Mastering Knee Arthroplasty: Indications, Biomechanics, and Surgical Principles
Key Takeaway
Total knee arthroplasty (TKA) and unicondylar knee arthroplasty (UKA) are highly successful interventions for end-stage knee arthritis. This comprehensive guide details the strict indications, absolute and relative contraindications, and biomechanical principles governing patient selection. It explores the nuances of patellar resurfacing and simultaneous bilateral TKA, providing orthopedic surgeons with evidence-based frameworks to optimize surgical outcomes, minimize complications, and ensure long-term implant survivorship in diverse patient populations.
TRICOMPARTMENTAL TOTAL KNEE ARTHROPLASTY (TKA)
Indications and Patient Selection
The paramount indication for tricompartmental Total Knee Arthroplasty (TKA) is the alleviation of recalcitrant pain secondary to advanced arthropathy, presenting with or without significant angular deformity. However, the diagnosis of intrinsic knee pathology must be rigorous. Surgeons must systematically seek out and exclude extrinsic sources of knee and leg pain. Differential diagnoses to eliminate include radicular pain from lumbar spondylosis, referred pain from ipsilateral hip osteoarthritis, peripheral vascular claudication, isolated meniscal pathology, and localized bursitis.
Radiographic findings (e.g., osteophytes, subchondral sclerosis, cysts, and joint space narrowing) must strictly correlate with a clear clinical impression of end-stage knee arthritis. Patients who lack complete cartilage space loss prior to surgery consistently demonstrate lower satisfaction rates and suboptimal clinical outcomes post-TKA.
Before surgical intervention is entertained, a comprehensive regimen of conservative modalities must be exhausted. This includes nonsteroidal anti-inflammatory drugs (NSAIDs), targeted intra-articular injections (corticosteroids or viscosupplementation), activity modification, physical therapy, and the use of ambulatory aids such as a cane.
Because a knee prosthesis has a finite expected survivorship that is inversely proportional to the patient's activity level, TKA is classically indicated in older, more sedentary patients. However, it is also definitively indicated in younger patients whose function is severely curtailed by systemic inflammatory arthropathies (e.g., rheumatoid arthritis) involving multiple joints. Duffy, Trousdale, and Stuart reported an exceptional 99% survivorship at 10 years and 95% at 15 years in patients younger than 55 years old with cemented TKAs, the majority of whom carried a primary diagnosis of rheumatoid arthritis.
Other specific indications include:
* Osteonecrosis: Subchondral collapse of a femoral condyle.
* Crystalline Arthropathy: Severe, debilitating pain from chondrocalcinosis and pseudogout in elderly patients, occasionally justifying TKA even in the absence of complete joint space obliteration.
* Isolated Severe Patellofemoral Arthritis: In rare elderly cases, TKA is justified over patellectomy due to vastly superior functional outcomes. (Note: Newer patellofemoral arthroplasty designs exist but currently lack robust long-term follow-up).
Clinical Pearl: Deformity can supersede pain as the principal indication for TKA in patients with moderate arthritis. When a flexion contracture progresses beyond 20 degrees, the gait cycle is significantly hampered. Early intervention prevents the need for highly constrained prostheses.
As varus or valgus laxity becomes severe, a constrained condylar prosthesis becomes mandatory to prevent coronal plane instability. Intervening before this profound degree of laxity develops allows the surgeon to utilize an unconstrained (posterior-stabilized or cruciate-retaining) prosthesis, which boasts a more favorable long-term survivorship.
Contraindications to TKA
Patient optimization is the cornerstone of arthroplasty success. Contraindications must be strictly respected to avoid catastrophic failure.
Absolute Contraindications:
* Recent or current knee sepsis.
* A remote source of ongoing, untreated infection (e.g., severe dental abscess, untreated urinary tract infection).
* Extensor mechanism discontinuity or severe, irreparable dysfunction.
* Recurvatum deformity secondary to profound muscular weakness or paralysis.
* The presence of a painless, well-functioning knee arthrodesis.
Relative Contraindications:
* Severe medical comorbidities compromising anesthetic tolerance or the metabolic demands of wound healing.
* Inability to participate in the rigorous postoperative rehabilitation required for a favorable functional outcome.
* Significant atherosclerotic peripheral vascular disease of the operative extremity.
* Active skin conditions (e.g., psoriasis) directly within the operative field.
* Venous stasis disease with a history of recurrent cellulitis.
* Neuropathic (Charcot) arthropathy.
* Morbid obesity (BMI > 40), which exponentially increases infection and aseptic loosening risks.
* History of osteomyelitis in the proximity of the knee.
