Slipped Capital Femoral Epiphysis: Comprehensive Surgical Management
Key Takeaway
Slipped Capital Femoral Epiphysis (SCFE) is a critical pediatric hip disorder characterized by the displacement of the proximal femoral epiphysis. This comprehensive guide details the evidence-based management of SCFE, emphasizing the Loder stability classification, precise radiographic evaluation, and the gold-standard percutaneous single-screw in situ fixation technique. Key focus is placed on optimizing fluoroscopic positioning, avoiding devastating complications like osteonecrosis and chondrolysis, and ensuring optimal long-term hip biomechanics.
Comprehensive Introduction and Patho-Epidemiology
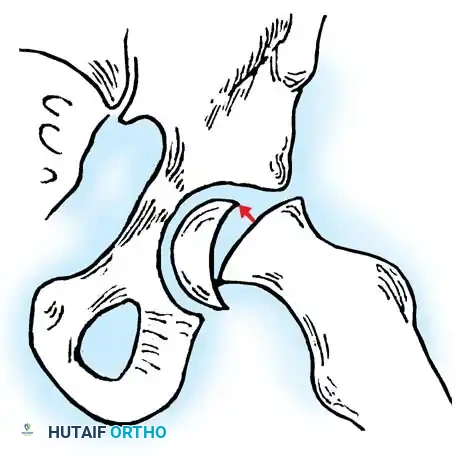
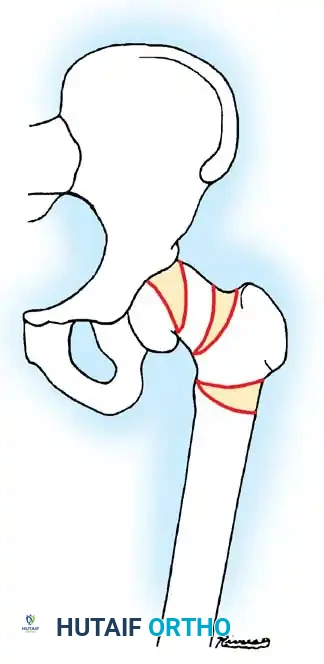
Slipped Capital Femoral Epiphysis (SCFE) represents a unique, profoundly complex, and biomechanically devastating pediatric hip disorder if left untreated. While technically classified as a type I transepiphyseal fracture-separation through the hypertrophic zone of the proximal femoral physis, SCFE is distinguished from standard traumatic epiphyseal separations by its distinct natural history, insidious pathogenesis, and multifactorial etiology. The disorder is strictly characterized by the displacement of the proximal femoral epiphysis posteriorly and inferiorly relative to the femoral neck, creating a three-dimensional deformity that alters the hip's fundamental kinematics.
The epidemiology of SCFE is closely tied to the physiological changes of adolescence. It is the most common hip disorder in adolescents, with an overall incidence ranging from 0.2 to 10 per 100,000 depending on geographic and demographic factors. The condition predominantly affects males (in a ratio of approximately 1.5:1 to 2:1) and typically manifests during the peak adolescent growth spurt—between ages 12 and 16 in boys, and 10 and 14 in girls. The rising global prevalence of childhood obesity has radically shifted the epidemiological landscape of SCFE, dramatically increasing both the incidence and the severity of presentations. Bilateral involvement is observed in 20% to 40% of cases, with over half of these sequential slips occurring within 18 months of the initial presentation, necessitating rigorous contralateral surveillance.
