Comprehensive Introduction and Patho-Epidemiology
Deformities of the hip in patients with cerebral palsy (CP) represent a complex, progressive continuum of pathology that ranges from mild, painless subluxation to complete, rigid dislocation accompanied by severe joint destruction, intractable pain, and profound impairment of mobility. Unlike developmental dysplasia of the hip (DDH), which is characterized by an intrinsic embryologic or fetal maldevelopment of the acetabulum and proximal femur, the hip in a child with cerebral palsy is almost universally anatomically normal at birth. The progressive deformity is entirely acquired and multifactorial, driven primarily by relentless spastic muscle imbalance, retained primitive reflexes, abnormal posturing, and secondary pelvic obliquity. This acquired dysplasia is a hallmark of the upper motor neuron lesion that defines CP, creating a dynamic environment where muscle forces actively deform the growing skeleton.
When a spastic hip begins to subluxate, the natural history is one of relentless, unidirectional progression; it rarely, if ever, improves without decisive, well-timed orthopedic intervention. The altered biomechanical forces across the joint, combined with delayed or absent physiological weight-bearing, lead to profound structural bony deformities. These typically manifest as progressive acetabular dysplasia (specifically posterosuperior deficiency), excessive femoral anteversion, an increased neck-shaft angle (coxa valga), and regional osteopenia. The lack of normal weight-bearing forces deprives the proximal femur and acetabulum of the physiological Wolff's Law remodeling necessary to develop a congruent, stable hip joint. Consequently, the femoral head is driven superolaterally, eroding the acetabular rim and creating a false acetabulum over time.
Hip pain is a paramount complaint among young adults with cerebral palsy, severely impacting their quality of life, sitting tolerance, and perineal care. In a landmark cross-sectional multicenter study by Hodgkinson et al., the prevalence of hip pain in 234 adult patients (mean age 28 years) was a staggering 47%. Progressive hip instability occurs in approximately 15% of all patients with CP, but this statistic belies the true risk profile, which is highly dependent on the severity of neurological involvement. The Gross Motor Function Classification System (GMFCS) is the most reliable predictor of hip displacement. Children classified as GMFCS Level I or II (independent ambulators) have a relatively low risk of displacement (less than 10%), whereas those in GMFCS Levels IV and V (dependent sitters and non-ambulators) face a displacement risk approaching 90%.
Sharrard historically noted that when nonspastic types of CP and hemiplegia were excluded, 92% of patients exhibited some degree of hip deformity. Lonstein and Beck further stratified this risk in a seminal natural history study, finding that hip subluxation and dislocation occurred in 7% of ambulators but up to 60% of dependent sitters. This epidemiological reality underscores the absolute necessity of rigorous, protocol-driven hip surveillance programs. Because early hip subluxation in CP is typically painless and masked by severe flexor and adductor contractures, clinical detection by physical examination alone is notoriously difficult and unreliable. Therefore, the contemporary orthopedic consensus dictates that all hips in patients with cerebral palsy must be considered abnormal and at risk until proven otherwise through serial radiographic evaluation.
Detailed Surgical Anatomy and Biomechanics
The pathoanatomy of the spastic hip is fundamentally a disorder of dynamic muscle imbalance leading to static bony deformity. In the typical spastic diplegic or quadriplegic patient, the adductors (adductor longus, brevis, magnus, and gracilis) and the flexors (iliopsoas, rectus femoris) are profoundly hypertonic and spastic. Conversely, the abductors (gluteus medius and minimus) and extensors (gluteus maximus) are relatively weak and overpowered. This chronic, unremitting imbalance results in a net force vector that drives the proximal femur into flexion, adduction, and internal rotation. Over time, this dynamic posturing inhibits the normal physiological varus and derotational remodeling of the proximal femur that occurs during the first decade of life.
