repair of the coracoclavicular ligaments, and temporary transacromial Kirschner wire (K-wire) fixation to neutralize deforming forces during ligamentous healing.
1. Patient Positioning and Anesthesia
The patient is placed in the beach chair position with the head secured in a neutral position. General anesthesia is typically employed, often supplemented with an interscalene regional block for postoperative analgesia. The operative arm must be draped free to allow for intraoperative manipulation and reduction of the shoulder girdle.
2. Surgical Approach and Exposure
- Make an anterior curved incision (often referred to as a "bra-strap" or saber incision) starting just posterior to the AC joint, extending anteriorly over the distal clavicle, and curving inferiorly toward the tip of the coracoid process.
- Develop the subcutaneous flaps to expose the deltotrapezial fascia.
- Incise the capsule and the superior acromioclavicular ligament strictly in line with the clavicle. This allows for meticulous subperiosteal exposure of the distal clavicle, preserving the robust fascial sleeves for subsequent capsular and ligamentous repair.
3. Distal Clavicular Excision
Resection of the distal clavicle prevents postoperative AC joint arthrosis and impingement, which are common sequelae of AC joint trauma.
- Resect subperiosteally the lateral 1 cm of the clavicle.
- Use a bone-cutting forceps or an oscillating saw to osteotomize the bone obliquely in an inferolateral direction.
- Remove the superior subcutaneous edge of the remaining end of the bone with a file or rasp to prevent soft tissue irritation beneath the skin.

FIGURE 1: Stewart technique for acute dislocation of the acromioclavicular joint. (A) Radiograph demonstrating the acute injury with superior displacement of the distal clavicle.
4. Coracoclavicular Ligament Preparation
- Identify the ruptured ends of the conoid and trapezoid ligaments.
- Place heavy, nonabsorbable mattress sutures (e.g., No. 2 or No. 5 braided composite sutures) into the ruptured coracoclavicular ligaments.
- Do not tie these sutures yet. They will be tied only after the joint is anatomically reduced and pinned.
5. Transacromial Kirschner Wire Fixation
Temporary rigid fixation is required to protect the CC ligament repair.
- Insert two smooth Kirschner wires (the size of a standard guidewire, typically 2.0 mm or 5/64 inch) about 2 cm apart through the lateral border of the acromion.
- Direct them so that they enter the middle of the articular facet of the acromion.
Surgical Warning: To accomplish this trajectory more easily and accurately, pass the wires retrograde from the acromial articular surface, through the acromion, and out through the lateral skin.
- Have an assistant elevate the arm and apply downward pressure on the clavicle to hold the lateral end of the clavicle in a perfectly reduced, normal anatomical position.
- Advance the K-wires antegrade across the AC joint and into the medullary canal of the clavicle for a depth of 2.5 to 4.0 cm.

FIGURE 2: Stewart technique. (B) Six weeks after surgery, demonstrating transacromial K-wire fixation maintaining anatomic reduction.
6. Final Fixation and Closure
- As described for the modified Phemister technique, verify the position of the K-wires using intraoperative fluoroscopy.
- Once confirmed, bend the lateral ends of the wires to prevent medial migration, cut them short, and bury them beneath the skin to prevent infection.
- Tie the previously placed mattress sutures in the CC ligaments.
- Meticulously repair the deltotrapezial fascia over the distal clavicle. This dynamic stabilizer is critical for long-term success.

FIGURE 3: Stewart technique. (C) Three months after surgery, following the removal of the K-wires, showing maintenance of reduction and a healed distal clavicle excision.
SURGICAL TECHNIQUE 2: THE WEAVER-DUNN PROCEDURE
As an alternative to direct repair and pinning, the method of coracoclavicular reconstruction described by Weaver and Dunn utilizes the native coracoacromial (CA) ligament. This technique is particularly useful in chronic separations where the native CC ligaments have retracted and are irreparable.
1. Preparation of the Coracoacromial Ligament
- Expose the distal clavicle and coracoid process as described above. Perform a standard distal clavicle excision (resecting 1 to 1.5 cm).
- Identify the coracoacromial ligament. Detach it from its insertion on the undersurface of the acromion.