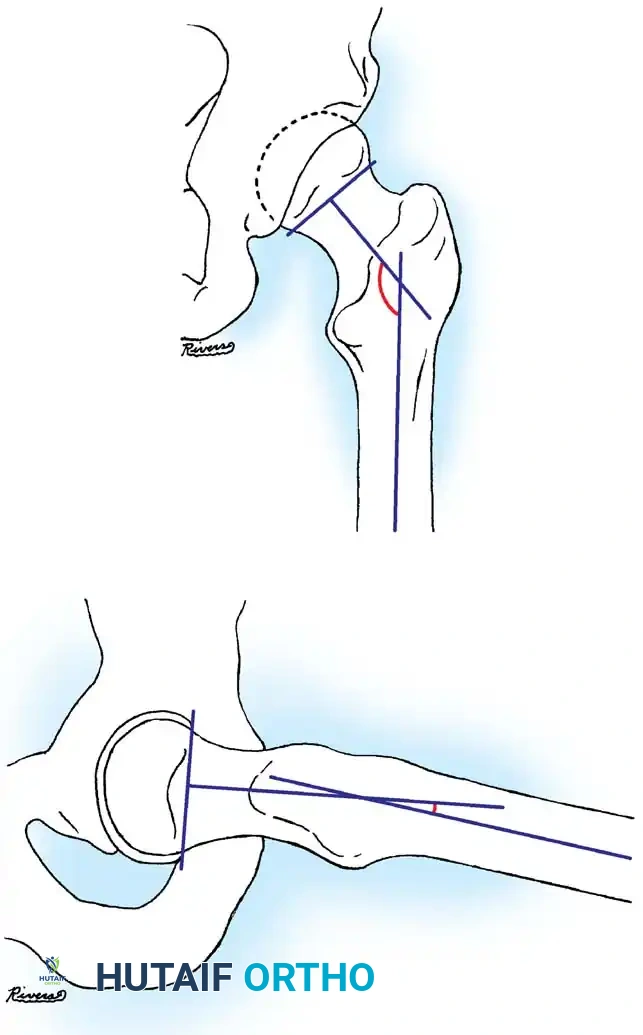
The pathogenesis of SCFE is fundamentally multifactorial, representing a critical failure of the physis under physiological or supra-physiological loads. During the adolescent growth spurt, the physis rapidly widens under the influence of growth hormone, specifically expanding the zone of hypertrophy. This rapid cellular proliferation inherently weakens the structural integrity of the cartilaginous matrix. When this transient mechanical vulnerability is coupled with the exponentially increased mechanical shear forces associated with obesity, the yield strength of the physis is catastrophically exceeded. Kordelle et al., utilizing three-dimensional computed tomography (CT) analysis in 30 slips, identified significant morphological variations predisposing to SCFE. They noted a reduced femoral anteversion averaging 7 degrees (compared to a normal 12.7 degrees) and a reduced femoral shaft angle of 134.2 degrees (compared to a normal 141 degrees).
Beyond mechanical factors, underlying endocrine or metabolic susceptibilities play a profound role, particularly in "atypical" SCFE. Conditions such as hypothyroidism, growth hormone deficiency, panhypopituitarism, and renal osteodystrophy fundamentally alter the maturation and mineralization of the physeal cartilage. In these endocrinopathies, the structural failure of the physis occurs at substantially lower mechanical thresholds. Children presenting with SCFE outside the typical age demographic (younger than 10 or older than 16), or those whose weight falls below the 50th percentile, must undergo an exhaustive endocrinological workup, as the slip is often the first orthopaedic manifestation of a severe systemic disease.
Detailed Surgical Anatomy and Biomechanics
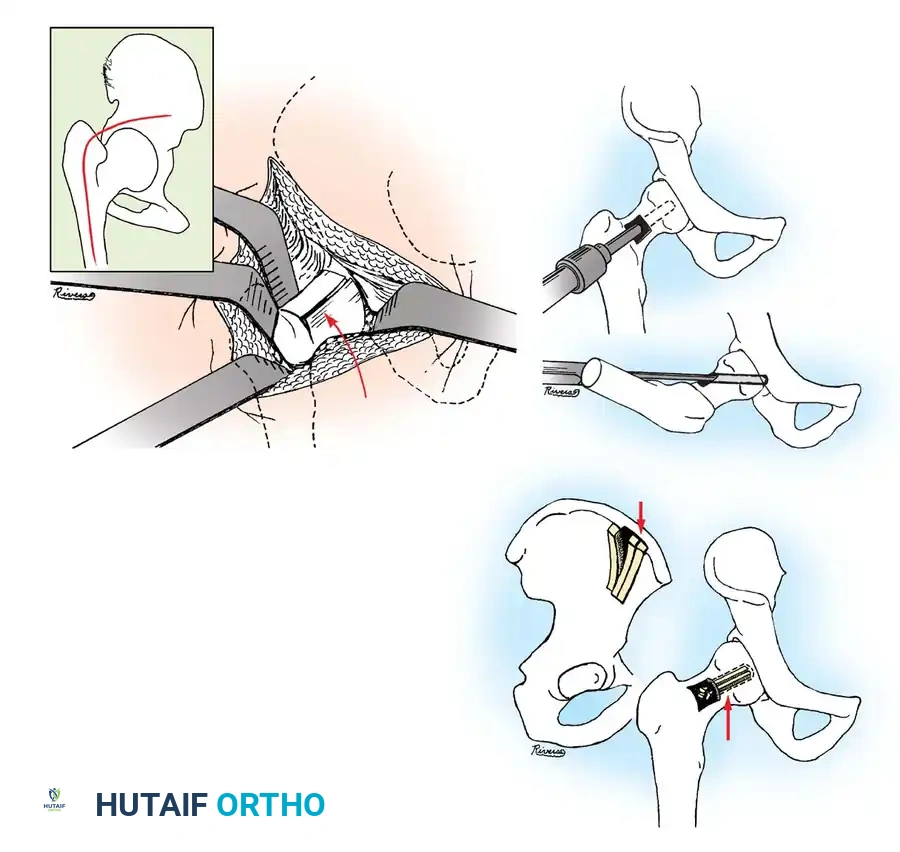
A profound mastery of the surgical anatomy of the proximal femur, particularly its tenuous vascular supply, is the absolute prerequisite for the operative management of SCFE. The proximal femoral epiphysis is supplied almost exclusively by the terminal branches of the medial femoral circumflex artery (MFCA). The deep branch of the MFCA courses posterior to the obturator externus tendon, ascending along the posterosuperior aspect of the femoral neck as the lateral epiphyseal retinacular vessels. These delicate vessels perforate the capsule at the intertrochanteric line and travel within the synovial retinacular folds to enter the epiphysis.