Bobroff et al. demonstrated that with increasing age, the neck-shaft angle in children with CP paradoxically increases, contrasting sharply with the physiological varus remodeling seen in unaffected children. Furthermore, Baker et al. reviewed the radiographic appearance of 258 hips in 129 patients with CP, finding that only 21% were radiographically normal. Their analysis revealed valgus deformity of the femoral neck in 76%, increased acetabular roof obliquity in 62%, subluxation in 16%, dislocation in 12%, and varus deformity in a mere 2%. Baker postulated that prolonged spasticity of the adductor and flexor musculature leads to a relative overpowering of the abductors and extensors. This chronic imbalance causes growth inhibition of the greater trochanter, producing a relative valgus overgrowth of the proximal femur and a persistence of fetal femoral anteversion, which often exceeds 50 to 60 degrees.
Flexion Deformities and Gait Kinematics
Crouched gait—characterized by excessive flexion of the hip, knee, and ankle—is a hallmark kinematic abnormality of spastic diplegia and quadriplegia. Excessive hip flexion shifts the center of gravity anteriorly, which the patient compensates for by increasing lumbar lordosis, flexing the knees, and dorsiflexing the ankles. This creates a highly inefficient, energy-consuming gait pattern that places immense stress on the patellofemoral joint and the extensor mechanism.
It is imperative for the reconstructive surgeon to differentiate whether increased hip flexion is a primary deformity driven by iliopsoas spasticity or a secondary kinematic compensation for distal contractures (e.g., fixed knee flexion or ankle equinus). If an unrecognized fixed knee flexion contracture is present, an isolated hip flexor release will paradoxically weaken the hip, exacerbate the anterior center of gravity shift, and ultimately worsen the crouch gait. Comprehensive 3D gait analysis is often required to parse out these complex, multi-level kinematic derangements prior to surgical intervention.
Pseudoadduction vs. True Adduction
A frequent source of clinical confusion during physical examination is differentiating a flexion-internal rotation deformity (often termed "pseudoadduction") from an isolated true adduction contracture. Children with pseudoadduction typically sit in the classic "W" position: hips flexed to 90 degrees and maximally internally rotated, knees maximally flexed, and feet externally rotated.

In pseudoadduction, secondary bony deformities such as increased femoral anteversion, external tibial torsion, and planovalgus feet (the so-called "miserable malalignment syndrome") are almost universally present. When the hip is extended, the apparent adduction often resolves, revealing that the primary issue is rotational and sagittal, not coronal. In a true isolated adduction contracture, these secondary torsional deformities are less pronounced, and the restriction in abduction is present regardless of the hip's position in the sagittal plane.
Radiographic Surveillance and the Migration Percentage
In 1969, Beals introduced a practical radiographic method for quantifying hip subluxation, which Reimers later popularized as the Migration Percentage (MP). This metric remains the international gold standard for monitoring hip displacement in CP.
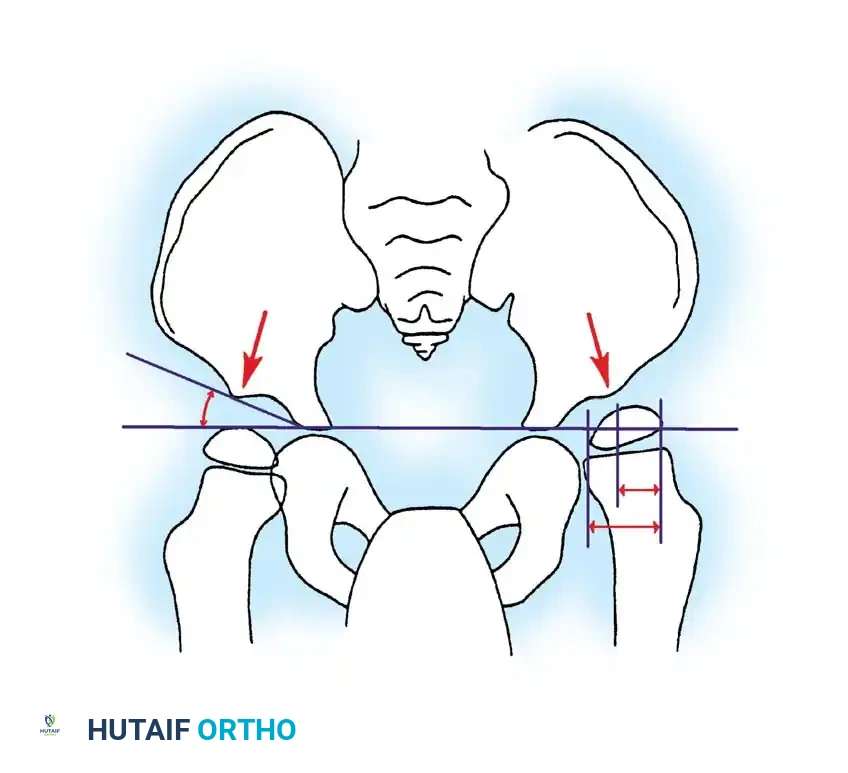