Biomechanics, Positioning, and Surgical Approach
Biomechanics: The goal of TKA is to restore the mechanical axis of the lower extremity (typically 0 degrees, passing through the center of the hip, knee, and ankle) and to achieve balanced flexion and extension gaps.
Positioning: The patient is positioned supine on the operating table. A tourniquet is applied to the proximal thigh. The leg is placed in a specialized leg holder or over a sandbag to allow dynamic flexion past 120 degrees and full extension.
Surgical Approach (Step-by-Step):
1. Incision: A standard anterior midline longitudinal incision is made, extending from the proximal pole of the patella to the tibial tubercle.
2. Arthrotomy: A medial parapatellar arthrotomy is the gold standard. The incision skirts the medial border of the patella and extends proximally into the quadriceps tendon, leaving a small cuff of tendon for later repair.
3. Exposure: The patella is everted or laterally subluxated. The fat pad is partially excised to visualize the lateral meniscus and tibial plateau.
4. Bone Preparation:
* Femur: The intramedullary canal is accessed. The distal femoral cut is made at a pre-calculated valgus angle (usually 5 to 7 degrees) to the anatomical axis. Anterior, posterior, and chamfer cuts are executed using a sizing block.
* Tibia: An extramedullary alignment guide is typically used. The proximal tibia is resected perpendicular to the mechanical axis in the coronal plane, with a posterior slope (usually 3 to 7 degrees) matching the native anatomy or implant design.
5. Soft Tissue Balancing: Osteophytes are meticulously removed. The extension and flexion gaps are measured. Sequential soft tissue releases (e.g., medial collateral ligament for varus knees; posterolateral corner/iliotibial band for valgus knees) are performed until symmetric, rectangular gaps are achieved.
6. Implantation: Trial components are placed to assess tracking, stability, and range of motion. Once optimized, the definitive components are cemented into place using polymethylmethacrylate (PMMA) bone cement.
Surgical Warning: Failure to adequately balance the flexion and extension gaps will result in kinematic instability, accelerated polyethylene wear, and early aseptic loosening.
Postoperative Protocol
- Day 0-1: Immediate weight-bearing as tolerated (WBAT) with an assistive device. Initiation of active and passive range of motion (ROM) exercises. Deep vein thrombosis (DVT) prophylaxis (e.g., low-molecular-weight heparin, aspirin, or direct oral anticoagulants) is commenced.
- Weeks 1-6: Intensive physical therapy focusing on achieving full terminal extension and flexion >110 degrees. Quadriceps strengthening is paramount.
- Months 3-12: Return to low-impact activities (swimming, cycling, golf). High-impact activities (running, jumping) are permanently discouraged to preserve polyethylene longevity.
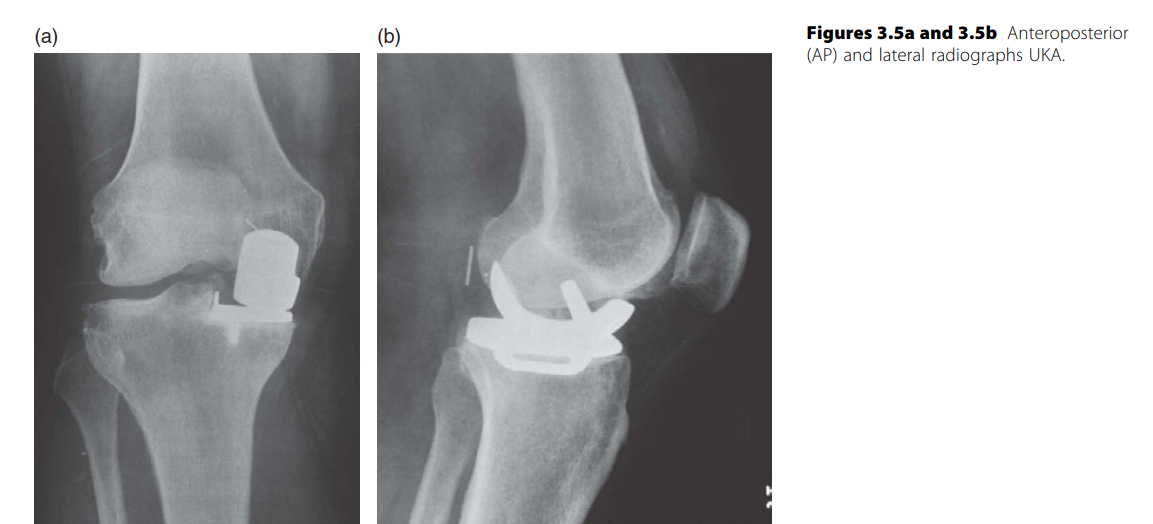
UNICONDYLAR KNEE ARTHROPLASTY (UKA)
Indications and Patient Selection
Unicondylar Knee Arthroplasty (UKA) has seen a resurgence, driven by minimally invasive techniques that facilitate outpatient surgery and rapid recovery. Ten-year follow-up studies of established UKA designs—such as the Oxford mobile-bearing knee (Biomet) and the Miller-Galante knee (Zimmer)—demonstrate survivorship approaching that of TKA in appropriately selected patients. However, most authors caution that UKA survivorship into the second decade rarely parallels TKA.
