Primary Total Knee Arthroplasty: Functional Outcomes, Radiographic Evaluation, and Long-Term Survivorship
Key Takeaway
Evaluating the success of primary total knee arthroplasty requires standardized functional and radiographic metrics. The Knee Society Score separates joint-specific function from overall patient mobility, preventing age-related decline from skewing implant success rates. Radiographic evaluation utilizes a standardized zone system to monitor radiolucencies and component alignment. Long-term survivorship of modern cemented prostheses exceeds 90% at two decades, though meticulous surgical technique and biomechanical restoration remain paramount to preventing aseptic loosening and polyethylene wear.
INTRODUCTION TO TOTAL KNEE ARTHROPLASTY OUTCOMES
Primary Total Knee Arthroplasty (TKA) is widely recognized as one of the most successful and cost-effective procedures in modern orthopedic surgery. Designed to relieve pain, restore function, and improve the quality of life in patients with end-stage degenerative joint disease, the procedure has undergone decades of refinement in implant design, biomechanical understanding, and surgical technique.
To accurately assess the efficacy of these advancements, the orthopedic community relies on standardized, reproducible outcome measures. Historically, outcome reporting was highly variable, making cross-study comparisons difficult. The paradigm shifted significantly in the late 1980s with the introduction of standardized clinical and radiographic scoring systems, which remain the foundation of modern orthopedic literature. This comprehensive guide details the functional and radiographic outcome measures used to evaluate TKA, the biomechanical and surgical principles required to optimize these outcomes, and the long-term survivorship of various prosthesis designs.
FUNCTIONAL OUTCOME MEASURES: THE KNEE SOCIETY SCORE
In 1989, the Knee Society published its revised clinical rating system, fundamentally changing how TKA outcomes were reported. Prior to this, the most commonly utilized metric was the Hospital for Special Surgery (HSS) knee rating system.
The primary catalyst for the Knee Society's revision was the critical need to separate a patient’s overall functional ability from the specific function of the knee joint. In an aging demographic, a patient's overall functional capacity often declines due to cardiopulmonary comorbidities, neurologic conditions, or contralateral joint arthritis, even if the replaced knee remains perfectly stable and painless. By separating these variables, the Knee Society Score (KSS) prevents the artificial deflation of TKA success rates caused by unrelated systemic decline.
The Dual-Scoring Architecture
The Knee Society clinical rating system is divided into two distinct 100-point scales: the Knee Score and the Patient Function Score.
1. The Knee Score (100 Points Maximum)
This score isolates the objective and subjective status of the operated joint.
* Pain (50 Points): The most heavily weighted parameter. A completely painless knee scores 50 points. Mild or occasional pain scores 45; pain only on stairs scores 40; pain with walking and stairs scores 30; moderate occasional pain scores 20; continual pain scores 10; and severe pain scores 0.
* Range of Motion (25 Points): Calculated as 1 point for every 5 degrees of flexion arc achieved.
* Stability (25 Points): Assessed as the maximal movement in any position.
* Anteroposterior Stability: < 5 mm (10 pts), 5–10 mm (5 pts), > 10 mm (0 pts).
* Mediolateral Stability: < 5 degrees (15 pts), 6–9 degrees (10 pts), 10–14 degrees (5 pts), > 15 degrees (0 pts).
Deductions for the Knee Score:
Points are aggressively deducted for surgical or rehabilitative failures:
* Flexion Contracture: 5–10° (-2 pts), 10–15° (-5 pts), 16–20° (-10 pts), > 20° (-15 pts).
* Extension Lag: < 10° (-5 pts), 10–20° (-10 pts), > 20° (-15 pts).
* Malalignment: Ideal alignment is considered 5–10 degrees of valgus (0 deductions). Alignment of 0–4 degrees or 11–15 degrees incurs a deduction of 3 points per degree of deviation. Other severe malalignments deduct 20 points.
2. The Patient Function Score (100 Points Maximum)
This score evaluates the patient's practical mobility.
* Walking Distance (50 Points): Unlimited (50 pts), > 10 blocks (40 pts), 5–10 blocks (30 pts), < 5 blocks (20 pts), housebound (10 pts), unable (0 pts).
* Stair Climbing (50 Points): Normal up and down (50 pts), normal up but down with rail (40 pts), up and down with rail (30 pts), up with rail but unable down (15 pts), unable (0 pts).
Deductions for the Function Score:
* Use of a cane (-5 pts).
* Use of two canes (-10 pts).
* Use of crutches or a walker (-20 pts).
Clinical Pearl: When evaluating a patient with a poor Function Score but an excellent Knee Score, always categorize the patient accurately. The Knee Society utilizes three categories: Category A (Unilateral or bilateral with opposite knee successfully replaced), Category B (Unilateral, other knee symptomatic), and Category C (Multiple arthritis or medical infirmity). This categorization provides vital context for the functional score.
RADIOGRAPHIC EVALUATION AND SCORING SYSTEM
Simultaneous to the clinical score revision in 1989, the Knee Society (spearheaded by Ewald) introduced the Total Knee Arthroplasty Radiographic Evaluation and Scoring System. The goal was to standardize the radiographic parameters measured when reporting TKA outcomes, eliminating subjective interpretations of implant fixation and alignment.
