Mastering Preoperative Evaluation and Surgical Preparation in Total Knee Arthroplasty
Key Takeaway
A meticulous preoperative evaluation is the cornerstone of a successful Total Knee Arthroplasty (TKA). This phase demands rigorous radiographic templating to determine mechanical axes, comprehensive medical optimization to mitigate perioperative risks, and strategic anesthetic selection. By integrating detailed anatomical assessments with tailored regional or general anesthesia protocols, orthopedic surgeons can minimize complications, optimize biomechanical alignment, and ensure superior postoperative functional outcomes for patients undergoing joint reconstruction.
PREOPERATIVE EVALUATION AND INDICATIONS
The foundation of a successful Total Knee Arthroplasty (TKA) is established long before the patient enters the operating theater. The most critical component of the preoperative evaluation is confirming that surgical intervention is unequivocally indicated. TKA is primarily indicated for severe, end-stage osteoarthritis, rheumatoid arthritis, or post-traumatic arthritis that has proven refractory to comprehensive conservative management (e.g., NSAIDs, physical therapy, intra-articular corticosteroid or hyaluronic acid injections, and lifestyle modifications).
The primary goals of TKA are pain relief, restoration of functional mobility, and correction of deformity. However, the procedure is not without significant physiological demands. Because the demographic undergoing TKA is predominantly elderly, a meticulous, multidisciplinary approach to preoperative evaluation is mandatory to prevent life-threatening or limb-threatening complications.
Biomechanical Principles of TKA
Understanding the biomechanics of the native and prosthetic knee is essential for preoperative planning. The primary biomechanical objective of TKA is to restore the mechanical axis of the lower extremity to neutral (0 degrees Hip-Knee-Ankle angle), ensuring symmetrical load distribution across the polyethylene bearing surface.
Clinical Pearl: Failure to restore the mechanical axis within ±3 degrees of neutral significantly increases the risk of eccentric polyethylene wear, aseptic loosening, and premature catastrophic failure of the implant.
The native knee operates with complex kinematics, including "rollback" of the femur on the tibia during flexion, driven by the cruciate ligaments and the geometry of the articular surfaces. Preoperative planning must account for whether a cruciate-retaining (CR) or posterior-stabilized (PS) implant will be utilized, as this dictates the necessary bone resections and soft tissue balancing required to replicate native kinematics.
RADIOGRAPHIC EVALUATION AND TEMPLATING
A comprehensive radiographic series is non-negotiable. Standard preoperative knee radiographs must include:
* Standing Anteroposterior (AP) View: Assesses medial and lateral joint space narrowing, osteophyte formation, and coronal plane deformity.
* Lateral View: Evaluates patellofemoral joint space, posterior osteophytes, and the anatomical posterior tibial slope.
* Skyline (Merchant) View: Critical for assessing patellofemoral tracking, subluxation, and isolated patellofemoral arthritis.
The Long-Leg Standing Radiograph
A long-leg standing AP radiograph (hip-to-ankle) is highly beneficial, and often considered mandatory, for determining the mechanical axis of the limb. This is particularly critical when extra-articular deformity secondary to prior trauma, metabolic bone disease, or previous surgical procedures (e.g., high tibial osteotomy) is present.
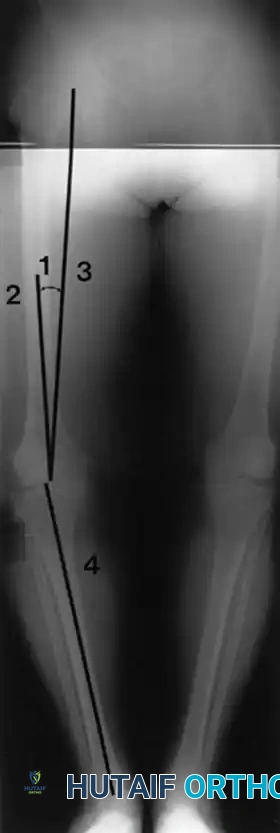
Fig. 6-26 Anatomical and mechanical axes of femur and tibia are determined independently on preoperative long-leg radiographs, with the goal of centering postoperative mechanical axis of limb within center of prosthetic knee. 1, Angle between anatomical (2) and mechanical (3) axes of femur. 4, Mechanical axis of tibia (see text).
The long-leg film allows the surgeon to calculate the angle between the anatomical axis of the femur (the intramedullary canal) and the mechanical axis of the femur (a line drawn from the center of the femoral head to the center of the knee). This angle, typically between 5 and 7 degrees, dictates the valgus cut angle set on the distal femoral cutting block. Furthermore, the long-leg film is vital for identifying significant diaphyseal bowing of the tibia or femur, which may preclude the use of standard intramedullary alignment guides and necessitate extramedullary referencing or computer-assisted navigation.
