Complex Primary Total Knee Arthroplasty: Navigating Previous Surgeries and Medical Comorbidities

Key Takeaway
Total knee arthroplasty in the setting of previous surgical interventions, such as high tibial osteotomy or patellectomy, presents unique biomechanical and technical challenges. Surgeons must navigate altered anatomy, compromised soft-tissue envelopes, and disrupted kinematics. This comprehensive guide details evidence-based surgical strategies, including specialized approaches, component selection, and deformity correction, to optimize outcomes in complex primary arthroplasty and manage high-risk medical comorbidities effectively.
SURGICAL PROBLEMS RELATIVE TO SPECIFIC DISORDERS
The transition from a standard primary total knee arthroplasty (TKA) to a complex primary TKA is frequently dictated by the presence of prior surgical interventions or severe systemic medical comorbidities. Procedures such as high tibial osteotomy (HTO) and patellectomy fundamentally alter the biomechanical axis, soft-tissue envelope, and kinematic function of the knee joint. Consequently, the orthopedic surgeon must approach these cases with advanced preoperative templating, a mastery of extensile surgical exposures, and a comprehensive understanding of revision-style component utilization.
Total Knee Arthroplasty After Previous High Tibial Osteotomy
High tibial osteotomy (HTO) has historically been utilized to treat unicompartmental osteoarthritis of the knee, primarily serving as a time-buying procedure to delay eventual TKA in younger, active patients. Although early orthopedic doctrine suggested that a prior HTO had negligible effects on the outcome of a subsequent TKA, contemporary, high-powered studies have unequivocally demonstrated less successful clinical outcomes and highly predictable surgical challenges.
Clinical Outcomes and Literature Review
The literature presents a nuanced view of TKA following HTO, heavily dependent on the degree of preoperative deformity and the specific surgical techniques employed.
Windsor et al., Katz et al., and Mont et al. reported significantly lower total Knee Society Scores for patients with a history of HTO prior to TKA when compared to matched cohorts without prior osteotomy. Katz et al. specifically noted decreased postoperative ranges of motion in the HTO group. Furthermore, Windsor et al. correlated poor clinical outcomes with the presence of patella infera (patella baja)—a frequent sequela of the original osteotomy surgery and subsequent immobilization in a long leg cast.
Wound healing is a paramount concern. Jackson, Sarangi, and Newman reported significant wound healing complications in 30% (6 of 20) of patients with previous HTO, culminating in deep periprosthetic joint infections in four patients. These catastrophic failures were directly attributed to the difficulty in surgical exposure and the poor vascularity of the lateral skin flap.
In a robust review of 166 TKAs following HTO, Parvizi, Hanssen, and Spangehl identified an 8% revision rate at 6 years’ follow-up. They isolated several critical risk factors for failure, including:
* Male gender
* Obesity
* Younger age at the time of arthroplasty
* Preexisting varus-valgus ligamentous laxity
* Residual limb malalignment
Conversely, Staeheli, Cass, and Morrey, alongside Meding et al., reported functional outcomes and complication rates comparable to primary TKA. The more favorable results in these specific cohorts are largely attributed to lesser degrees of pre-TKA deformity; the average preoperative alignment was 3.5 degrees of valgus in Staeheli’s study and 4 degrees of valgus in Meding’s study.
Preoperative Planning and Incision Strategy
Several technical problems unique to patients with previous HTO must be anticipated to optimize conversion to TKA.
Surgical Warning: Skin incision planning is critical. While previous transverse skin incisions may generally be ignored, prior lateral longitudinal skin incisions must be strictly respected. To prevent catastrophic skin flap necrosis, an adequate intervening skin bridge of at least 8 cm must be maintained between the new midline incision and the old lateral incision.
Surgical Approach and Exposure
Extensive scarring over the lateral compartment and the infrapatellar region is routinely encountered, rendering standard patellar eversion and lateral compartment exposure exceedingly difficult.
