Acromioclavicular Joint Injuries: Classification & Surgery
Key Takeaway
Acromioclavicular (AC) joint injuries typically result from a direct downward force on the shoulder dome. Management depends heavily on the Rockwood classification, which categorizes injuries from Type I to VI based on ligamentous and muscular disruption. While Types I through III are generally managed nonoperatively with excellent functional outcomes, Types IV, V, and VI require surgical intervention to restore coracoclavicular stability and shoulder biomechanics.
ACROMIOCLAVICULAR JOINT: PATHOANATOMY AND BIOMECHANICS
The acromioclavicular (AC) joint is a diarthrodial joint that serves as the sole articular articulation between the axial skeleton and the upper extremity via the clavicle and scapula. Understanding the intricate biomechanics and stabilizing structures of this region is paramount for the orthopedic surgeon, as it dictates both conservative management and surgical reconstruction strategies.
Etiology and Mechanism of Injury
Injuries to the acromioclavicular joint usually are the result of a high-energy force applied downward on the acromion. The most common mechanism of injury is a direct fall onto the dome of the shoulder with the arm adducted. As the force drives the acromion inferiorly, the clavicle rests against the first rib, which acts as a fulcrum and blocks further downward displacement of the clavicle.
As a result, if the clavicle does not fracture, the applied kinetic energy sequentially ruptures the acromioclavicular ligaments, followed by the coracoclavicular (CC) ligaments. Injuries to the other structures in this area may include severe tears in the clavicular attachments of the deltoid and trapezius muscles; fractures of the acromion, clavicle, and coracoid; disruption of the acromioclavicular fibrocartilage (intra-articular disc); and osteochondral fractures of the articular cartilage of the AC joint.
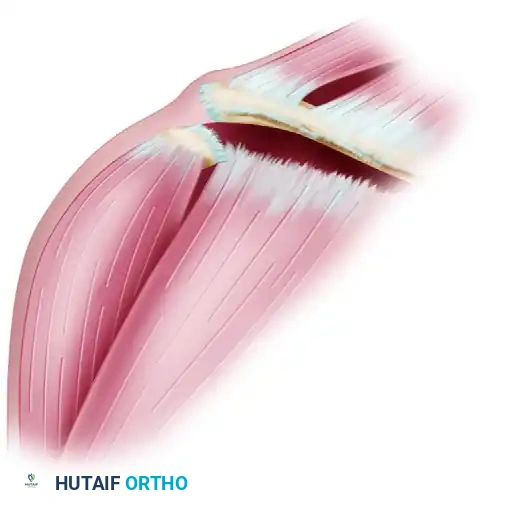
Figure 1: Dislocation of the clavicle often causes extensive tears in the clavicular attachments of the deltoid and trapezius muscles, destabilizing the dynamic suspensory mechanism of the shoulder.
Biomechanical Cadaveric Studies
The severity of any superior or posterior displacement of the clavicle is determined by the extent of injury to the AC ligaments, the CC ligaments (conoid and trapezoid), the AC joint capsule, and the dynamic stabilizers (trapezius and deltoid muscles).
In landmark cadaveric dissections, Rosenørn and Pedersen demonstrated the sequential nature of this instability. They found that if the AC ligament, the joint capsule, and the deltotrapezial fascia were cut, proximal displacement of the clavicle ranged from 0.5 to 1.0 cm. More importantly, considerable anteroposterior (AP) instability was present when the AC ligament and joint capsule were sectioned, highlighting that the AC ligaments are the primary restraint to AP translation.
If, in addition to these structures, the robust coracoclavicular ligaments were also divided, the superior clavicular displacement increased dramatically, ranging from 1.5 to 2.5 cm. Horn further noted the clinical association of tears or avulsions of the deltoid and trapezius muscles with complete tears of the AC and CC ligaments, emphasizing that high-grade separations are not merely ligamentous injuries, but complex musculotendinous disruptions.
Clinical Pearl: The AC ligaments provide primary stability in the anteroposterior plane, while the CC ligaments (specifically the conoid) provide primary stability in the superior-inferior plane. Surgical reconstruction must address both vectors to prevent late construct failure.
THE ROCKWOOD CLASSIFICATION SYSTEM
Although historical texts utilized a simple three-grade system of severity, modern orthopedic practice relies on the Rockwood classification, which subclassifies these injuries into types I through VI based on the degree and direction of displacement, as well as the specific anatomic structures disrupted.