Digital Templating
Preoperative digital templating is utilized to:
* Anticipate approximate femoral and tibial component sizes.
* Identify significant bone defects (e.g., severe uncontained tibial plateau defects) that may require metal augments, bone grafting, or metaphyseal cones/sleeves.
* Determine the optimal level of the joint line to prevent patella baja or alta.
COMPREHENSIVE MEDICAL OPTIMIZATION
The preoperative medical evaluation of TKA candidates must be exhaustive. Patients with multiple unoptimized medical risk factors demonstrate exponentially higher rates of perioperative morbidity, prolonged hospital stays, and increased readmission rates.
Cardiopulmonary Assessment
Patients must possess adequate cardiopulmonary reserve to withstand the physiological stress of anesthesia and an anticipated perioperative blood loss of 1000 to 1500 mL.
* Routine Testing: A baseline electrocardiogram (ECG) is mandatory.
* Specialist Consultation: Patients with a history of coronary artery disease, congestive heart failure, chronic obstructive pulmonary disease (COPD), or restrictive airway disease require formal evaluation and clearance by cardiology or pulmonology consultants.
* Chest Radiography: Routine use of a chest radiograph is not cost-effective as a universal screening tool; however, it is strictly indicated in patients with a documented history of cardiopulmonary disease or active symptomatology.
Modifiable Risk Factors
- Smoking Cessation: Smokers exhibit significantly longer operative times, higher rates of wound necrosis, delayed healing, and increased periprosthetic joint infection (PJI) rates. Smoking cessation should be mandated at least 4 to 6 weeks prior to surgery.
- Glycemic Control: Diabetic patients must be optimized. An HbA1c > 7.5% or perioperative hyperglycemia (>200 mg/dL) drastically increases the risk of PJI.
- Nutritional Status: Malnutrition (Albumin < 3.5 g/dL, Transferrin < 200 mg/dL) must be corrected to ensure adequate wound healing.
Vascular and Hematologic Evaluation
Vascular supply to the operative extremity must be meticulously evaluated via palpation of dorsalis pedis and posterior tibial pulses.
Surgical Warning: If adequate vascularity is questionable (e.g., absent pulses, trophic skin changes), noninvasive arterial studies (Ankle-Brachial Index, Doppler ultrasound) must be obtained. A vascular surgery consultation is imperative, as performing a TKA—especially with a tourniquet—in a severely ischemic limb can precipitate acute limb ischemia and subsequent amputation.
Routine preoperative laboratory evaluation should include a complete blood count (CBC), comprehensive metabolic panel (electrolytes, BUN, creatinine), and urinalysis to rule out asymptomatic bacteriuria. Routine coagulation studies (PT/INR, aPTT) are unnecessary unless the patient has a known history of coagulopathy, hepatic dysfunction, or is actively taking anticoagulant medications. Patients on chronic anticoagulation require a carefully bridged perioperative management plan to limit intraoperative hemorrhage while preventing thromboembolic events.
ANESTHETIC MODALITIES: REGIONAL VS. GENERAL
The selection between regional (neuraxial) and general anesthesia for TKA is a complex decision influenced by patient comorbidities, anatomical constraints, and institutional protocols. The anesthesiologist bears the ultimate responsibility for this selection, though it requires close collaboration with the orthopedic surgeon.
Cardiovascular and Cognitive Outcomes
Current literature indicates that overall cardiovascular outcomes and perioperative mortality rates are not significantly different between regional and general anesthesia in major lower extremity arthroplasty. Furthermore, while general anesthesia may cause transient early postoperative cognitive dysfunction, long-term cognitive function is similar between the two modalities.
Thromboembolic Considerations
The effect of anesthetic choice on deep vein thrombosis (DVT) and pulmonary embolism (PE) remains a topic of intense academic debate.
* Sharrock et al. reported a slight, though not statistically significant, decrease in overall DVT and PE rates in patients receiving epidural anesthesia compared to general anesthesia.
* A randomized controlled trial by Mitchell et al. demonstrated no difference in overall thromboembolic disease but did reveal a significant decrease in proximal thrombus formation with epidural anesthesia.
The postulated benefits of epidural anesthesia include:
1. Sympathectomy-Induced Vasodilation: Results in increased lower extremity blood flow, reducing venous stasis.
2. Hemodilution and Decreased Viscosity: Further mitigates the Virchow's triad component of stasis.
3. Fibrinolytic Effect: Although postulated, studies (including those by Sharrock et al.) comparing epidural and general anesthesia have shown no significant difference in intraoperatively obtained blood markers for fibrinolysis or thrombogenesis.
