Pediatric Traumatic Hip Dislocations & SCFE: Surgical Guide
Key Takeaway
Pediatric traumatic hip dislocations and slipped capital femoral epiphysis (SCFE) require prompt, evidence-based intervention to prevent devastating complications like osteonecrosis. This comprehensive guide details the biomechanics, clinical evaluation, and step-by-step surgical management of these conditions. Emphasizing precise reduction techniques, optimal surgical approaches, and rigorous postoperative protocols, it provides orthopedic surgeons with the critical knowledge necessary to achieve congruous joint reduction and preserve long-term hip function in the growing child.
TRAUMATIC HIP DISLOCATIONS IN CHILDREN
Traumatic hip dislocations in the pediatric population are exceedingly rare, yet they occur with greater frequency than pediatric hip fractures. The management of these injuries requires a profound understanding of the unique biomechanical properties of the immature skeleton, meticulous clinical evaluation, and precise surgical execution to prevent catastrophic long-term sequelae, most notably osteonecrosis of the femoral head.
Epidemiology and Biomechanics
The threshold for dislocation in a young child is significantly lower than in an adult. Trivial injuries or low-energy trauma can precipitate a complete hip dislocation primarily because the pediatric articular cartilage is highly pliable and the capsuloligamentous structures are inherently lax.
Historically, the age distribution of these injuries has been a subject of academic debate. MacFarlane originally noted that approximately 50% of pediatric hip dislocations occurred in adolescents between the ages of 12 and 15 years. However, subsequent large-scale reviews by Gartland and Brenner demonstrated a relatively equal age distribution across 248 patients. More contemporary literature, including pivotal studies by Libri et al. and Hamilton and Broughton, suggests a distinct bimodal distribution. Their cohorts fell into two distinct demographic peaks:
* Early Childhood (2 to 5 years old): Dislocations typically result from low-energy, trivial trauma due to maximum ligamentous laxity and cartilaginous pliability.
* Adolescence (11 to 15 years old): Dislocations in this cohort mirror adult mechanisms, typically requiring high-energy trauma (e.g., motor vehicle collisions, high-impact sports).
Consistent with adult trauma patterns, posterior dislocations are markedly more common than anterior dislocations in all pediatric age groups.
Prognostic Factors and Complications
The ultimate functional outcome and survivorship of the native hip joint following a traumatic dislocation depend on several critical variables. Orthopedic surgeons must evaluate these seven primary prognostic factors:
- Severity of the Initial Injury: High-energy trauma correlates with a higher incidence of concomitant chondral damage and capsular stripping.
- Interval Between Injury and Reduction: Time is joint cartilage. Reduction must be performed emergently (ideally within 6 hours) to decompress the intracapsular vessels and minimize the risk of avascular necrosis (AVN).
- Type of Treatment: The choice between closed versus open reduction, dictated by post-reduction congruity.
- Period of Non–Weight Bearing: Adequate protection of the vulnerable chondral surfaces during the acute inflammatory phase.
- Development of Recurrent Dislocation: Indicative of severe capsulolabral incompetence or unrecognized bony avulsions.
- Development of Osteonecrosis: The most devastating complication, directly linked to the duration of ischemia and initial trauma severity.
- Incomplete Reduction: Often caused by the intra-articular interposition of soft tissue (e.g., inverted limbus, capsule) or osteochondral fragments.
Clinical Pearl: Price et al. emphasized that hip dislocations presenting with spontaneous incomplete reduction are highly suspicious for interposed structures. Never accept an incongruous joint space on post-reduction imaging.