The migration percentage is calculated on an anteroposterior (AP) pelvis radiograph by drawing Hilgenreiner's line (connecting the bilateral triradiate cartilages) and dropping perpendicular lines (Perkins' lines) at the lateral margins of the ossified acetabular sourcil. The width of the femoral head uncovered (lateral to Perkins' line) is divided by the total width of the femoral head and multiplied by 100. A normal MP is less than 30-33%. Subluxation is defined as an MP between 33% and 99%, and dislocation is an MP of 100%. More critical than a single absolute value is the velocity of change observed within a given patient over time; an MP increasing by more than 10% per year is a dire prognostic sign mandating immediate surgical consideration.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in the spastic hip is dictated by the patient's age, GMFCS level, ambulatory status, Migration Percentage, and the presence of articular cartilage damage. The overarching goal is to maintain a painless, mobile, and located hip joint that allows for optimal function, whether that function is community ambulation or comfortable seating in a custom wheelchair.
Soft-tissue releases (adductor and iliopsoas lengthening) are prophylactic procedures. They are indicated early in the disease process, typically in children under 8 years of age, before irreversible bony deformity has occurred. The ideal candidate has an MP between 25% and 50% and restricted abduction (less than 30 degrees in extension). However, surgeons must counsel families that soft-tissue release is often a temporizing measure; literature demonstrates that up to 58% of these patients will eventually require bony reconstruction as they grow.
Bony reconstruction—comprising a Varus Derotational Osteotomy (VDRO) of the proximal femur and a pelvic osteotomy (e.g., Dega or San Diego)—is the definitive management for established dysplasia. It is indicated when the MP exceeds 50%, when there is significant acetabular dysplasia (acetabular index > 25 degrees), or when soft-tissue releases have failed. Salvage procedures (resection arthroplasty, valgus osteotomy, or total hip arthroplasty) are reserved for mature patients with painful, chronically dislocated hips where the articular cartilage is destroyed, rendering reconstructive containment impossible or doomed to failure.
| Intervention Category | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Prophylactic Soft-Tissue Release | Age < 8 years; MP 25%–50%; Abduction < 30°; Minimal bony dysplasia. | MP > 60%; Severe acetabular dysplasia; Fixed bony deformity. | Previous failed soft-tissue release; Athetoid/Dystonic CP (high recurrence). |
| Reconstructive Bony Surgery (VDRO + Pelvic Osteotomy) | MP > 50%; Progressive subluxation despite soft-tissue release; Coxa valga > 150°; Acetabular dysplasia. | Destroyed articular cartilage; Stiff, painful, chronically dislocated hip in an older child/adult. | Severe osteopenia precluding hardware fixation; Uncontrolled seizure disorder. |
| Salvage Procedures (Castle, McHale, THA) | Painful, rigid, chronically dislocated hip; Severe cartilage destruction; Inability to maintain perineal hygiene. | Painless dislocated hip with acceptable sitting tolerance (leave alone). | Active local or systemic infection; Severe malnutrition (albumin < 3.0). |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful hip reconstruction in cerebral palsy. The clinical examination must be exhaustive, evaluating not only the hip but the entire lower extremity and spine. The Thomas test is utilized to quantify fixed hip flexion contractures, while the Duncan-Ely test assesses rectus femoris spasticity. Ryder's test (trochanteric prominence angle test) provides a clinical estimation of femoral anteversion, which must be correlated with radiographic findings. Spinal alignment must be scrutinized, as a rigid scoliotic curve driving pelvic obliquity will rapidly compromise a reconstructed hip if left unaddressed.