In the setting of SCFE, the posterior and inferior displacement of the epiphysis relative to the metaphysis places these retinacular vessels under extreme tension. As the femoral neck translates anteriorly and superiorly, the posterosuperior retinacular vessels are stretched across the sharp metaphyseal ridge. Any iatrogenic manipulation, particularly forceful internal rotation or aggressive reduction maneuvers, can stretch these vessels beyond their elastic limit, resulting in intimal tearing, thrombosis, and subsequent devastating avascular necrosis (AVN). Furthermore, in acute or unstable slips, the accumulation of an intracapsular hematoma can lead to a tamponade effect, further compromising epiphyseal perfusion and providing the theoretical basis for emergent capsulotomy.
Biomechanically, the proximal femoral physis is subjected to a complex interplay of compressive and shear forces. In a normal hip, the perichondrial ring of LaCroix and the interdigitating mammillary processes of the physis provide substantial resistance to shear stress. However, during adolescence, the perichondrial ring thins and weakens, and the physis shifts from a relatively horizontal orientation to a more oblique, vertical alignment. This anatomical reorientation exponentially increases the shear forces acting across the physeal plate during normal weight-bearing. When the applied shear stress exceeds the mechanical yield stress of the weakened hypertrophic zone, the epiphysis begins to displace.
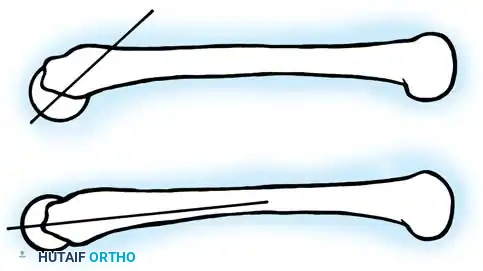
Radiographically, this biomechanical failure manifests in specific, highly characteristic patterns. On the anteroposterior (AP) radiograph, the normal intersection of Klein's line (a line drawn along the superior border of the femoral neck) with the lateral portion of the epiphysis is lost; this is known as Trethowan's sign. Additionally, the anterior translation of the metaphysis creates a double-density shadow over the femoral head on the AP view, known as the metaphyseal blanch sign of Steel. Recognizing these subtle morphological and biomechanical alterations is critical for diagnosing early or "preslip" conditions before catastrophic displacement occurs.
Exhaustive Indications and Contraindications
The therapeutic decision-making matrix for SCFE is dictated by the precise classification of the slip's stability, severity, and chronicity. The overarching goals of any surgical intervention are to halt the progression of the slip, stimulate rapid physeal symphysiodesis (closure), and meticulously avoid the triad of iatrogenic complications: osteonecrosis, chondrolysis, and severe femoroacetabular impingement (FAI). Nonoperative management, historically involving spica casting or prolonged traction, has been entirely abandoned in modern orthopaedic practice due to unacceptably high rates of chondrolysis and failure to reliably prevent slip progression.