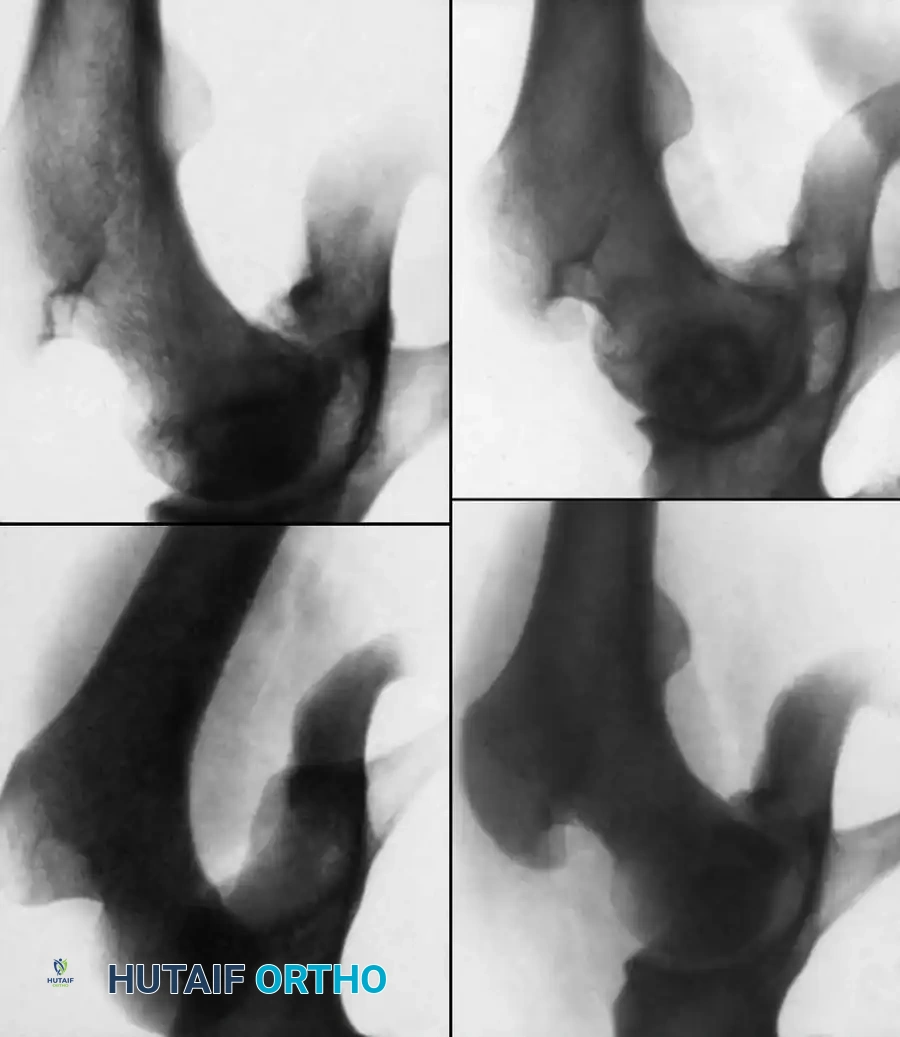
Fig. 33-125 Osteonecrosis of the femoral head after hip dislocation. A, Traumatic dislocation in an older child. B, After satisfactory closed reduction. C, At 1 year after reduction, suggestion of early osteonecrosis. D, At 8 years after reduction, cystic appearance of osteonecrosis.
Evaluation of Reduction Congruity
Following a closed reduction under general anesthesia, meticulous radiographic evaluation is mandatory. The surgeon must scrutinize the anteroposterior (AP) pelvis and cross-table lateral radiographs.
An incongruous reduction is diagnosed when there is:
* Asymmetry or widening of the medial joint space (teardrop distance) compared to the contralateral normal hip.
* A break in Shenton's line.
* Failure of the femoral head to seat concentrically within the acetabular fossa.

Fig. 33-126 Incongruous reduction of hip. Radiograph of both hips after what was thought to be successful closed reduction of traumatic dislocation of the right hip in adolescent. Reduction is incongruous, however, as shown by break in Shenton line and increase in width of joint space.
If plain radiographs are equivocal, or if an incongruous reduction is identified, a computed tomography (CT) scan is the gold standard to identify the offending intra-articular material, such as an osteocartilaginous fragment or an avulsed ligamentum teres.