UKA is currently advocated for two distinct patient populations:
1. The Elderly, Thin Patient: Individuals with isolated unicompartmental osteoarthritis who would otherwise undergo TKA. Benefits include shorter rehabilitation, greater postoperative ROM, less blood loss, and preservation of the cruciate ligaments, yielding a more "natural-feeling" knee. Berger et al. reported a 10-year survivorship of 98% with a cemented UKA design in older patients using stringent selection criteria.
2. The Younger, Active Patient: Individuals with unicompartmental disease using UKA as a "first" arthroplasty, often replacing High Tibial Osteotomy (HTO). Pennington et al. described an 11-year survivorship of 92% in patients younger than 60 years old, though 22% showed radiographic progression in the unresurfaced compartment.
Pitfall: The concept of UKA as a "bone-sparing" procedure that guarantees an uncomplicated future revision to TKA is heavily debated. While Levine et al. and McAuley et al. found contemporary UKA revisions straightforward (often requiring only standard stems or wedges), earlier studies by Padgett, Stern, and Insall found major osseous defects in 76% of knees at the time of revision.
Contraindications to UKA
The indications for UKA may be debated, but the contraindications are rigidly defined. According to the classic criteria by Kozinn and Scott, UKA is contraindicated in the presence of:
* Inflammatory arthritis (e.g., Rheumatoid Arthritis).
* Flexion contracture of 15 degrees or more.
* Preoperative arc of motion less than 90 degrees.
* Angular deformity >10 degrees varus or >5 degrees valgus (uncorrectable passively).
* Significant cartilaginous erosion in the contralateral weight-bearing compartment.
* Anterior Cruciate Ligament (ACL) deficiency.
* Exposed subchondral bone beneath the patella (severe patellofemoral OA).
Furthermore, obesity is a significant contraindication. Berend et al. demonstrated that a Body Mass Index (BMI) > 32, combined with technical errors, was the most significant predictor of early failure, citing a 20% failure rate in minimally invasive UKA procedures.
Surgical Technique and Surgeon Volume
The success of UKA is exquisitely sensitive to surgical technique. Stern, Becker, and Insall noted that only 6% of arthroplasty candidates meet the strict criteria for UKA. Because it is rarely indicated, low-volume surgeons may struggle to reproduce the excellent results published by high-volume reconstructive centers. Gioe and Bowman reported an 89% 10-year survivorship for UKA in a community hospital setting, compared to 95% for TKA during the same period.
Surgical Approach:
UKA is typically performed via a minimally invasive midvastus or limited medial parapatellar approach. The patella is not everted. Bone resection is minimal, aiming to resurface only the diseased compartment while meticulously preserving the ACL and the contralateral compartment. Overcorrection of the mechanical axis must be avoided; the knee should be left in slight varus (for medial UKA) to prevent accelerated degeneration of the preserved lateral compartment.
INDICATIONS FOR PATELLAR RESURFACING IN TKA
The role of universal versus selective patellar resurfacing remains one of the most fiercely debated topics in orthopedic surgery.
Universal Resurfacing
Proponents of universal resurfacing (Ranawat, Soudry, Enis) argue that it yields superior knee scores, reduces residual peripatellar pain, and improves quadriceps strength. A large retrospective study by Boyd et al. found patellofemoral complications in only 4% of resurfaced patients, compared to 12% in unresurfaced patients, with anterior knee pain being the primary culprit. Waters and Bentley’s prospective randomized study echoed this, showing a 25% incidence of anterior knee pain in unresurfaced patellae versus 5% in resurfaced ones.
Surgical Warning: Secondary resurfacing of a retained patella for postoperative anterior knee pain yields notoriously poor results. Muoneke et al. and Karnezis et al. demonstrated that pain relief after secondary resurfacing is vastly inferior to primary resurfacing and carries a higher risk of complications, including patellar fracture and arthrofibrosis.
Selective Resurfacing
Advocates for selective resurfacing (Abraham, Keblish, Barrack, Burnett) argue that complications related to the resurfaced patella (e.g., fracture, avascular necrosis, component loosening, extensor mechanism rupture) account for the majority of reoperations after TKA.