Surgeons must be prepared to utilize extensile exposure techniques. If the patella cannot be safely everted without risking avulsion of the patellar tendon from the tibial tubercle, the following step-wise interventions should be considered:
1. Lateral Retinacular Release: Often the first step to improve patellar mobility.
2. V-Y Quadricepsplasty: Indicated for severe contractures, though it requires modified postoperative rehabilitation.
3. Tibial Tubercle Osteotomy (TTO): Provides excellent exposure and allows for proximal advancement of the extensor mechanism to correct preexisting patella infera.
Medial subperiosteal exposure must be executed with meticulous care to maintain the continuous soft-tissue sleeve, which is absolute necessary for secure closure and medial soft-tissue stability.
Bone Resection and Component Alignment
Following a failed valgus closing-wedge osteotomy of the proximal tibia, the surgeon will typically find that only minimal bone resection from the lateral tibial plateau is necessary.
The tibial cut must be referenced off the intact medial compartment. Because of the previous valgus correction, referencing the medial side frequently leaves a substantial uncontained defect on the lateral side of the tibia. This defect mandates the use of structural bone grafting or, more commonly, the placement of a metal augmentation wedge or block.
Clinical Pearl: A hallmark challenge after a closing-wedge HTO is the medial offset of the intramedullary canal of the tibia relative to the center of the tibial plateau. Intramedullary tibial alignment guides are often inaccurate in this setting. Extramedullary alignment is strongly advocated. Furthermore, medialization of the tibial tray or the use of an offset tibial stem may be required to accommodate the metaphyseal-diaphyseal mismatch.
Rotational deformity is another frequent complication, as the proximal tibial fragment may have been rotated relative to the tibial shaft during the index HTO. The tibial tray must be inserted with precise attention to rotational landmarks (e.g., the medial third of the tibial tubercle) to avoid internal rotation of the component, which invariably leads to severe patellar tracking complications.
Because ligamentous balancing is notoriously difficult due to asymmetric soft-tissue contractures and altered joint lines, routine Posterior Cruciate Ligament (PCL) substitution (using a Posterior Stabilized [PS] implant) is highly recommended by most arthroplasty authorities.
🔪 Surgical Technique: Joint Preparation and Balancing
Whether performing a unicompartmental arthroplasty or a complex primary TKA, meticulous joint preparation is required.
- Osteophyte Resection: Thoroughly remove all peripheral osteophytes from the femoral condyles and tibial plateau. Retained osteophytes cause impingement, restrict range of motion, and generate pain with weight-bearing. Appropriate medial peripheral osteophyte resection often allows for the passive correction of a varus deformity without necessitating thicker tibial polyethylene components.
- Component Sizing: Proper sizing of the femoral component is paramount. The implant must reproduce the anteroposterior dimension of the normal femoral condyle. In borderline cases, default to the larger component; this provides superior capping of the subchondral bone, thereby resisting loosening and subsidence.
- Posterior Condylar Resection: Resect the posterior condyle to at least the exact thickness of the femoral implant. To avoid tightness in flexion—a common cause of limited postoperative ROM—it is biomechanically safer to resect slightly too much of the posterior condyle rather than too little.
- Anterior Referencing: The junction of the eburnated bone on the femoral condyle and the remaining intact articular cartilage usually defines the anterior weight-bearing margin. Ensure the femoral component does not protrude anteriorly (overstuffing the patellofemoral joint), which disrupts patellar tracking. However, it must extend far enough anteriorly to cover the weight-bearing surface in contact with the tibia during full extension.
- Tibial Restoration: Select a tibial component thick enough to restore the tibial plateau to its original anatomic height.
- Ligamentous Tensioning: After component trialing, the joint space kinematics must be assessed. When valgus stress is applied with the knee fully extended, the medial joint space should open exactly 1 to 2 mm. Similarly, the lateral joint space should open 1 to 2 mm under varus stress. Components placed too tightly will cause the tibia to subluxate toward the opposite compartment, producing excessive contact pressures and accelerated polyethylene wear.