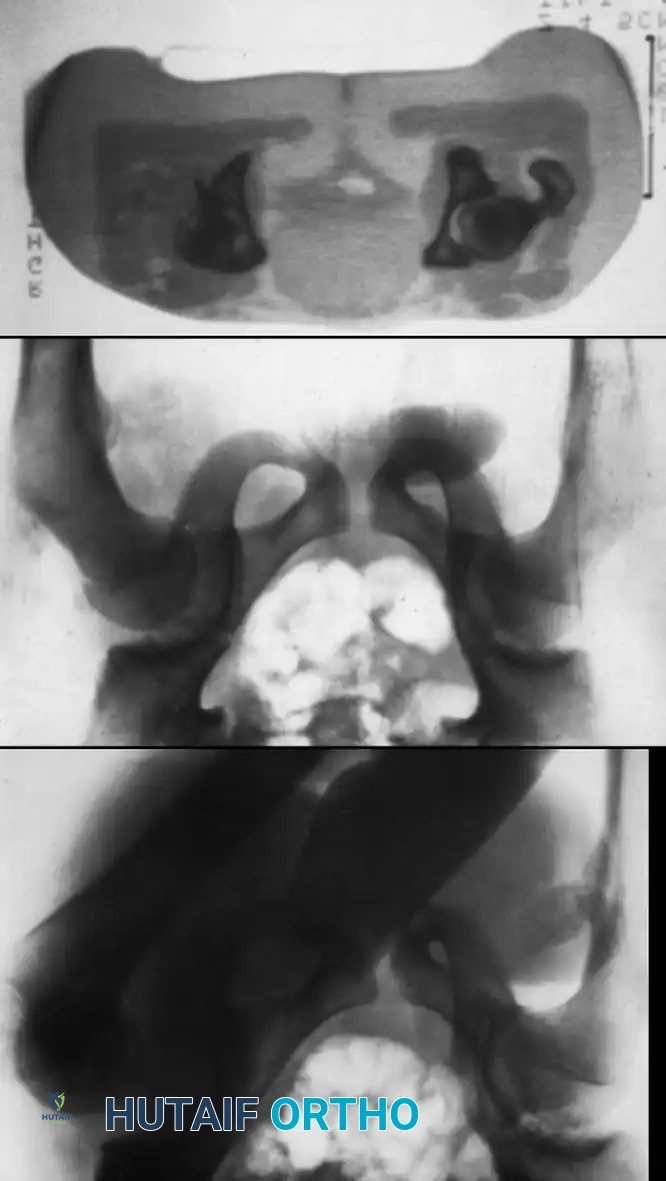
Fig. 33-127 Incongruous reduction of hip. A, Traumatic hip dislocation in adolescent. B, After two attempts at closed reduction, joint space is still too wide and Shenton line is broken. C, CT scan shows osteocartilaginous fragment in acetabulum impeding reduction; open reduction was necessary.
Surgical Management: Open Reduction Techniques
When closed reduction fails to achieve a perfectly congruous joint, emergent open reduction is indicated to extract the offending material and restore joint anatomy.
Selection of the Surgical Approach
The surgical approach is dictated by the direction of the dislocation:
* Posterior Dislocations: A posterior approach, such as a modified Gibson or Moore approach, is utilized.
* Anterior Dislocations: An anterior approach, such as the Smith-Petersen approach, is required.
* Unknown Direction: If the initial direction of dislocation cannot be definitively determined (e.g., spontaneous partial reduction prior to arrival), a posterior approach is the default, as posterior dislocations are statistically far more common.
Step-by-Step Open Reduction (Posterior Approach)
- Positioning: Place the patient in the lateral decubitus position on a radiolucent table. Ensure secure pelvic positioning to allow for intraoperative fluoroscopy.
- Incision (Modified Gibson): Make a curvilinear incision starting proximal to the greater trochanter, extending distally along the posterior border of the greater trochanter, and continuing along the femoral shaft.