Radiographic templating is mandatory for bony reconstruction. A true AP pelvis and a frog-leg lateral are standard. The AP pelvis is used to measure the MP, the acetabular index, and the center-edge angle of Wiberg. An AP radiograph with the hips in maximal abduction and internal rotation is highly valuable; if the femoral head reduces concentrically on this view, the hip is considered "reconstructible" via a VDRO and pelvic osteotomy. If the head does not reduce, an open reduction with capsulorrhaphy will be required concomitantly. Advanced imaging, such as 3D computed tomography (CT), is increasingly utilized to precisely quantify femoral anteversion and map the specific topography of the acetabular deficiency, which is almost universally posterosuperior in CP.
Patient positioning in the operating room requires meticulous attention to detail. The patient is placed supine on a radiolucent Jackson or OSI table to allow for unencumbered fluoroscopic imaging.

For soft-tissue releases, the lower extremities are prepped and draped freely from the toes to the inferior costal margin. The perineum is isolated with a sterile adhesive drape (e.g., U-drape) to allow full, unrestricted intraoperative range of motion, particularly maximum abduction to assess the adequacy of the adductor release. For bony reconstructions, a bump is placed under the ipsilateral sacrum to elevate the hemipelvis, facilitating the anterior approach to the hip and the ilium. Bilateral procedures are common; thus, a wide, sterile field encompassing both entire lower extremities and the entire pelvis is standard protocol.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention in the spastic hip is frequently a multilevel, bilateral endeavor. The following sections detail the masterclass techniques for soft-tissue releases and complex bony reconstructions.
Soft-Tissue Management: Adductor Tenotomy and Release
Adduction is the most common primary deformity. For mild contractures, an isolated adductor longus tenotomy is sufficient. More severe contractures require the release of the gracilis and the anterior half of the adductor brevis.
Incision and Dissection:
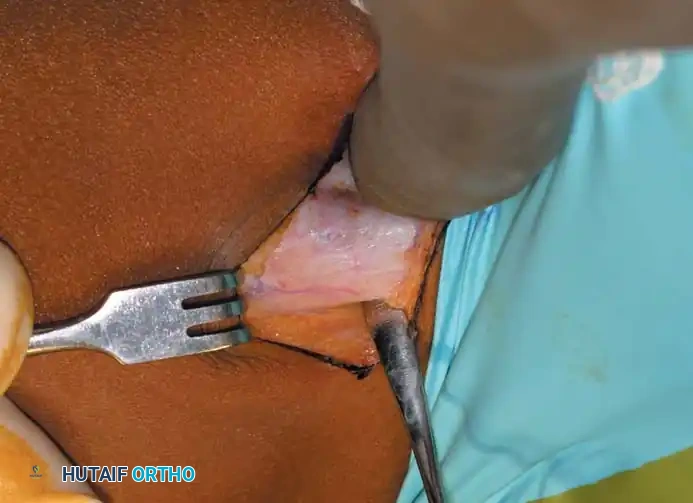
Palpate the taut adductor longus tendon at its origin on the pubis. Make a 3-cm transverse incision centered over the tendon, approximately 1 cm distal to its origin.
Dissect bluntly through the subcutaneous adipose tissue to identify the underlying adductor fascia. Make a longitudinal incision in the fascia to expose the tendinous portion of the adductor longus.
Muscle Release:
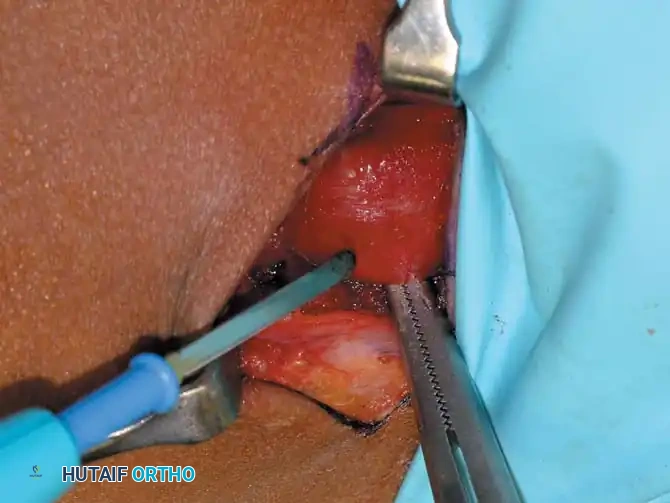
Isolate the adductor longus tendon and resect a small 1-cm portion using electrocautery to prevent bridging and recurrence. If the hip does not abduct to at least 45 degrees in extension, sequentially identify and release the gracilis and the anterior half of the adductor brevis.