Type I Injuries
Type I injuries result from minor strains of the acromioclavicular ligament and joint capsule. The coracoclavicular ligaments remain completely intact. The AC joint is stable to stress testing, and pain is minimal to moderate. Although radiographs initially may be negative, periosteal calcification at the distal end of the clavicle may become apparent weeks later.

Figure 2: Rockwood Type I. Neither the acromioclavicular nor coracoclavicular ligaments are completely disrupted.
Type II Injuries
More significant forces cause type II injuries, wherein the acromioclavicular ligament and the joint capsule are completely ruptured, but the coracoclavicular ligaments remain intact. The AC joint is unstable, especially in the anteroposterior plane. On radiographs, the lateral end of the clavicle may ride higher than the acromion, but usually by less than the thickness of the clavicle. Stress radiographs may be necessary to assess the true degree of instability.

Figure 3: Rockwood Type II. The acromioclavicular ligament is disrupted, but the coracoclavicular ligament remains intact.
Type III Injuries
Type III injuries consist of complete disruption of both the acromioclavicular and coracoclavicular ligaments, alongside tearing of the distal clavicular attachment of the deltoid muscle. The distal clavicle is elevated above the acromion by at least the thickness of the clavicle (100% displacement).
Biomechanics Insight: Traditionally, this elevation of the clavicle has been attributed solely to the superior pull of the trapezius muscle. However, Rockwood astutely suggested that the scapula, including the glenohumeral joint, is actually depressed by the weight of the arm, rather than the clavicle being purely elevated. This combined vector creates the massive gap between the clavicle and the acromion.
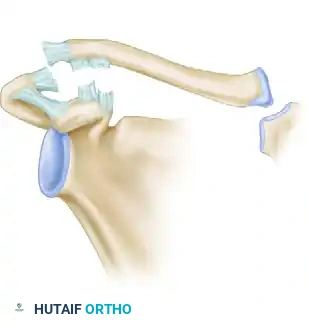
Figure 4: Rockwood Type III. Both the AC and CC ligaments are disrupted, resulting in 100% superior displacement.
Type IV Injuries
In type IV injuries, the same ligamentous structures are disrupted as in grade III injuries. However, the defining characteristic is that the distal clavicle is displaced posteriorly into or completely through the trapezius muscle. This posterior displacement is best visualized on an axillary lateral radiograph. These injuries are highly symptomatic and cause severe pain with any shoulder motion.
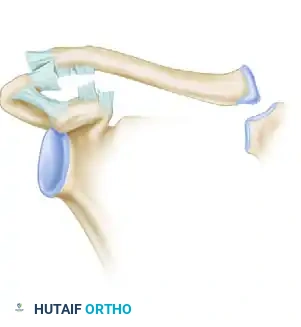
Figure 5: Rockwood Type IV. Ligaments are disrupted, and the distal end of the clavicle is displaced posteriorly into the trapezius muscle.
Type V Injuries
Type V injuries represent a severe progression of the Type III pattern. The distal attachments of the deltoid and trapezius to the clavicle are completely detached from the distal half of the clavicle. The acromioclavicular joint is displaced 100% to 300%, and a gross, clinically obvious separation between the clavicle and the acromion is present. The patient will present with a severe "step-off" deformity and profound shoulder droop.

Figure 6: Rockwood Type V. Ligaments and muscle attachments are completely disrupted, and the clavicle and acromion are widely separated (100-300%).
Type VI Injuries
Type VI injuries are exceedingly rare and are caused by a mechanism of extreme abduction combined with a downward force that tears the AC and CC ligaments. The distal clavicle is dislocated inferiorly, resting under the coracoid process and posterior to the conjoined tendons of the short head of the biceps and coracobrachialis. This injury often presents with associated neurovascular compromise or severe paresthesias due to brachial plexus compression.

Figure 7: Rockwood Type VI. Ligaments are disrupted, and the distal clavicle is dislocated inferior to the coracoid process.

Figure 8: Detailed view of the Type VI dislocation, demonstrating the clavicle trapped posterior to the conjoined tendon of the biceps and coracobrachialis.