- Superficial Dissection: Incise the fascia lata in line with the skin incision. Proximally, split the gluteus maximus bluntly in line with its fibers to expose the short external rotators.
- Deep Dissection & Nerve Protection: Identify and meticulously protect the sciatic nerve, which may be displaced or draped over the dislocated femoral head.
- Capsulotomy and Joint Inspection: Tag and release the piriformis and obturator internus tendons at their insertion. Perform a T-shaped or I-shaped capsulotomy.
- Debridement: The hip should be gently redislocated to allow full visualization of the acetabulum. Systematically inspect for and remove loose bony fragments, osteochondral shear injuries, an inverted acetabular labrum (limbus), or a hypertrophic/avulsed ligamentum teres.
- Reduction and Confirmation: Gently reduce the hip. Confirm concentric reduction visually and radiographically in the operating room, ensuring the joint space width has returned to absolute normal.
- Closure: Repair the capsule meticulously to restore posterior stability, followed by the reattachment of the short external rotators.
Surgical Warning: Occasionally, an ipsilateral femoral fracture occurs simultaneously with a hip dislocation. This complex injury pattern requires specialized management, typically involving temporary stabilization of the femur to allow for controlled manipulation and reduction of the hip joint, followed by definitive fixation of the fracture.
Arthroscopic Alternatives
With advancements in pediatric hip arthroscopy, minimally invasive techniques are becoming viable for specific indications. Kashiwagi et al. described the successful arthroscopic excision of an avulsed ligamentum teres (presenting as an osteochondral fragment) that was causing an incongruous reduction in a 10-year-old child. Arthroscopy offers the advantage of minimal soft-tissue morbidity but requires advanced technical proficiency and is contraindicated if there is a risk of fluid extravasation into the retroperitoneum or fascial compartments.
SLIPPED CAPITAL FEMORAL EPIPHYSIS (SCFE)
While traumatic hip dislocations represent acute mechanical failures, Slipped Capital Femoral Epiphysis (SCFE) represents a complex interplay of mechanical, endocrine, and anatomical vulnerabilities leading to the displacement of the proximal femoral epiphysis.
Pathophysiology and Demographics
It is critical to differentiate SCFE from Type I transepiphyseal separations.
* Type I Transepiphyseal Separations: Generally caused by high-energy trauma and are most common in very young children.
* SCFE: Occurs insidiously. Minor trauma can precipitate an acute separation or exacerbate a chronic slip.
SCFE occurs in a distinct, older demographic, typically between the ages of 10 and 16 years. Strikingly, 78% of patients with SCFE are adolescents undergoing the rapid pubertal growth spurt.
Epidemiological Risk Factors:
* Obesity: The most significant mechanical risk factor.
* Sex: Almost twice as common in boys as in girls.
* Race: Occurs approximately twice as often in Black children compared to White children.
* Laterality: The left hip is affected twice as often as the right.
* Bilateral Involvement: Reported in 25% to 40% of children. When bilateral slips occur, the contralateral slip usually manifests within 12 to 18 months of the initial presentation.
Etiology and Endocrine Associations
The etiology of SCFE is multifactorial. A physis weakened by an underlying systemic condition fails when subjected to physiological or slightly supranormal stresses. Suggested etiological factors include:
* Local trauma and mechanical overload (obesity).
* Growth spurts and pubertal hormonal surges.
* Inflammatory conditions.
* Genetic factors and Down syndrome.
* Seasonal variations.
Endocrine Disorders:
Endocrine abnormalities must be suspected in patients presenting outside the typical age range (under 10 or over 16 years) or in those with extremely low body weight. Loder, Wittenberg, and DeSilva conducted a landmark review of 85 children with endocrine disorders and SCFE, finding that 40% had hypothyroidism and 25% had growth hormone deficiencies. Other associated conditions include hypopituitarism and chronic renal disease (renal osteodystrophy).
