ABOS Part I & AAOS OITE Orthopaedic Surgery Review: Clinical Cases & Exam Questions | Part 22139
Key Takeaway
ABOS Part I Review modules offer advanced orthopedic multiple-choice questions mirroring the ABOS Part I and AAOS OITE examinations. Content is derived from high-yield clinical teaching cases, covering essential topics like shoulder dislocations, fracture fixation principles, and orthopedic screw biomechanics to ensure comprehensive exam preparation.
ABOS Part I & AAOS OITE Orthopaedic Surgery Review: Clinical Cases & Exam Questions | Part 22139
A 24-year-old male presents to the emergency department after a football injury, complaining of severe right shoulder pain. His arm is held in slight abduction and external rotation. On inspection, the anterior aspect of his shoulder appears prominent, and there is a palpable void beneath the acromion. Which of the following physical exam findings is MOST concerning for an associated neurovascular injury in this patient?
Correct Answer: D
An absent radial pulse is a critical finding indicating potential compromise of the brachial artery, which is a surgical emergency. While axillary nerve injury (loss of sensation over the lateral deltoid, weakness in abduction) is the most common nerve injury with anterior shoulder dislocations, it is rarely an acute limb-threatening condition unless it's a traction injury without spontaneous recovery. Weakness in wrist extension would suggest radial nerve involvement, which is less common. Ecchymosis is a common finding but not acutely life- or limb-threatening.
A 35-year-old patient presents with a history of recurrent anterior shoulder dislocations. During your examination, you perform the Apprehension Test. Which of the following describes a positive test?
Correct Answer: A
The Apprehension Test is performed by abducting the shoulder to 90 degrees and slowly externally rotating the arm. A positive test is indicated by the patient's feeling of impending dislocation (apprehension) or significant pain, often due to stretching of the anterior capsule. Options B and C describe findings related to rotator cuff or glenohumeral arthritis. Option D describes the Sulcus Sign, indicative of inferior or multidirectional instability. Option E describes a clunk, which could be related to labral pathology but is not the apprehension test.
A 50-year-old patient presents with acute shoulder pain after a seizure. On examination, the arm is held in internal rotation, and the anterior shoulder appears flattened. External rotation is severely restricted. Which radiographic finding on an AP shoulder view is pathognomonic for a posterior shoulder dislocation?
Correct Answer: C
The Trough line sign (or reverse Hill-Sachs lesion) is an impaction fracture on the anterior-medial aspect of the humeral head, often seen with posterior dislocations. The other options are incorrect: Hill-Sachs and Bankart lesions are typically associated with anterior dislocations. HAGL lesions are avulsions of the glenohumeral ligaments, often associated with anterior dislocations. Os acromiale is an anatomical variant.
During the examination of a patient with suspected shoulder dislocation, you note a sulcus sign. What does this finding MOST commonly indicate?
Correct Answer: C
The Sulcus Sign is elicited by applying inferior traction to the arm, causing a dimple or sulcus to appear below the acromion. It is indicative of inferior capsular laxity and is a hallmark of inferior or multidirectional glenohumeral instability. While multidirectional instability often includes an inferior component, the most direct interpretation of a sulcus sign is inferior instability.
A 68-year-old woman falls directly onto her shoulder. She presents with severe pain and an inability to move her arm. On exam, the shoulder appears abducted, and a prominent hard mass is palpable inferior to the glenoid, consistent with a Luxatio Erecta. Which neurovascular structure is at highest risk of injury in this type of dislocation?
Correct Answer: C
Luxatio Erecta (inferior dislocation) involves extreme abduction, forcing the humeral head inferiorly. The head can impinge upon or stretch the neurovascular bundle in the axilla. The axillary artery is at significant risk due to its proximity and the severe displacement. While the axillary nerve and brachial plexus are also at risk, arterial compromise (axillary artery) is a more acute and limb-threatening complication associated with the extreme force and direction of displacement in luxatio erecta, often leading to intimal tears or thrombosis.
Following reduction of an anterior shoulder dislocation, a patient complains of persistent weakness in active shoulder abduction. Sensation over the lateral aspect of the deltoid is intact. Which of the following is the MOST likely cause of this isolated weakness?
Correct Answer: B
If sensation over the lateral deltoid (axillary nerve sensory distribution) is intact, persistent isolated weakness in shoulder abduction, especially in an older patient or high-energy trauma, should raise suspicion for an associated rotator cuff tear (supraspinatus or deltoid dysfunction). Axillary nerve neuropraxia would typically present with sensory deficits in addition to motor weakness. Musculocutaneous nerve injury affects biceps and coracobrachialis, and lateral forearm sensation. Long thoracic nerve injury causes scapular winging. Brachial plexus avulsion would present with more widespread neurological deficits.