EVIDENCE-BASED MANAGEMENT STRATEGIES
The management of AC joint injuries is dictated by the Rockwood classification, patient age, activity level, and occupational demands.
Nonoperative Management (Types I, II, and III)
Types I and II injuries are universally treated nonoperatively. If the distal clavicle is displaced no more than one-half of its thickness, strapping, splinting, or immobilization with a simple sling for 2 to 3 weeks is usually successful. The primary goal is comfort and reduction of acute inflammation. Reinstitution of activities is permitted when comfort allows; however, six weeks must pass before heavy lifting or contact sports can be safely resumed to allow for adequate ligamentous scarring.
Treatment of type III injuries has historically been controversial but has shifted heavily toward nonoperative management in recent years. Isokinetic testing after nonsurgical treatment of type III AC dislocations has revealed that strength and endurance are comparable on the affected and uninjured sides. Most patients have no difficulty with activities of daily living.
At our clinic, we generally treat all type III AC joint separations nonoperatively initially, reserving late reconstruction for patients who develop chronic pain or scapular dyskinesia. However, elite overhead athletes or heavy manual laborers may occasionally report pain with contact sports and throwing, prompting early surgical consideration.
Surgical Warning: It has been suggested that conservative treatment fails in a small subset of patients chiefly because of the interposition of the articular disc, frayed capsular ligaments, and fragments of articular cartilage blocking spontaneous reduction and causing chronic mechanical impingement.
Operative Indications (Types IV, V, and VI)
In types IV, V, and VI injuries, there is universal consensus among orthopedic surgeons that the displacement of the acromioclavicular joint is too great to accept. The severe disruption of the deltotrapezial fascia and the gross instability of the shoulder girdle lead to chronic pain, weakness, and severe scapular dyskinesia. Therefore, open reduction and internal fixation (ORIF) or ligamentous reconstruction is strictly indicated.
SURGICAL TECHNIQUE: ACROMIOCLAVICULAR RECONSTRUCTION
Modern surgical management of high-grade AC joint separations focuses on anatomic reconstruction of the coracoclavicular ligaments and robust repair of the deltotrapezial fascia.
Patient Positioning and Preparation
- Positioning: The patient is placed in the beach-chair position with the head secured. The operative arm must be draped free to allow for manipulation of the shoulder girdle, which is critical for reducing the AC joint.
- Fluoroscopy: A C-arm should be positioned to allow for orthogonal views (Zanca and axillary) to confirm reduction and hardware placement.
Surgical Approach
- Incision: A "sabre-cut" or bra-strap incision is made starting 1 cm posterior to the AC joint, extending anteriorly over the distal clavicle, and curving inferiorly toward the tip of the coracoid process.
- Dissection: The subcutaneous tissues are divided. The deltotrapezial fascia is carefully incised in line with the clavicle. It is imperative to preserve full-thickness flaps of this fascia for later repair, as it is a critical dynamic stabilizer.
- Exposure: The distal clavicle and the AC joint are exposed. The AC joint is debrided of the torn meniscus and frayed capsular remnants to allow for anatomic reduction. The anterior deltoid is split in line with its fibers to expose the superior surface and base of the coracoid process.
Coracoclavicular Fixation (Cortical Button Technique)
The current gold standard for acute injuries (< 3 weeks old) is suspensory cortical button fixation, which mimics the native vectors of the conoid and trapezoid ligaments.
- Drilling the Coracoid: A guide pin is placed centrally at the base of the coracoid process. A 4.0 mm or 4.5 mm cannulated drill is passed over the pin through the coracoid.
- Drilling the Clavicle: Two holes are drilled in the distal clavicle to anatomically replicate the conoid (posteromedial) and trapezoid (anterolateral) insertions.
- Passing the Construct: A shuttle relay is used to pass the suspensory button construct through the coracoid and up through the clavicular tunnels.
- Reduction: The surgeon elevates the arm (reducing the scapula to the clavicle) while applying direct downward pressure on the distal clavicle. Once anatomic reduction is confirmed visually and fluoroscopically, the high-strength sutures are tied over the clavicular buttons.
Adjunctive Procedures
- Hook Plate Fixation: In cases of severe comminution or revision surgery, an AC hook plate may be utilized. The hook is placed under the acromion, and the plate is fixed to the clavicle. Note: Hook plates require a mandatory second surgery for removal at 3 to 4 months to prevent acromial osteolysis and rotator cuff tearing.