Clinical Pearl: In the modified Weaver-Dunn technique, a small fleck of acromial bone is harvested with the ligament to facilitate bone-to-bone healing within the clavicle.
- Apply traction to the coracoacromial ligament to determine the proper length necessary to maintain the reduction of the clavicle.
- Excise any excess ligament length.
- Place a locking mattress suture (using a No. 1 or No. 2 nonabsorbable material) into the free end of the CA ligament, leaving the suture ends free for passage.
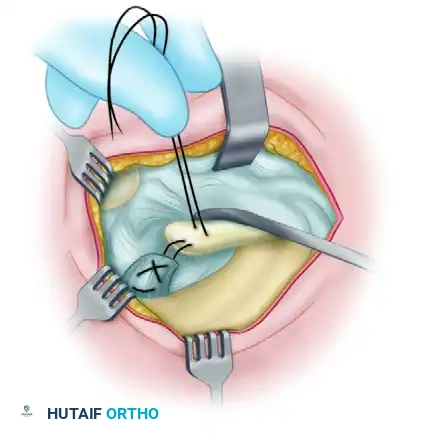
FIGURE 4: Technique of Weaver and Dunn for acromioclavicular separations. (A) Passing the nonabsorbable suture through the detached coracoacromial ligament.
2. Clavicular Preparation and Ligament Transfer
- Drill two small osseous tunnels (usually 2.0 mm) in the superior cortex of the distal clavicle, approximately 1 cm medial to the resected edge.
- Pass one suture limb through each drill hole from inferior to superior.
- Hold the clavicle in the anatomically reduced position relative to the acromion and coracoid.
- Pull firmly on the suture limbs to draw the free end of the coracoacromial ligament directly into the medullary canal of the distal clavicle.
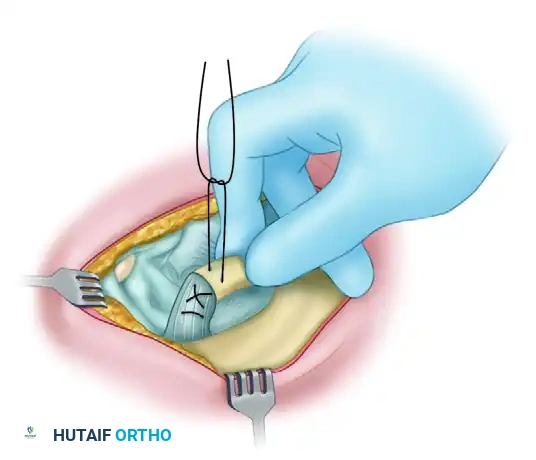
FIGURE 5: Technique of Weaver and Dunn. (B) Pulling the suture to bring the coracoacromial ligament into the medullary canal of the clavicle while reduction is maintained.
3. Final Fixation
- Tie the suture securely over the superior bony bridge of the clavicle while the reduction is rigidly maintained by an assistant.
- Repair the capsule and superior ligaments of the AC joint.
- If supplementary CC fixation (e.g., suture buttons or cerclage) was utilized to protect the transfer, ensure it is tensioned appropriately before final closure.
POSTOPERATIVE CARE AND REHABILITATION
Strict adherence to postoperative protocols is mandatory to prevent elongation of the repair or hardware failure.
- Weeks 0-1: The operative arm is immobilized in a sling. Only gentle, active circumduction exercises (pendulums) are permitted to prevent adhesive capsulitis.
- Weeks 2-4: Sutures are removed at 14 days. Passive and active-assisted range of motion (ROM) exercises are gradually increased, strictly avoiding cross-body adduction and heavy lifting.
- Weeks 4-8: Heavy lifting remains prohibited. If K-wires were used (Stewart technique), they are typically removed in the clinic under local anesthesia at the 6-week mark.
- Weeks 8+: Normal activities of daily living can be resumed. Progressive strengthening of the deltoid and periscapular stabilizers is initiated.
- Return to Sport: Contact sports and heavy overhead labor must be avoided for at least 8 to 12 weeks, pending radiographic evidence of maintenance of reduction and clinical stability.
COMPREHENSIVE MANAGEMENT OF CONCOMITANT UPPER EXTREMITY INSTABILITY
While AC joint separations represent a significant portion of shoulder girdle trauma, the orthopedic surgeon must also be adept at managing concomitant or isolated instability patterns in the upper extremity, specifically radiocapitellar and glenohumeral dislocations.