A 22-year-old male presents with his first-time anterior shoulder dislocation. During the initial assessment, which of the following is a critical component of the examination PRIOR to any reduction attempts?
Correct Answer: C
A thorough neurovascular examination of the affected extremity, including palpation of pulses and assessment of sensation and motor function, is paramount before any reduction attempts. This establishes a baseline and helps identify any pre-existing or acute neurovascular compromise that could be exacerbated by or misattributed to the reduction maneuver. Analgesia is important but secondary to neurovascular assessment. Contralateral shoulder ROM is not critical pre-reduction. Ice is for comfort. Family history is irrelevant in acute management.
You are examining a patient with a suspected posterior shoulder dislocation. Which maneuver is most likely to confirm your suspicion on physical exam?
Correct Answer: C
Posterior dislocations classically present with the arm held in internal rotation and adduction, with a significant block to external rotation. The anterior shoulder may appear flattened, and the coracoid process prominent. Apprehension with abduction and external rotation is characteristic of anterior instability. Limited internal rotation with intact external rotation is incorrect. Increased superior translation with anterior force is not directly indicative of posterior dislocation. A palpable defect below the coracoid is more suggestive of anterior dislocation.
Which finding on a post-reduction physical exam of an anterior shoulder dislocation indicates successful reduction and suggests stability?
Correct Answer: B
Successful reduction is indicated by the restoration of normal shoulder contour (loss of the anterior prominence of the humeral head), relief of severe pain, and the ability to achieve full or near-full passive range of motion without a 'block.' Persistent apprehension or instability signs (like a sulcus sign or continued apprehension with external rotation) suggest potential underlying pathology or incomplete reduction. Crepitus might indicate cartilage damage, and inability to actively abduct could suggest a rotator cuff tear or nerve injury, not necessarily unsuccessful reduction.
A 70-year-old male sustains an anterior shoulder dislocation. After reduction, plain radiographs show a concomitant fracture. Which fracture is MOST commonly associated with anterior shoulder dislocation in this age group?
Correct Answer: B
While Hill-Sachs and Bankart lesions are very common with anterior dislocations, in older patients, a greater tuberosity fracture is particularly common (up to 30% in some series) due to the weaker bone and the forces involved in the injury. The rotator cuff avulses a piece of the tuberosity during the dislocation. Surgical neck fracture is also possible but less frequent than greater tuberosity in direct association with dislocation. Clavicle fractures are less directly associated with glenohumeral dislocation mechanism.
A resident is reviewing the basic anatomy of an orthopedic screw. Referring to the provided image, which labeled component is primarily responsible for providing a smooth, unthreaded link between the screw head and the threaded portion?
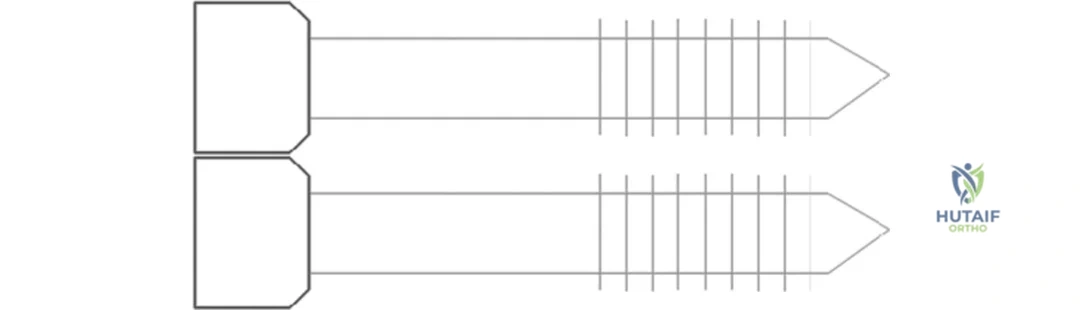
Correct Answer: B
The case explicitly states, 'The shank provides a smooth link between the head and thread.' The image clearly labels the shank as the unthreaded portion immediately distal to the head. The head (A) provides a connection for a screwdriver and prevents sinking. The thread (C) engages with the bone. Pitch (D) is the distance between adjacent threads. Flutes (E) provide a route for bone debris removal.
A 68-year-old female with osteoporotic bone requires internal fixation for a distal femur fracture. To maximize the pull-out strength of the screws in this challenging bone quality, which of the following biomechanical principles should the surgeon prioritize?