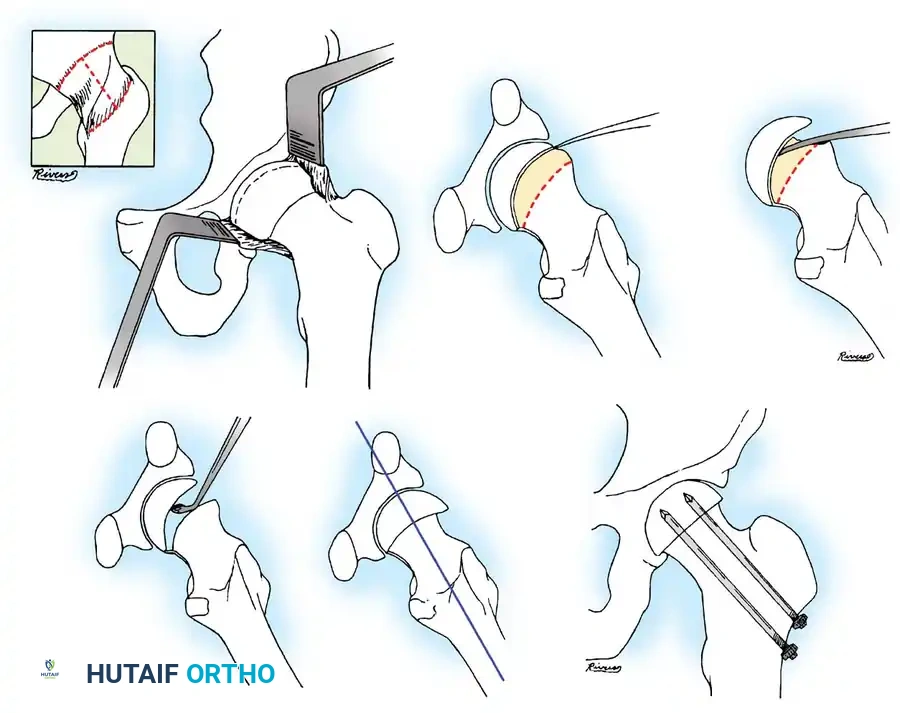
The Loder classification, which strictly dichotomizes slips into "stable" (patient can bear weight with or without crutches) and "unstable" (patient cannot bear weight), is the primary driver of surgical indications. Stable slips, regardless of their radiographic severity, are universally indicated for prompt percutaneous in situ pinning. Unstable slips represent a true orthopaedic emergency due to the impending threat of AVN. The surgical management of unstable slips is highly controversial, with options ranging from emergent in situ pinning with or without capsulotomy, to the technically demanding modified Dunn procedure (surgical hip dislocation with anatomical reduction).

Prophylactic pinning of the asymptomatic contralateral hip remains one of the most vigorously debated topics in pediatric orthopaedics. The indication for prophylactic fixation is heavily weighted by the patient's individual risk factors. Patients with atypical SCFE (endocrinopathies, renal failure, radiation therapy) have an exceedingly high risk of bilateral involvement and are absolute candidates for prophylactic pinning. For idiopathic cases, the modified Oxford Bone Age score is frequently utilized; patients with a low score (indicating significant remaining growth) and a high body mass index are strongly considered for prophylactic intervention to prevent future morbidity.
| Clinical Scenario | Primary Indication | Relative/Absolute Contraindication | Preferred Surgical Modality |
|---|---|---|---|
| Stable SCFE (Mild/Moderate) | Halting slip progression, promoting closure | Active joint infection (Absolute) | Percutaneous single-screw in situ pinning |
| Stable SCFE (Severe) | Halting progression | Open reduction (Relative - high AVN risk) | In situ pinning; delayed osteochondroplasty for FAI |
| Unstable SCFE | Urgent stabilization, preventing AVN | Delayed treatment > 24 hours (Relative) | Emergent in situ pinning ± capsulotomy OR Modified Dunn |
| Atypical SCFE (Young age) | Halting progression while allowing growth | Rigid fixation crossing physis (Relative) | Single dynamic screw fixation (smooth distally) |
| Asymptomatic Contralateral Hip | High risk of future slip (Endocrine, Obesity) | Near skeletal maturity (Absolute) | Prophylactic single-screw in situ pinning |
Contraindications to standard in situ pinning are relatively few but clinically significant. Active, untreated septic arthritis of the hip is an absolute contraindication to hardware placement. Severe, unoptimized medical comorbidities (e.g., profound uremia in untreated renal osteodystrophy) may serve as a relative contraindication requiring medical stabilization prior to anesthesia. Furthermore, in patients who have already achieved complete radiographic physeal closure (a rare presentation of a missed, chronic slip), in situ pinning offers no mechanical benefit, and the patient should instead be evaluated for corrective proximal femoral osteotomy to address the resultant FAI and biomechanical derangement.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful, complication-free SCFE surgery. The radiographic evaluation must strictly include a high-quality AP radiograph of the pelvis and a cross-table (true) lateral radiograph of the affected hip. The frog-leg lateral view, while excellent for detecting subtle preslips, is absolutely contraindicated in any patient with a suspected unstable slip, as the obligate abduction and external rotation maneuver can iatrogenically convert a mild slip into a catastrophic, completely displaced slip, rupturing the remaining retinacular vessels.