Elbow Instability: The Annular Ligament
In cases of complex elbow trauma, the radial head may be displaced anteriorly. While many acute dislocations can be easily reduced manually, the integrity of the annular ligament is paramount.
Because the annular ligament has been ruptured or displaced, the dynamic pull of the biceps brachii muscle often causes the radial head dislocation to recur. Unless the radial head remains anatomically reduced, it will severely limit flexion and supination of the joint.
Consequently, open reduction and direct repair or reconstruction of the annular ligament is strictly indicated under the following conditions:
1. When the dislocation recurs after closed reduction and immobilization of the elbow in more than 90 degrees of flexion.
2. When the dislocation has gone untreated or unrecognized for 2 to 4 weeks.
3. When it is irreducible by closed means, which is usually due to the radial head becoming trapped by interposed soft tissues (e.g., capsule or annular ligament stump).
Surgical Warning: When a radial head dislocation has gone untreated for more than 4 or 5 weeks in an adult, the articular cartilage is often irreparably damaged, and the soft tissue contractures are severe. In these chronic, neglected cases, radial head excision (or replacement with a radial head arthroplasty) should be considered.
Glenohumeral Instability: Pathoanatomy and Classification
Uncomplicated anterior dislocations of the shoulder rarely require open reduction. However, some acute anterior dislocations of the shoulder are irreducible due to the interposition of the long head of the biceps tendon, the greater tuberosity, or large fracture fragments of the anterior glenoid rim. Furthermore, massive rotator cuff tears that require concurrent repair have been frequently reported with shoulder dislocations in older adults.
Understanding the biomechanics and pathoanatomy seen with recurrent dislocations is critical for surgical planning. In an effort to determine which shoulders are prone to recurrent dislocation, Baker et al. identified specific intraarticular lesions of the shoulder and classified these into three distinct groups:
- Group 1: Patients (6 in the original cohort) had isolated capsular tears with no labral lesions. The shoulders were stable on examination under anesthesia (EUA). Hemorrhage was present in the inferior capsule between the middle and inferior glenohumeral ligaments. No Hill-Sachs lesions were identified.
- Group 2: Patients (11 in the cohort) had subluxable shoulders on EUA. Arthroscopy revealed partial detachment of the labrum from the glenoid rim and disruption of the inferior glenohumeral ligament (IGHL) attachment to the biceps insertion. Hill-Sachs lesions (impaction fractures of the posterolateral humeral head) were identified in this group.
- Group 3: Patients (28 shoulders) demonstrated gross instability on EUA. Pathoanatomy included complete disruption of the IGHL insertion anteriorly (a classic Bankart lesion). Significant Hill-Sachs lesions were universally seen.
Operative vs. Nonoperative Management of Shoulder Instability
Recurrent instability in young, athletic patients has been reported in up to 90% of patients treated nonoperatively after a first-time dislocation. Conversely, up to a 12% recurrence rate has been reported even in operatively treated shoulders, highlighting the challenging nature of this pathology.
Arthroscopic stabilization (Bankart repair with suture anchors) has been highly recommended in active, young patients (under 25 years of age) with no prior history of subluxation or impingement, who would otherwise face an unacceptably high risk of recurrent dislocations after an acute traumatic event.
While we currently favor initial nonoperative management (immobilization followed by aggressive physical therapy focusing on dynamic stabilizers) for the majority of first-time dislocations, we consider early arthroscopic stabilization procedures an appropriate and evidence-based alternative in selected high-risk patients.
CONCLUSION
The surgical management of upper extremity instability requires a profound understanding of joint biomechanics and meticulous surgical execution. For the acromioclavicular joint, both the Stewart technique (utilizing K-wire fixation and direct CC repair) and the Weaver-Dunn procedure (utilizing CA ligament transfer) remain foundational techniques in the orthopedic surgeon's armamentarium. When combined with strict postoperative rehabilitation and a vigilant approach to concomitant glenohumeral or radiocapitellar pathology, surgeons can reliably restore function, alleviate pain, and return patients to their pre-injury levels of activity.
You Might Also Like