Correct Answer: C
The case states that pull-out strength can be increased by 'increasing thread density' or by having a 'finer' pitch, which allows more turns of the spiral thread to engage in a given depth of cortex, creating greater resistance to pull-out. Options A and B would decrease the contact surface area or thread depth, thereby reducing pull-out strength. Option D directly contradicts the principle of increasing engaged threads. Option E (larger pilot hole) is a surgeon factor that reduces pull-out strength.
During a complex ankle fracture fixation, a junior resident inadvertently makes a pilot hole slightly larger than recommended for the chosen screw. This technical error is most likely to result in which of the following?
Correct Answer: C
The case explicitly lists 'making too large a pilot hole' as a surgeon factor that can reduce screw pull-out strength. A larger pilot hole reduces the contact area between the screw threads and the bone, diminishing the frictional and mechanical interlock necessary for strong fixation. Options A, B, D, and E are incorrect as a larger pilot hole would generally weaken the fixation, not strengthen it or improve insertion characteristics in a beneficial way.
A surgeon is selecting a screw for metaphyseal fixation in a comminuted proximal humerus fracture, where bone quality may be compromised. To optimize the screw's resistance to axial dislodgement, which characteristic related to the screw's thread design would be most beneficial?
Correct Answer: C
The case states, 'The 'finer' the pitch, the more turns of the spiral thread engage in a given depth of cortex, creating greater resistance to pull-out.' A finer pitch means more threads per unit length, increasing the contact surface area with the bone. A larger lead (A) or coarser pitch (B) would mean fewer threads engaged. A shallower thread depth (D) or smaller outer diameter (E) would reduce the contact surface area, thereby decreasing pull-out strength.
In a scenario where a surgeon aims to maximize the pull-out strength of a non-locking screw in cortical bone, which combination of screw diameter characteristics would be most advantageous?
Correct Answer: C
The case indicates that pull-out strength can be increased by 'increasing the contact surface area between screw threads and bone, either by increasing the outer diameter, decreasing the core diameter.' This combination (increased outer diameter and decreased core diameter) results in a greater thread depth, maximizing the volume of bone engaged by the screw threads and thus increasing the resistance to pull-out. Options A, B, and D would either reduce the thread depth or the overall screw-bone contact. Option E describes a smooth pin, not a screw.
A 55-year-old male sustains a periprosthetic femur fracture around a total hip arthroplasty stem. The surgeon opts for plate and screw fixation. The use of locking screws in this context primarily enhances stability by:
Correct Answer: B
The case states, 'The use of a locking screw can also create a monobloc effect for greater stability.' Locking screws thread into the plate, creating a fixed-angle construct that acts as a single unit (monobloc) with the bone, providing enhanced stability, especially in osteoporotic bone or comminuted fractures. They do not primarily rely on screw-plate friction (A) or provide dynamic compression (C) in the same way non-locking screws do. They increase, rather than reduce, the stiffness of the construct (D). Flutes, not locking screws, facilitate bone debris removal (E).
During a revision surgery for a failed ankle fusion, a surgeon attempts to re-insert a screw into a previously drilled hole. After initial resistance, the screw feels loose and does not achieve adequate purchase. This situation is most likely due to:
Correct Answer: C
The case identifies 'repeated withdrawal and reintroduction of a screw causing damage to the negative threads in the bone tissue' as a surgeon factor that can reduce screw pull-out strength. When a screw is removed and reinserted, the bone threads (negative threads) can be stripped or damaged, leading to poor purchase and reduced pull-out strength upon reinsertion. Insufficient pilot hole depth (A) would typically lead to difficulty inserting the screw initially, not looseness after reinsertion. Over-tightening (B) could strip the threads on the first attempt, but the scenario describes re-insertion. An excessively fine pitch (D) would increase pull-out strength, not decrease it. The type of screw (E) is not the primary cause of this specific failure mode.
A biomechanical engineer is testing various orthopedic screw designs. The primary parameter being measured when assessing a screw's "pull-out strength" is the:
Correct Answer: C
The case clearly defines pull-out strength: 'A screw's pull-out strength refers to the axial force required to remove a screw from bone.' Options A, B, D, and E describe other mechanical properties of screws (torsional strength, bending strength, fatigue strength, compressive strength) but not specifically pull-out strength, which is a measure of resistance to axial extraction.
A 72-year-old patient with severe osteoporosis undergoes open reduction and internal fixation of a proximal tibia fracture. The surgeon is particularly concerned about screw pull-out. Which of the following intraoperative strategies would provide the greatest cumulative benefit in maximizing screw pull-out strength in this patient?