Standardized Radiographic Parameters
The system mandates the evaluation of specific criteria on standardized recumbent and standing anteroposterior (AP) and lateral radiographs, as well as skyline patellar views. The parameters include:
1. Component Alignment: Measurement of the femoral flexion angle, tibial angle, and total valgus angle.
2. Tibial Surface Coverage: The percentage of the resected tibial plateau covered by the baseplate.
3. Radiolucencies: The width (in millimeters) and extent of radiolucent lines at the bone-cement or bone-implant interface.
4. Patellar Problem List: Evaluation of the prosthesis angle, eccentric component placement, subluxation, and dislocation.
The Zone Scoring System for Radiolucencies
To quantify the risk of aseptic loosening, developers of total knee prostheses superimpose silhouettes of their designs onto the Knee Society form, assigning specific radiographic zones.
For the standard seven-zone tibial component, radiolucencies are measured in millimeters for each zone and summed to create a total score:
* Score $\le$ 4: Generally considered insignificant and often represents a non-progressive physiological radiolucent line (especially in cemented implants where a thin, sclerotic-margined line may appear in the first year).
* Score 5 to 9: Indicates a need for close, serial radiographic follow-up to monitor for progression.
* Score $\ge$ 10: Signifies possible or impending clinical failure, regardless of whether the patient is currently symptomatic.
Surgical Warning: Do not confuse a stable, non-progressive radiolucent line (often $< 2$ mm with a sclerotic border) with aggressive osteolysis. Progressive radiolucencies, especially those appearing after years of stability or those accompanied by scalloping, strongly suggest polyethylene wear debris-induced osteolysis or late infection.
SURGICAL PRINCIPLES TO OPTIMIZE OUTCOMES
Achieving excellent Knee Society Scores and pristine radiographic evaluations requires meticulous surgical technique. The biomechanics of the knee must be respected, and the components must be placed with high precision.
Patient Positioning and Surgical Approach
- Positioning: The patient is placed supine on the operating table. A tourniquet is typically applied to the proximal thigh. A lateral post or leg holder is utilized to allow the knee to be flexed past 90 degrees and to provide a fulcrum for valgus/varus stress during exposure and balancing.
- Surgical Approach: The medial parapatellar approach remains the gold standard, offering excellent exposure of all three compartments. The incision extends from the proximal pole of the patella to the tibial tubercle. Alternative approaches, such as the subvastus or midvastus, may be utilized to preserve the extensor mechanism and potentially accelerate early functional recovery, though they offer more limited exposure in complex or stiff knees.
Biomechanics and Component Alignment
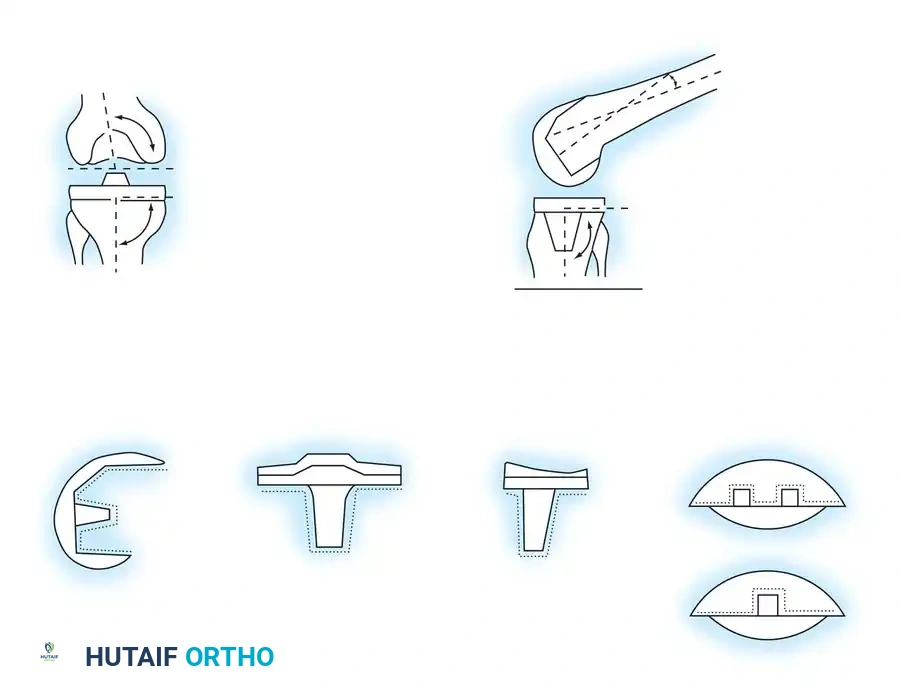
The primary biomechanical goal of TKA is the restoration of the mechanical axis (a line drawn from the center of the femoral head to the center of the ankle joint) to pass through the center of the knee.