- Tracking Assessment: If the quadriceps mechanism is everted during the procedure, congruency of the components and patellar tracking must be checked with the knee extended, not flexed, to accurately assess the extensor mechanism vector.
Total Knee Arthroplasty After Previous Patellectomy
Historically, patellectomy was utilized for severe patellofemoral arthritis or comminuted patellar fractures. Performing a TKA in a patellectomized knee presents profound biomechanical disadvantages. Early clinical studies reported highly variable results, with the majority of patients experiencing persistent anterior knee pain and severe functional disability secondary to profound quadriceps weakness.
Biomechanical Implications: The Four-Bar Linkage
To understand the failure mechanisms in these knees, one must understand the kinematics of the normal knee. Sledge and Ewald elegantly described the knee as a "four-bar linkage system" comprising the quadriceps tendon, the patellar tendon, the anterior cruciate ligament (ACL), and the posterior cruciate ligament (PCL).
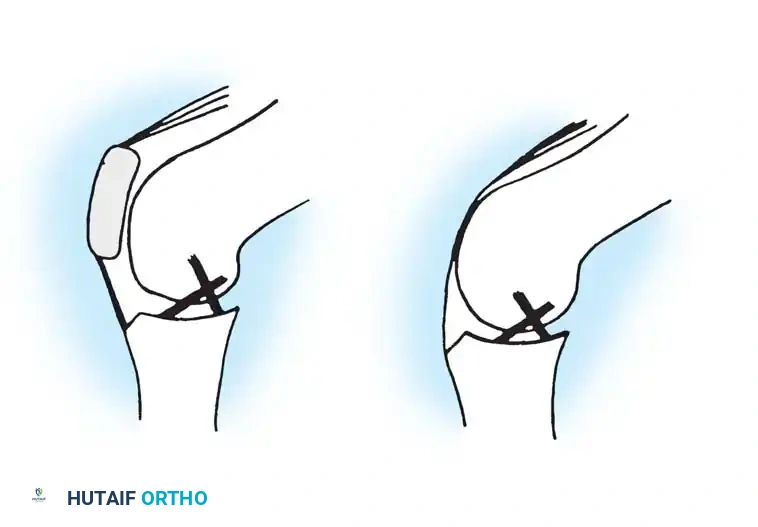
The patella acts as a critical fulcrum, increasing the moment arm of the extensor mechanism. Loss of the patella results in a considerable alteration of the mechanical axis and destroys this four-bar linkage. Without the anterior counter-force provided by the intact extensor mechanism, the PCL and posterior capsule are subjected to immense stress and are ultimately incapable of maintaining long-term sagittal plane stability.
Implant Selection and Clinical Outcomes
Recent advancements in implant design have yielded more encouraging results, though the optimal prosthesis remains a subject of academic debate.
Laskin and Palleta conducted a pivotal comparative study evaluating TKA after patellectomy, contrasting PCL-retaining (Cruciate Retaining, CR) and PCL-substituting (Posterior Stabilized, PS) prostheses against a control group.
* PCL-Substituting (PS) Designs: Yielded significantly greater Knee Society Scores. The cam-and-post mechanism compensates for the lost sagittal stability.
* PCL-Retaining (CR) Designs: Demonstrated unacceptable levels of anteroposterior instability over time due to the failure of the isolated PCL to resist posterior tibial translation without a competent extensor mechanism.

Surgical Warning: Patients with a history of multiple previous knee surgeries, including patellectomy, experience significantly less reliable pain relief following TKA. Lennox, Hungerford, and Krackow demonstrated that patients who had undergone more than three prior knee operations, possessed only moderate tibiofemoral arthritic changes, and exhibited compromised quadriceps function, universally tended toward poor outcomes.
Surgeons must manage patient expectations aggressively in this cohort. Meticulous attention must be paid to coronal limb alignment, precise ligamentous balancing, and the liberal use of bone grafting or prosthetic augmentation for bony defects. Revision-type components (e.g., stems, constrained inserts) should be readily available and utilized when necessary.