Correct Answer: B
This option combines multiple strategies mentioned in the case to maximize pull-out strength. The case states that pull-out strength can be increased by 'increasing the number of threads engaged in the bone cortex' and by using a 'finer' pitch. An undersized pilot hole (the opposite of 'too large a pilot hole' which reduces strength) would maximize thread purchase. Option A describes characteristics that would decrease pull-out strength (larger core, coarser pitch). Option C suggests avoiding locking screws, which the case states 'create a monobloc effect for greater stability,' and micro-motion is generally undesirable for fixation. Option D (repeated insertion/removal) is explicitly listed as a factor that reduces pull-out strength. Option E (smaller outer diameter, larger lead) would reduce thread engagement and pull-out strength.
Referring to the provided image, the component labeled 'Depth' is crucial for a screw's pull-out strength. According to the case, how does the 'Depth' of a screw thread primarily contribute to its resistance against axial removal from bone?
Correct Answer: B
The case states, 'the depth determines the amount of contact with bone for resistance to pull-out.' A greater thread depth allows for more bone engagement and thus a larger contact surface area, which directly increases pull-out strength. Option A describes the lead. Option C describes the function of flutes. Option D describes the pitch. Option E describes the shank.
A 45-year-old male sustains a comminuted mid-shaft femoral fracture (OTA/AO 32-C3) in a high-energy trauma. He is hemodynamically stable. Which of the following is the most appropriate initial surgical approach concerning reaming?
Correct Answer: C
For a hemodynamically stable patient with a comminuted mid-shaft femoral fracture, immediate reamed intramedullary nailing is generally the preferred approach. Reaming clears the medullary canal, allowing for a larger diameter nail, which provides greater bending and torsional stiffness, leading to superior biomechanical stability and higher rates of union. While unreamed nailing might be considered in polytrauma patients who are unstable or have significant pulmonary compromise to reduce the risk of fat embolism, a stable patient benefits from reamed nailing. Staged procedures are often reserved for patients who are initially unstable. External fixation is typically a temporizing measure. Percutaneous plating is not the standard of care for a comminuted mid-shaft femoral fracture due to inferior load-sharing capabilities compared to IM nailing.
Regarding the entry point for an antegrade femoral intramedullary nail, which statement is most accurate to prevent iatrogenic injury?
Correct Answer: A
While both piriformis fossa and trochanteric entry points are utilized, the piriformis fossa entry point, when properly executed, is considered to minimize the risk of avascular necrosis of the femoral head by avoiding excessive penetration into the vascular watershed area of the superior retinacular vessels. However, it can be technically challenging and increase the risk of gluteal muscle damage. A trochanteric tip entry point may risk damage to the gluteus medius and piriformis tendons and can lead to lateral hip pain. A medial-based trochanteric entry point is more likely to cause iatrogenic fracture of the greater trochanter or varus malalignment due to impingement. The size of the nail is determined by the medullary canal, not the entry point directly. Hip pain is often multifactorial but can be higher with more lateral entry points.
What is the primary biomechanical advantage of reamed compared to unreamed intramedullary nailing for diaphyseal fractures?
Correct Answer: B
The primary biomechanical advantage of reamed intramedullary nailing is the ability to use a larger diameter nail. This significantly increases the nail's moment of inertia, which dramatically improves its bending and torsional stiffness. This enhanced stability is crucial for fracture healing, especially in comminuted or unstable fractures. While reaming does increase intramedullary pressure and transiently disrupts the endosteal blood supply, the long-term benefit of superior stability often outweighs these initial concerns. Reduced thermal necrosis is incorrect, as reaming generates heat. Faster insertion time is not a primary biomechanical advantage, and reaming typically increases insertion time. Preservation of endosteal vascularity is generally better with unreamed nailing.
When performing antegrade humeral intramedullary nailing, which specific nerve is most at risk during the proximal locking screw placement?
Correct Answer: A
During proximal locking screw placement for an antegrade humeral intramedullary nail, the axillary nerve is most vulnerable. It courses around the surgical neck of the humerus, deep to the deltoid, and is susceptible to injury, particularly with excessively long screws or imprecise drilling techniques in the superolateral aspect of the proximal humerus. The radial nerve is at risk more distally, especially with distal locking or in the spiral groove. The ulnar, musculocutaneous, and median nerves are typically not at high risk with proximal humeral locking screws.