Biomechanics of the Slip
The pathomechanics of SCFE involve a failure through the hypertrophic zone of the physis.
* Shear Forces: Traditionally cited as the primary causative factor due to the increasing obliquity of the physis during the adolescent growth spurt combined with increased body mass.
* Torsional Forces: Aronson and Tursky suggested that torsional forces play a highly significant role. In their study of 15 acute slips, torsion was the primary force in six cases. Furthermore, in all 15 cases, internal rotation or torsion was mechanically necessary to achieve reduction, highlighting the rotational instability inherent in the pathology.
Futami et al. provided direct intra-articular evidence supporting a traumatic pathomechanism. Through arthroscopic examination of five children prior to SCFE treatment, they consistently identified:
1. Erosion of the anterosuperior articular cartilage.
2. Damage to the posterolateral acetabular labrum.
3. Cartilaginous erosion and a transverse cleft on the anterior surface of the femoral head.
Clinical Presentation and Diagnostic Pitfalls
The clinical symptoms and radiographic signs of SCFE vary depending on whether the slip is acute, chronic, or acute-on-chronic.
Classic Symptoms:
* Pain localized to the groin or medial thigh.
* Limitation of hip motion, particularly internal rotation, abduction, and flexion.
* Obligate External Rotation: A hallmark clinical sign where the affected leg externally rotates as the hip is passively flexed into a frog-leg position.
Diagnostic Pitfall: SCFE frequently presents as isolated knee pain. Matava et al. noted that patients with SCFE whose chief complaint was distal thigh or knee pain (referred pain via the obturator nerve) were significantly more likely to experience a misdiagnosis, delayed diagnosis, and undergo unnecessary radiographic evaluations of the knee. SCFE must be suspected in any patient aged 10 to 16 complaining of vague knee pain.
Signs of Chronic Slips:
Patients presenting with chronic slips may exhibit:
* Mild to moderate shortening of the affected extremity.
* The leg held in fixed external rotation.
* A positive Trendelenburg sign and antalgic or abductor lurch gait due to altered abductor mechanics and shortening of the articular-trochanteric distance.
Principles of Surgical Management for SCFE
The primary goal of SCFE treatment is to prevent further slippage and promote premature closure of the proximal femoral physis, thereby stabilizing the hip while minimizing the risks of osteonecrosis and chondrolysis.
In Situ Fixation:
The gold standard for stable SCFE is in situ fixation using a single, large-diameter cannulated screw.
1. Positioning: The patient is placed supine on a fracture table. Gentle traction may be applied, but forceful closed reduction is strictly contraindicated as it exponentially increases the risk of AVN by stretching the already tenuous retinacular vessels.
2. Trajectory: Under biplanar fluoroscopy, the screw is introduced from the anterior aspect of the proximal femur. The goal is a "center-center" position—the screw should sit in the center of the epiphysis on both the AP and lateral radiographic views.
3. Joint Penetration Avoidance: The surgeon must utilize the "approach-withdrawal" phenomenon on live fluoroscopy, rotating the hip through a full arc of motion to ensure the screw tip has not penetrated the subchondral bone into the joint space, which would precipitate devastating chondrolysis.
For unstable SCFE (where the patient cannot bear weight even with crutches), the risk of AVN is significantly higher (up to 50%). Management may involve gentle, incidental reduction resulting from positioning on the fracture table, followed by urgent capsulotomy to decompress the intracapsular hematoma, and subsequent stable fixation.
Conclusion
Both traumatic pediatric hip dislocations and SCFE represent critical orthopedic conditions that demand a high index of suspicion, rapid diagnostic imaging, and precise surgical intervention. Whether executing a meticulous open reduction for an incongruous traumatic dislocation or performing precise in situ pinning for a slipped epiphysis, the surgeon's overarching mandate is the preservation of the delicate epiphyseal blood supply and the restoration of joint congruity to ensure the long-term viability of the pediatric hip.
You Might Also Like