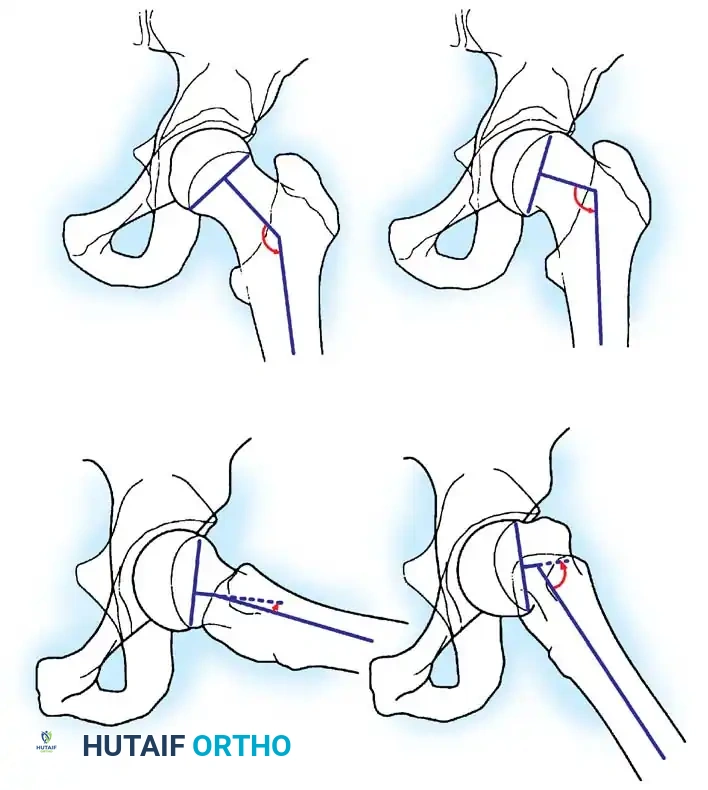
Preoperative templating is mandatory to determine the appropriate screw diameter, length, and trajectory. The Southwick slip angle must be calculated on both the AP and lateral radiographs to quantify the severity of the deformity. The surgeon must template for a cannulated screw (typically 6.5 mm or 7.3 mm) with a thread length designed to engage the epiphysis entirely without crossing the physis. If the threads bridge the physis, the compression effect is lost, and the risk of hardware failure increases. In cases of severe slips, templating will reveal that the starting point on the lateral femoral cortex must be moved significantly anteriorly to achieve a perpendicular trajectory into the displaced epiphysis.

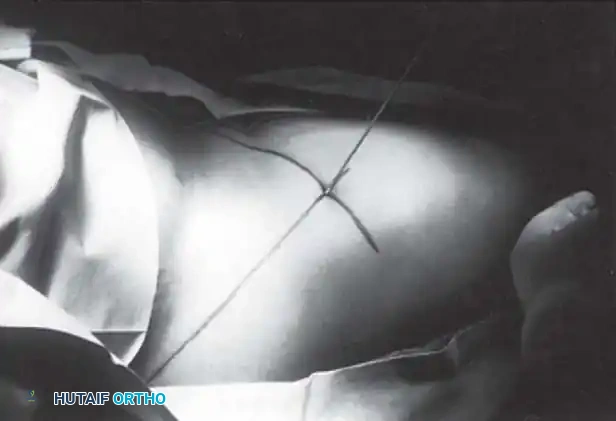
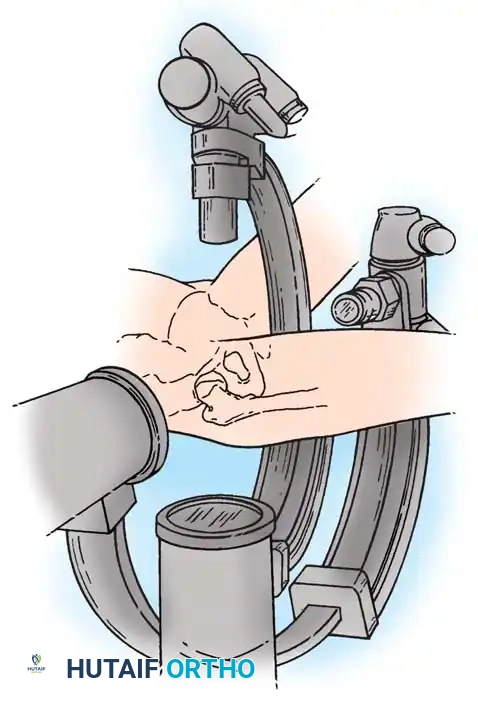
Patient positioning in the operating room is a critical, high-stakes phase of the procedure. The patient is placed supine on a radiolucent flat Jackson table or a specialized fracture table. For stable slips, the affected limb must be carefully supported and secured in its resting position of obligate external rotation. Under no circumstances should the surgeon attempt to internally rotate the limb to improve the radiographic appearance. Forceful internal rotation is the most common cause of iatrogenic AVN, as it directly wrings out the posterosuperior retinacular vessels against the metaphyseal step-off.