A 30-year-old male sustains an open Gustilo-Anderson Type IIIA tibia fracture. After debridement and irrigation, the most appropriate definitive fixation method is:
Correct Answer: D
For open Gustilo-Anderson Type IIIA tibia fractures, immediate unreamed intramedullary nailing, after thorough debridement and irrigation, is generally considered the preferred definitive fixation method. Unreamed nailing reduces the theoretical risk of disseminating contaminants into the medullary canal compared to reamed nailing, while still providing stable fixation and promoting early weight-bearing. Reamed nailing in an open fracture setting carries a higher theoretical risk of infection. External fixation is often a temporizing measure for more severe open fractures (e.g., Type IIIB/C) or when soft tissue coverage is an immediate concern, but definitive IM nailing is superior for union rates and function. Plate fixation has higher infection rates in open tibia fractures. Casting is insufficient for an open, unstable tibia fracture.
Which of the following conditions is considered a relative contraindication to reamed intramedullary nailing?
Correct Answer: D
Severe pulmonary compromise, such as Acute Respiratory Distress Syndrome (ARDS), is a relative contraindication to reamed intramedullary nailing. Reaming can lead to increased intramedullary pressure, release of fat emboli, and inflammatory mediators into the systemic circulation, which can exacerbate existing pulmonary issues. In such cases, unreamed nailing or external fixation might be preferred. Age and obesity are not contraindications per se, though they can pose technical challenges. Active systemic infection is generally a contraindication to any implant surgery. Polytrauma with an ISS < 16 is typically not a contraindication, and IM nailing is often beneficial in these patients.
What is the primary role of static locking in intramedullary nailing?
Correct Answer: B
Static locking, achieved by placing locking screws both proximally and distally, is primarily used to prevent shortening and rotational instability of the fracture. This is particularly important in unstable or comminuted fractures where axial loading might otherwise lead to collapse. While some controlled micromotion is desirable for callus formation, static locking aims to control excessive motion. Dynamization (removing one set of locking screws) is done to achieve compression, which is the opposite of the initial goal of static locking. Static locking does not inherently reduce implant fatigue failure more than dynamic locking, as fatigue is often due to micromotion. Bending stiffness is generally high with IM nails, and static locking maintains length and rotation, not primarily enhancing bending stiffness over dynamic locking.
A patient with a comminuted subtrochanteric femur fracture (AO/OTA 32-C1) is treated with a long cephalomedullary nail. Which reduction maneuver is often necessary to achieve adequate alignment before nail insertion?
Correct Answer: D
Subtrochanteric fractures are notoriously difficult to reduce due to the strong deforming forces of the hip musculature (iliopsoas, gluteus medius/minimus, adductors). A femoral distractor or manual traction is often necessary to overcome the powerful adductor spasm and length discrepancy, allowing for proper reduction. Once length is restored, other maneuvers may be needed for rotational and angular control. Knee flexion is more relevant for distal femur fractures (gastrocsoleus pull). External rotation is often the deformity, so internal rotation may be needed. Direct manipulation with a Schanz pin can aid, but overcoming severe shortening/displacement usually requires traction first. Axial compression before achieving length and alignment is counterproductive.
What is the most common iatrogenic complication associated with a piriformis fossa entry point for femoral intramedullary nailing?
Correct Answer: A
The most common iatrogenic complication associated with a piriformis fossa entry point is postoperative hip pain, often attributed to gluteal tendon irritation or heterotopic ossification (HO) in the gluteal region. While avascular necrosis of the femoral head is a theoretical concern with excessive penetration or damage to the retinacular vessels, it is less common than hip pain/HO. Greater trochanteric fracture is more associated with a lateral entry point. Damage to the superior gluteal neurovascular bundle is possible but less frequent than HO. Varus malunion is more related to an excessively medial entry point or improper reduction, rather than the piriformis fossa specifically.
A patient undergoes IM nailing for a femoral shaft fracture. Postoperatively, they develop chest pain, dyspnea, and petechial rash. Which complication is most likely?
Correct Answer: C
The classic triad of symptoms – respiratory distress, neurological dysfunction, and a petechial rash – following long bone fracture fixation (especially IM nailing) is highly indicative of Fat Embolism Syndrome (FES). The pathophysiology involves the release of marrow fat into the circulation, leading to mechanical obstruction and inflammatory response in the lungs and other organs. While pulmonary embolism is a possibility after any surgery, the presence of the petechial rash makes FES the more likely diagnosis. Pneumonia and AMI would present differently, and ARDS is a potential severe manifestation of FES but FES is the primary diagnosis here.
Which of the following vascular injuries is most commonly associated with this specific dislocation pattern?
Based on modern anatomic perfusion studies, which vessel provides the predominant blood supply to the humeral head that is at risk in complex proximal humerus fractures?
None