Arthroplasty in the Setting of Other Medical Conditions
Systemic medical comorbidities drastically alter the risk profile and surgical approach to TKA.
Hemophilic Arthropathy
Recurrent hemarthroses in patients with hemophilia lead to severe, early-onset, destructive arthropathy. While TKA provides excellent pain relief in this population, the restoration of motion is frequently suboptimal, and the perioperative complication profile is formidable.

Figgie, Goldberg, and Figgie reported significant postoperative complications in over 50% (10 of 19) of TKAs performed in hemophilic patients. Complications included massive hemorrhage, superficial skin necrosis, nerve palsies, and deep periprosthetic infections. Furthermore, progressive radiolucencies were observed adjacent to 13 of the tibial components, indicating early aseptic loosening.
Hematologic Management: The complication rate is directly tied to perioperative hemostasis. A perioperative Factor VIII level of less than 80% correlates with a drastically higher probability of complications. It is strictly recommended that perioperative Factor VIII levels be maintained at 100% through coordinated care with a hematologist.
Infectious and Vascular Risks: Historically, many patients with hemophilic arthropathy contracted the Human Immunodeficiency Virus (HIV) from contaminated transfusions of coagulation factors. In this specific sub-population, the most common complication after TKA is deep infection, with reported rates soaring to 30%.
Additionally, Saris et al. identified a high prevalence of periarticular aneurysms (7 out of 10 patients) via preoperative arteriography. Routine preoperative angiography, with prophylactic embolization of aneurysms as required, is strongly recommended before proceeding with TKA in hemophilic patients.
Diabetes Mellitus
Diabetes mellitus exerts a profound negative effect on arthroplasty outcomes. England et al., Serna et al., and Meding et al. have all independently reported that TKA in diabetic patients results in:
* Increased wound complication rates
* Higher incidences of deep periprosthetic joint infection
* More frequent aseptic and septic revisions
Serna et al. noted that both insulin-dependent and non-insulin-dependent diabetics suffer similar complication rates and diminished functional scores compared to non-diabetic controls. Furthermore, Forrest et al. identified diabetes mellitus and advanced age as independent risk factors requiring admission to an inpatient rehabilitation facility postoperatively. This is hypothesized to be secondary to the proximal muscle weakness and peripheral neuropathy inherent to chronic diabetes, which severely impedes standard postoperative physical therapy.
Psoriatic Arthritis
An inflammatory arthropathy clinically mimicking rheumatoid arthritis develops in approximately 7% of patients with psoriasis. The primary surgical concern in these patients is the presence of exfoliating psoriatic plaques on the extensor surfaces of the knee, which are heavily colonized with bacterial pathogens (predominantly Staphylococcus species).
Stern et al. reported an alarming deep infection rate of 17% (4 of 24 knees) following TKA in psoriatic patients. Conversely, Beyer et al., who strictly excluded patients with a positive rheumatoid factor, reported only a 2% deep infection rate.
Clinical Pearl: The absolute prerequisite for elective TKA in a patient with psoriasis is the optimal dermatologic control of psoriatic lesions in the vicinity of the proposed surgical incision. Surgery should be delayed until periarticular plaques are fully cleared to mitigate the risk of catastrophic periprosthetic joint infection.
Neuropathic (Charcot) Arthropathy
Historically, neuropathic arthropathy was considered an absolute contraindication to TKA due to the lack of protective proprioception and the high risk of catastrophic implant failure. However, contemporary literature suggests that fair-to-good results can be achieved with meticulous technique.
Parvizi, Marrs, and Morrey reviewed 40 TKAs in patients with Charcot arthropathy. They noted that excessive bone fragmentation frequently necessitated the use of structural bone grafting or metallic augmentation. Despite a 15% reoperation rate, limb salvage and functional ambulation were largely achieved. Success in neuropathic joints demands the use of highly constrained prostheses (often rotating hinge designs), robust intramedullary stem fixation to bypass metaphyseal bone loss, and prolonged postoperative bracing to protect the reconstruction while soft tissues heal.
You Might Also Like