Postoperative Analgesia via Epidural
A major advantage of epidural anesthesia is the ability to leave an indwelling catheter for 48 to 72 hours postoperatively for continuous pain control. Pettine et al. demonstrated that TKA patients required significantly lower total narcotic doses when continuous epidural bupivacaine was utilized.
Pitfall: Continuous epidural analgesia requires rigorous monitoring. Potential side effects include pruritus, urinary retention, nausea, vomiting, respiratory depression, and the rare but catastrophic formation of an epidural hematoma.
CRITICAL CONTRAINDICATION: The concurrent use of low-molecular-weight heparin (LMWH) for DVT prophylaxis alongside an indwelling postoperative epidural catheter is strictly not recommended due to the exponentially increased risk of epidural hematoma, which can lead to irreversible spinal cord compression and disastrous neurological sequelae.
SURGICAL APPROACH AND POSITIONING
Meticulous surgical technique begins with proper patient positioning and a well-executed surgical approach.
Patient Positioning
- The patient is placed supine on the operating table.
- A well-padded tourniquet is applied to the proximal thigh. (Note: The use of a tourniquet is surgeon-dependent; some prefer "tourniquet-less" surgery to reduce postoperative pain and quadriceps inhibition).
- A lateral post or sandbag is placed at the level of the greater trochanter to prevent external rotation of the hip.
- A foot piece or leg holder is utilized to allow the knee to be flexed past 90 degrees and held securely during bone preparation.
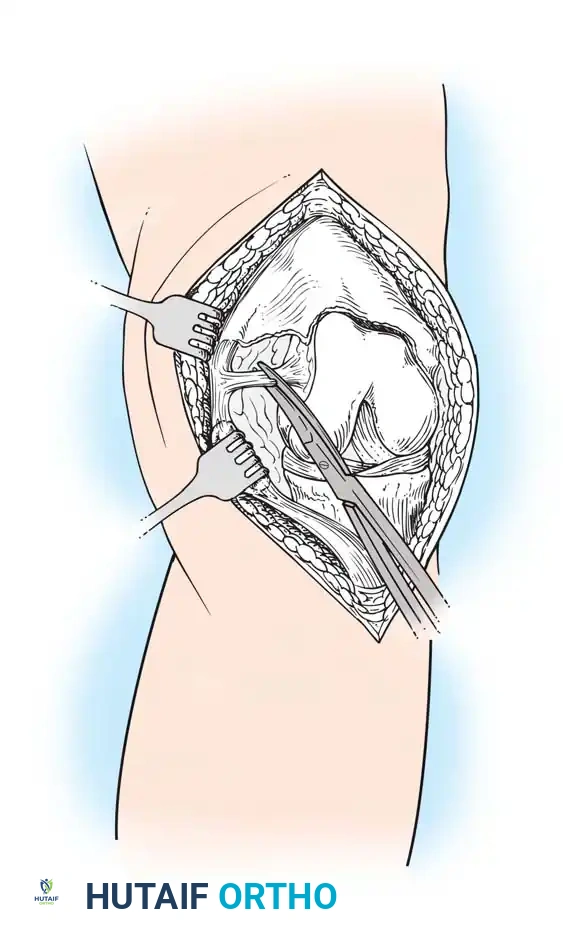
The Medial Parapatellar Approach
The medial parapatellar arthrotomy remains the gold standard and most widely utilized approach for TKA, providing unparalleled exposure to all three compartments of the knee.
Surgical diagram illustrating the standard anterior midline skin incision transitioning into the deep medial parapatellar arthrotomy.