The fluoroscopic setup is equally paramount. The "rotating beam" technique is the absolute standard of care. The C-arm must be positioned such that it can arc freely 90 degrees from a perfect AP to a perfect true lateral projection without requiring any movement of the patient's operative limb. The well leg is typically placed in a lithotomy position or scissored posteriorly to allow unobstructed access for the C-arm base. The surgeon must verify that perfect, orthogonal images of the femoral head and neck can be obtained prior to prepping and draping. Failure to establish this imaging capability preoperatively invariably leads to misdirected hardware, joint penetration, and subsequent chondrolysis.

Step-by-Step Surgical Approach and Fixation Technique
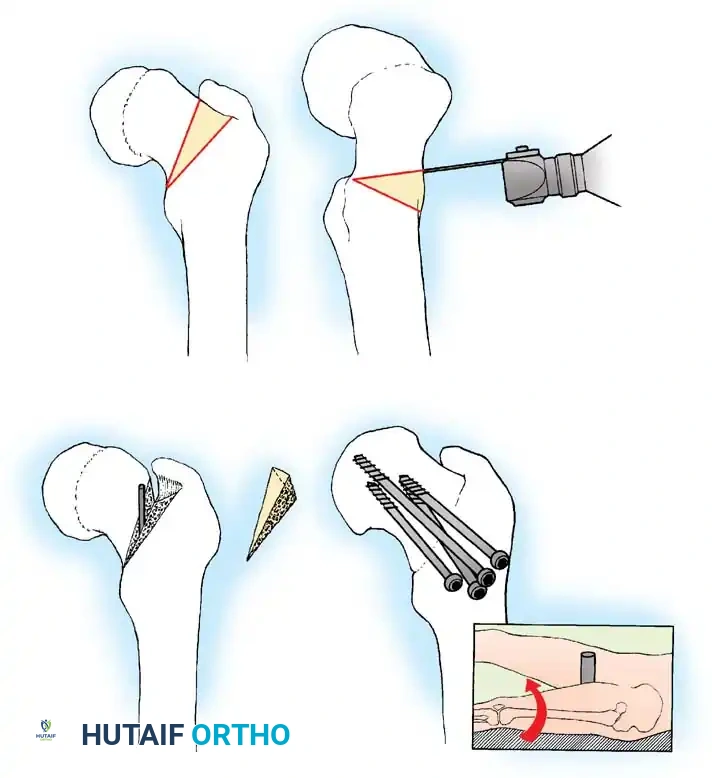
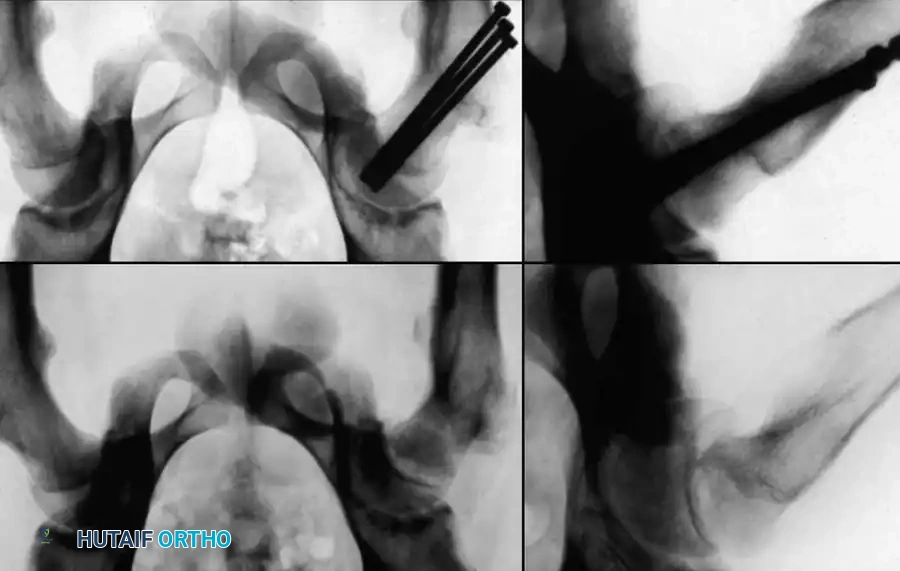
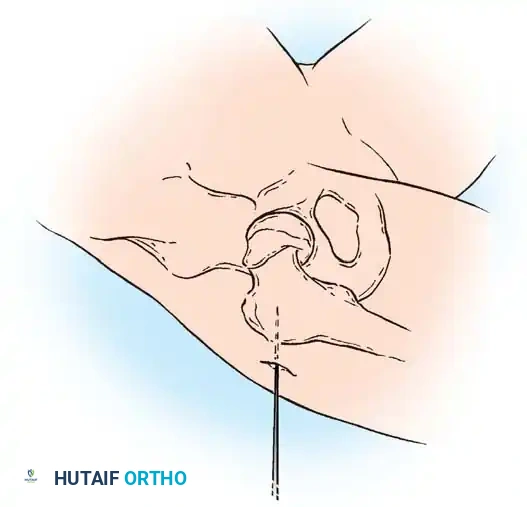
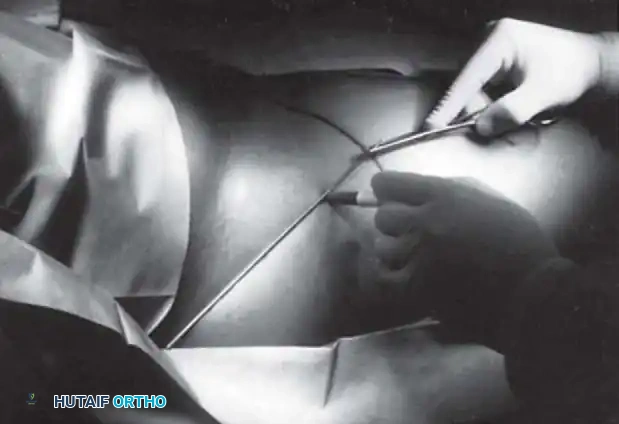
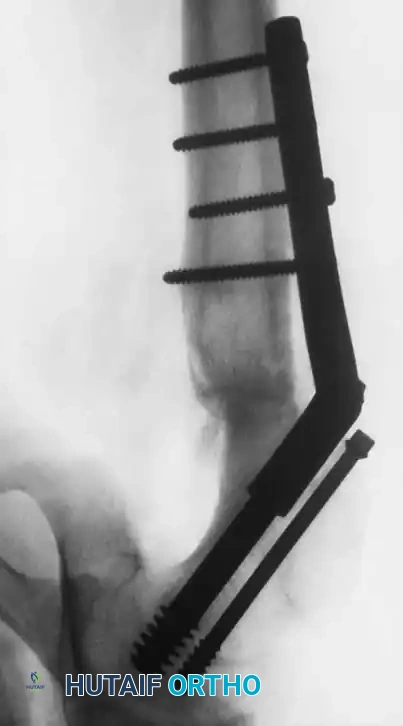