* Coronal Alignment: The femoral component is typically placed in 5 to 7 degrees of valgus relative to the anatomical axis of the femur, while the tibial component is cut perpendicular (0 degrees) to the mechanical axis of the tibia. Failure to achieve this results in point-loading of the polyethylene, leading to accelerated wear and high radiographic radiolucency scores.
* Sagittal Alignment: The femoral component should avoid excessive flexion or extension to prevent notching of the anterior cortex or altering the flexion gap. The tibial component is typically placed with 0 to 7 degrees of posterior slope, depending on the implant design (Cruciate-Retaining vs. Posterior-Stabilized) and the patient's native anatomy.
* Gap Balancing vs. Measured Resection: Achieving equal flexion and extension gaps is critical for the "Stability" portion of the KSS. A tight extension gap leads to flexion contractures (KSS deductions), while a loose flexion gap leads to anteroposterior instability.
PROSTHESIS SURVIVORSHIP AND LONG-TERM RESULTS
Modern knee arthroplasty began in the early 1970s with the development of the total condylar knee prosthesis by Insall and colleagues at the Hospital for Special Surgery. Survivorship studies utilizing this pioneering prosthesis serve as the historical gold standard against which all modern knee replacements are compared.
Long-Term Survivorship Benchmarks
Long-term series by Ranawat et al., Font-Rodriguez et al., and Pavone et al. have meticulously documented the longevity of the original total condylar prosthesis. These landmark studies demonstrated a survivorship of 95% at 15 years and 91% at 21 and 23 years. These results established TKA as a highly durable intervention for the aging population.
Cruciate-Retaining (CR) vs. Posterior-Stabilized (PS) Designs
The debate between retaining or substituting the posterior cruciate ligament (PCL) has dominated TKA literature for decades. Both philosophies have yielded exceptional long-term results.
* PCL-Retaining Designs: Multiple studies have documented 10-year survivorships of 95% or greater. Gill and Joshi reported an impressive survivorship of 96% at 15 years and 82% at 23 years for a specific PCL-retaining design. Furthermore, using a modular tibial design, Dixon et al. reported a 93% survivorship at 15 years.
* PCL-Substituting (Posterior-Stabilized) Designs: These designs, which utilize a cam-and-post mechanism to substitute for the resected PCL, show equivalent longevity. Font-Rodriguez et al. reported a survivorship of 98% at 14 years with a PCL-substituting design.
Ultimately, registry data suggests that the choice between CR and PS designs should be based on surgeon preference, patient anatomy, and the integrity of the native PCL, as long-term survivorship is comparable.
The Role of Component Fixation: Cemented vs. Cementless
- Cemented Fixation: The use of polymethylmethacrylate (PMMA) bone cement remains the gold standard for TKA fixation worldwide. It provides immediate, rigid fixation, allowing for early weight-bearing, and is responsible for the >90% survivorship at two decades seen in the aforementioned studies.
- Cementless Fixation: Introduced to achieve biologic fixation via osseointegration, cementless fixation has historically yielded mixed results. While some modern highly porous designs have equaled the success of cemented implants, earlier generations suffered from higher rates of failure. These failures were primarily driven by tibial baseplate loosening, accelerated polyethylene wear (due to backside wear in modular components), and subsequent osteolysis. Today, cementless TKA is generally reserved for younger, highly active patients with excellent bone stock, utilizing modern highly porous titanium interfaces.
POSTOPERATIVE PROTOCOLS TO MAXIMIZE OUTCOMES
To ensure the surgical success translates into high Knee Society Scores, a rigorous, evidence-based postoperative protocol is mandatory.
- Immediate Mobilization: Patients are encouraged to bear full weight as tolerated on the day of surgery. Early mobilization reduces the risk of deep vein thrombosis (DVT) and improves the KSS Function Score.
- Range of Motion (ROM) Therapy: Aggressive early ROM exercises are critical. The goal is to achieve full extension (0 degrees) immediately to prevent the severe KSS deductions associated with flexion contractures. Flexion should reach 90 degrees before hospital discharge, progressing to 110–120 degrees in the outpatient setting.
- Pain Management: A multimodal analgesia approach—utilizing regional nerve blocks (e.g., adductor canal blocks), periarticular local anesthetic infiltration, NSAIDs, acetaminophen, and minimal opioids—is essential. Adequate pain control directly correlates with the patient's ability to participate in physical therapy, thereby maximizing the KSS Pain and ROM scores.
- Radiographic Surveillance: Baseline standing AP, lateral, and skyline radiographs should be obtained prior to discharge. Subsequent imaging at 1 year, 5 years, and 10 years should be evaluated using the Knee Society Radiographic Evaluation System to monitor for silent osteolysis or progressive radiolucencies in the 7 tibial zones.
CONCLUSION
The evaluation of primary total knee arthroplasty relies heavily on the rigorous application of the Knee Society Clinical Rating System and the Radiographic Evaluation System. By separating joint-specific function from overall patient mobility, and by standardizing the measurement of radiolucencies and alignment, orthopedic surgeons can accurately track the success of their interventions. With meticulous surgical technique, appropriate implant selection, and adherence to modern biomechanical principles, TKA continues to demonstrate outstanding long-term survivorship, exceeding 90% at two decades.
You Might Also Like