Step-by-Step Execution:
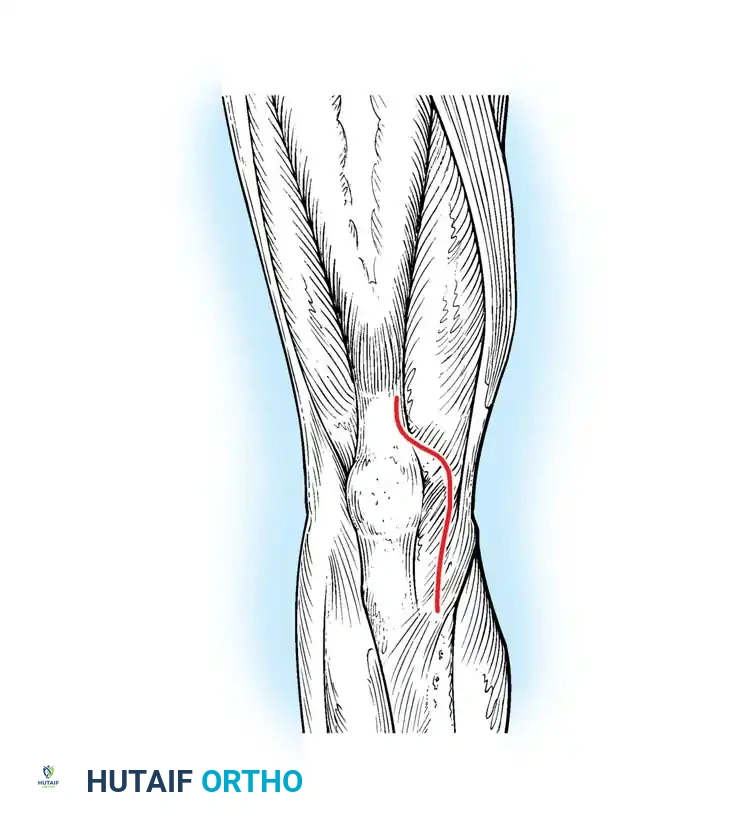
1. Skin Incision: A longitudinal midline incision is made, starting approximately 3-4 cm proximal to the superior pole of the patella, extending distally over the patella, and terminating just medial to the tibial tubercle.
2. Fascial Dissection: Full-thickness fasciocutaneous flaps are elevated medially and laterally to expose the extensor mechanism, preserving the prepatellar bursa where possible to minimize postoperative skin necrosis.
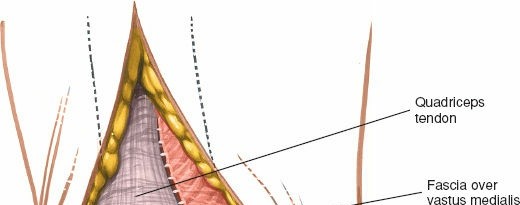
3. Arthrotomy: The deep incision begins proximally in the quadriceps tendon, leaving a 3-4 mm cuff of tendon attached to the vastus medialis obliquus (VMO) to facilitate robust closure.
4. Patellar Dissection: The incision is carried distally around the medial border of the patella (leaving a 2-3 mm capsular cuff) and extends distally along the medial border of the patellar tendon to the tibial tubercle.
5. Exposure: The patella is either everted or laterally subluxated (depending on surgeon preference and tissue tension). The retropatellar fat pad is partially excised to visualize the lateral tibial plateau and lateral meniscus.
6. Soft Tissue Releases: Depending on the preoperative deformity (varus vs. valgus), sequential soft tissue releases are performed to balance the flexion and extension gaps prior to final bone resection.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of a TKA relies heavily on a structured, evidence-based postoperative protocol designed to accelerate recovery, manage pain, and prevent complications.
Multimodal Pain Management
To minimize opioid consumption and its associated side effects (ileus, delirium, respiratory depression), a multimodal analgesic pathway is standard of care. This typically includes:
* Preoperative administration of gabapentinoids (e.g., pregabalin) and acetaminophen.
* Intraoperative periarticular local anesthetic infiltration (e.g., liposomal bupivacaine, ropivacaine mixed with epinephrine and ketorolac) injected into the posterior capsule, collateral ligaments, and extensor mechanism.
* Postoperative scheduled NSAIDs (if renal function permits), acetaminophen, and breakthrough short-acting opioids.
Venous Thromboembolism (VTE) Prophylaxis
Given the high risk of DVT/PE following TKA, chemical prophylaxis is mandatory. The choice of agent depends on patient risk stratification:
* Standard Risk: Aspirin (81 mg twice daily) has become the preferred agent for standard-risk patients due to its efficacy, low cost, and minimal bleeding risk.
* High Risk: Patients with a history of VTE or known hypercoagulable states require aggressive prophylaxis with LMWH (e.g., Enoxaparin), Direct Oral Anticoagulants (DOACs like Apixaban), or Warfarin. Mechanical prophylaxis (sequential compression devices) should be used universally while the patient is immobile.
Early Mobilization and Discharge
Modern rapid-recovery protocols emphasize mobilization on the day of surgery (Postoperative Day 0). Early weight-bearing as tolerated with an assistive device promotes venous return, reduces the risk of atelectasis, and improves psychological well-being.
Discharge criteria require the patient to demonstrate independent transfers, safe ambulation on level surfaces and stairs, adequate pain control on oral medications, and no evidence of surgical site complications. With optimized preoperative evaluation and modern surgical techniques, many TKA procedures are now safely transitioning to the outpatient or short-stay setting.
You Might Also Like