The percutaneous in situ pinning technique utilizing a single, large-diameter cannulated screw is the gold standard for the vast majority of SCFE presentations. The procedure begins with the identification of the optimal starting point on the proximal femur. Based on the Morrissy principles, the starting point is dictated entirely by the degree of posterior epiphyseal displacement. For mild slips, a standard lateral starting point near the level of the lesser trochanter is appropriate. However, as the severity of the slip increases, the starting point must migrate anteriorly on the intertrochanteric line.

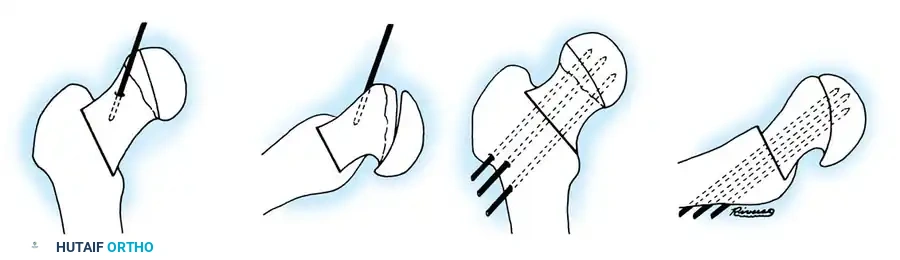
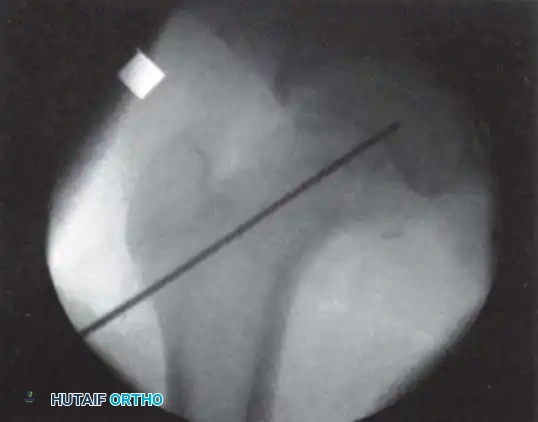
A small longitudinal stab incision is made over the templated starting point. Dissection is carried down through the fascia lata and the vastus lateralis muscle to the periosteum. A sturdy guidewire is then introduced onto the anterior-lateral cortex. The trajectory of the guidewire is the most critical step of the operation. The wire must be directed such that it crosses the physis perpendicular to the physeal plate and anchors perfectly in the geometric center of the displaced epiphysis. The surgeon must continuously alternate between the AP and true lateral fluoroscopic views as the wire is advanced.