- Chronic Reconstructions (> 6 weeks): In chronic cases, the native ligaments will not heal. A free tendon autograft (e.g., semitendinosus) or allograft must be woven through the clavicle and under the coracoid (anatomic CC reconstruction) to provide permanent biologic stability.
Deltotrapezial Fascial Repair
The most critical step of the closure is the meticulous, heavy-suture imbrication of the deltotrapezial fascia over the distal clavicle. Failure to achieve a watertight, robust fascial repair significantly increases the risk of superior clavicular migration and construct failure.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Successful outcomes depend heavily on strict adherence to postoperative rehabilitation guidelines to protect the healing ligaments.
- Phase I (0 to 4 weeks): The patient is immobilized in a sling. Only passive range of motion (ROM) for the elbow, wrist, and hand is permitted. Pendulum exercises may begin at 3 weeks. Active shoulder elevation is strictly prohibited to prevent stress on the CC reconstruction.
- Phase II (4 to 8 weeks): The sling is discontinued. Passive and active-assisted ROM of the shoulder is initiated. Forward flexion is limited to 90 degrees, and cross-body adduction is avoided to protect the AC joint capsule.
- Phase III (8 to 12 weeks): Full active ROM is achieved. Isotonic strengthening of the rotator cuff and periscapular stabilizers (rhomboids, serratus anterior) is initiated.
- Phase IV (3 to 6 months): Advanced strengthening and sport-specific drills. Return to contact sports or heavy manual labor is generally permitted at 5 to 6 months postoperatively, provided the patient has symmetric strength and no pain.
COMPLICATIONS
Despite advanced surgical techniques, complications can occur:
1. Loss of Reduction: Often due to premature return to activity, failure of the deltotrapezial repair, or hardware pull-out through osteoporotic bone.
2. Coracoid Fracture: Can occur if the drill hole is placed eccentrically or if the coracoid is too small to accommodate the tunnels.
3. AC Joint Arthrosis: Post-traumatic arthritis is common, even in nonoperatively managed Type I and II injuries. If symptomatic, it is treated with a late distal clavicle excision (Mumford procedure).
4. Infection: Superficial and deep infections require prompt irrigation, debridement, and appropriate antibiotic therapy. Hardware retention is attempted until ligamentous healing occurs, provided the infection can be suppressed.
📚 Medical References
- Roberts SM: Acromioclavicular dislocation, Am J Surg 23:322, 1934.
- Shoulder Abbott LC, Lucas DB: The tripartite deltoid and its surgical signifi cance in exposure of the scapulohumeral joint, Ann Surg 136:392, 1952.
- Abbott LC, Lucas DB: The function of the clavicle: its surgical significance, Ann Surg 140:583, 1954.
- Abbott LC, Saunders JBDM, Hagey H, et al: Surgical approaches to the shoulder joint, J Bone Joint Surg 31A:235, 1949.
- Armstrong JR: Excision of the acromion in treatment of the supraspinatus syndrome: report of ninety-five excisions, J Bone Joint Surg 31B:436, 1949.
- Bennett GE: Shoulder and elbow lesions of professional baseball pitcher, JAMA 117:510, 1941.
- Brodsky JW, Tullos HS, Gartsman GM: Simplified posterior approach to the shoulder joint: a technical note, J Bone Joint Surg 71A:407, 1989.
- Codman EA: Obscure lesions of the shoulder: rupture of the supraspinatus tendon, Boston Med Surg J 196:381, 1927.
- Cubbins WR, Callahan JJ, Scuderi CS: The reduction of old or irreducible dislocations of the shoulder joint, Surg Gynecol Obstet 58:129, 1934.
- Darrach W: Surgical approaches for surgery of the extremities, Am J Surg 67:237, 1945.
- Harmon PH: A posterior approach for arthrodesis and other operations on the shoulder, Surg Gynecol Obstet 81:266, 1945.
- Henry AK: Exposures of long bones and other surgical methods, Bristol, England, 1927, John Wright & Sons. Kocher T: Textbook of operative surgery , 3rd ed, London, 1911, Adam & Charles Black (Translated by HJ Stiles, CB Paul). Kuz JE, Pierce TD, Braunohler WB: Coronal transacromial osteotomy surgical approach for
You Might Also Like