When utilizing a femoral component with an anatomically optimized trochlear groove, selective resurfacing yields equivalent clinical scores. Barrack et al. and Burnett et al. (in a 10-year prospective randomized study) found no statistical difference in anterior knee pain, functional scores, or revision rates between resurfaced and unresurfaced groups. They concluded that anterior knee pain is more closely related to femoral component design and rotational alignment than to the patella itself.
Criteria for Retaining the Native Patella (Scott and Reilly):
* Primary diagnosis of osteoarthritis (no inflammatory arthropathy).
* Satisfactory patellar cartilage without eburnated subchondral bone.
* Congruent patellofemoral tracking intraoperatively.
* Normal anatomical patellar shape.
* Lighter patient weight (lower BMI correlates with better outcomes in unresurfaced patellae).
SIMULTANEOUS BILATERAL TOTAL KNEE ARTHROPLASTY
Cost-Effectiveness and Indications
For patients with severe, symptomatic bilateral knee osteoarthritis, simultaneous bilateral TKA offers documented cost-effectiveness and logistical advantages. Simultaneous procedures can reduce total hospital charges by up to 58% due to decreased cumulative operative time and a single hospital admission. However, Lane et al. noted that 89% of simultaneous bilateral TKA patients required discharge to an inpatient rehabilitation facility, compared to only 45% of unilateral TKA patients, potentially offsetting some initial cost savings.
Complications and Risk Mitigation
The controversy surrounding simultaneous bilateral TKA centers on perioperative morbidity and mortality.
- Blood Loss and Coagulopathy: While some studies show equal total blood loss, Bould et al. demonstrated significantly higher acute blood loss in simultaneous procedures. Jankiewicz and Lane reported higher homologous blood transfusion requirements. Stern et al. noted profound postoperative thrombocytopenia on postoperative day two, reflecting the massive stress placed on the coagulation cascade.
- Thromboembolic Events: Wapner and Ritter et al. reported slightly higher prevalences of Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE) following simultaneous procedures, though cardiovascular mortality was not significantly increased.
- Fat Embolism Syndrome (FES): FES is a critical risk when bilateral intramedullary femoral alignment rods are utilized sequentially. Dorr et al. reported a 12% prevalence of FES (documented by hypoxemia and neurological changes) in simultaneous bilateral TKA.
Clinical Pearl: To mitigate the risk of Fat Embolism Syndrome during bilateral TKA, surgeons must meticulously vent the intramedullary canal. This is achieved by overdrilling the cortical entry hole, utilizing fluted intramedullary alignment rods, and avoiding excessive intramedullary pressurization during cementation.
For patients with significant cardiopulmonary comorbidities, staggering the two replacements is highly recommended. Sliva et al. endorsed a staged approach, separating the procedures by 4 to 7 days during a single hospital stay, noting that overall complication rates were lower than those reported for sequential bilateral TKA performed under a single anesthetic event. Careful patient selection, rigorous preoperative medical optimization, and meticulous surgical technique remain the ultimate determinants of success in bilateral joint reconstruction.
📚 Medical References
- knee arthroplasty, Clin Orthop Relat Res 269:70, 1991.
- Hoppenfeld S, deBoer P: Surgical exposures in orthopaedics: the anatomic approach, Philadelphia, 2003, Lippincott Williams & Wilkins. Insall JN: A midline approach to the knee, J Bone Joint Surg 53A:1584, 1971.
- Jones R: Disabilities of the knee-joint, Br Med J 2:169, 1916.
- Kaplan EB: Surgical approach to the lateral (peroneal) side of the knee joint, Surg Gynecol Obstet 104:346, 1957.
- Keblish PA: The lateral approach to the valgus knee: surgical technique and analysis of 53 cases with over two-year followup evaluation, Clin Orthop Relat Res 271:52, 1991.
- Kocher T: Textbook of operative surgery, 3rd ed, London, 1911, Adam & Charles Black (Translated by HJ Stiles, CB Paul). Kummel BM, Zazanis GA: Preservation of intrapatellar branch of saphenous nerve during knee surgery, Orthop Rev 3:43, 1974.
- Langenbeck B von: Über die Schussverletzungen des Huftgelenks, Arch Klin Chir 16:263, 1874.
- McConnell BE: A dynamic transpatellar approach to the knee, South Med J 69:557, 1976.
- McConnell JC: Paper presented at the Thirteenth Triennial Meeting of the Willis C Campbell Club, Memphis, Tenn, Oct 1985.
- Minkoff J, Jaffe L, Menendez L: Limited posterolateral surgical approach to the knee for excision of
You Might Also Like