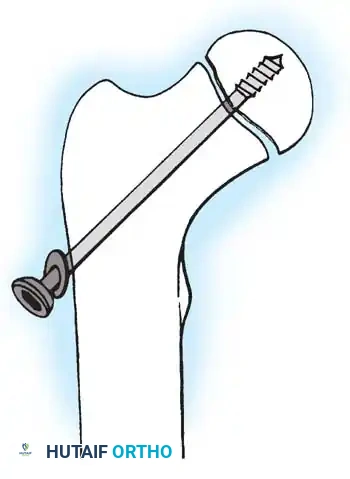
A common, devastating error is the "in-out-in" trajectory, where the guidewire exits the posterior femoral neck and re-enters the displaced posterior epiphysis. This trajectory inherently damages the posterior retinacular vessels and drastically increases the risk of AVN. To avoid this, the surgeon must ensure the wire remains entirely intraosseous on both the AP and lateral projections. Once the guidewire is positioned in the center of the epiphysis, its depth is measured. The goal is to place the tip of the screw 3 to 5 millimeters short of the subchondral bone to account for the convex geometry of the femoral head and prevent unrecognized joint penetration.
After measuring, the near cortex is overdrilled, and the selected cannulated screw (typically a 6.5 mm or 7.3 mm partially threaded screw with reverse-cutting flutes) is advanced over the wire. The threads must fully engage the epiphysis to provide adequate purchase, but they must not bridge the physis. Once the screw is seated, the surgeon must perform the "approach-withdrawal" fluoroscopic maneuver. The C-arm is live-fluoroscoped while the hip is gently rotated through a full 60-degree arc of motion. If the screw tip appears to approach the joint line and then withdraw, it is safely contained within the bone. If the tip remains at a constant distance from the joint line throughout the arc, it has penetrated the articular cartilage, and the screw must be immediately backed out to prevent catastrophic chondrolysis.
For atypical SCFE in very young patients, dynamic screw fixation is utilized to allow continued longitudinal growth of the femoral neck. A specialized screw with a short 10-mm thread profile is advanced until it engages only the epiphysis. The proximal portion of the screw is left protruding 15 to 20 millimeters laterally from the femoral cortex. As the child grows, the femoral neck elongates, and the epiphysis "rides" the smooth shaft of the screw laterally, preventing premature physeal closure and subsequent leg-length discrepancy or coxa breva.

Complications, Incidence Rates, and Salvage Management
The surgical management of SCFE is fraught with severe, life-altering complications. Osteonecrosis (AVN) is the most feared complication, characterized by the ischemic death of the proximal femoral epiphysis. The incidence of AVN is directly correlated with the stability of the slip at presentation. In stable slips, the AVN rate is historically less than 2%. However, in unstable slips, the rate skyrockets to between 20% and 47%, regardless of the treatment modality chosen. AVN typically manifests radiographically within 6 to 12 months post-operatively as subchondral sclerosis, cystic changes, and eventual structural collapse of the femoral head, leading to rapid, end-stage osteoarthritis.
Chondrolysis, or acute cartilage necrosis, is another devastating complication characterized by the rapid, progressive loss of articular cartilage space (defined as a joint space less than 3 mm). The etiology of chondrolysis is classically linked to unrecognized intra-articular hardware penetration, where the protruding screw mechanically abrades the acetabular cartilage. However, an autoimmune etiology has also been proposed, as chondrolysis can occur in unpinned hips or those treated strictly with spica casting. Patients present with profound stiffness, severe pain, and a global loss of range of motion. Management of established chondrolysis is exceptionally difficult, often requiring aggressive physical therapy, NSAIDs, and ultimately, salvage procedures such as arthrodesis or total hip arthroplasty in adulthood.

Femoroacetabular Impingement (FAI) is an almost universal, albeit initially insidious, complication of in situ pinning for moderate to severe slips. Because the epiphysis is pinned in its displaced, retroverted position, the prominent anterior metaphysis creates a massive "cam" lesion. During hip flexion and internal rotation, this metaphyseal prominence violently impacts the anterior acetabular rim, causing labral tearing and del
Clinical & Radiographic Imaging Archive