Meticulously avoid injury to the anterior branch of the obturator nerve, which lies in the fascial interval between the adductor longus and adductor brevis. Do not perform an obturator neurectomy; historical data proves this frequently leads to an iatrogenic, irreversible abduction contracture.
Closure:
Once adequate abduction is achieved, irrigate the wound. Close the adductor fascia meticulously to prevent unsightly postoperative skin dimpling, a common cosmetic complaint. Close the subcutaneous tissue and skin in a standard layered fashion.
Management of Hip Flexion Contractures: Iliopsoas Recession
Hip flexion contractures between 15 and 30 degrees are typically managed with an iliopsoas lengthening via an intramuscular recession over the pelvic brim. In ambulatory children, a complete iliopsoas tenotomy at the lesser trochanter is strictly contraindicated, as it leads to profound hip flexion weakness and an inability to clear the foot during swing phase.
Approach and Recession:
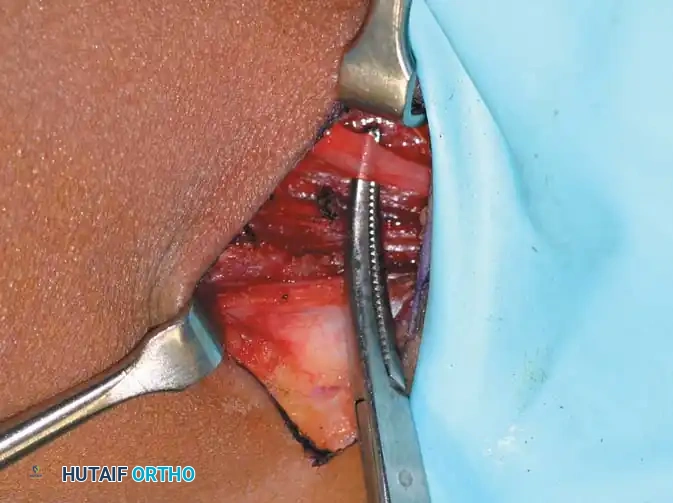
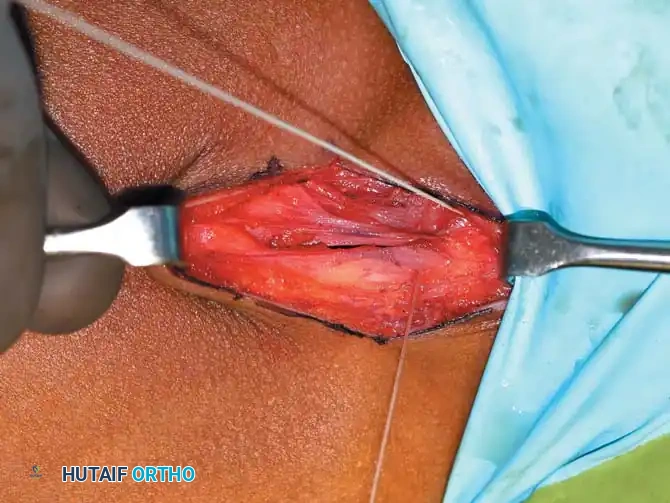
Make a 5-cm "bikini" incision centered medial to and 2 cm distal to the anterior superior iliac spine (ASIS). Develop the internervous interval between the tensor fasciae latae (superior gluteal nerve) and the sartorius (femoral nerve). Palpate the pelvic brim medial and inferior to the rectus origin. Place a right-angle retractor on the lateral aspect of the iliopsoas muscle and retract medially to protect the femoral nerve.
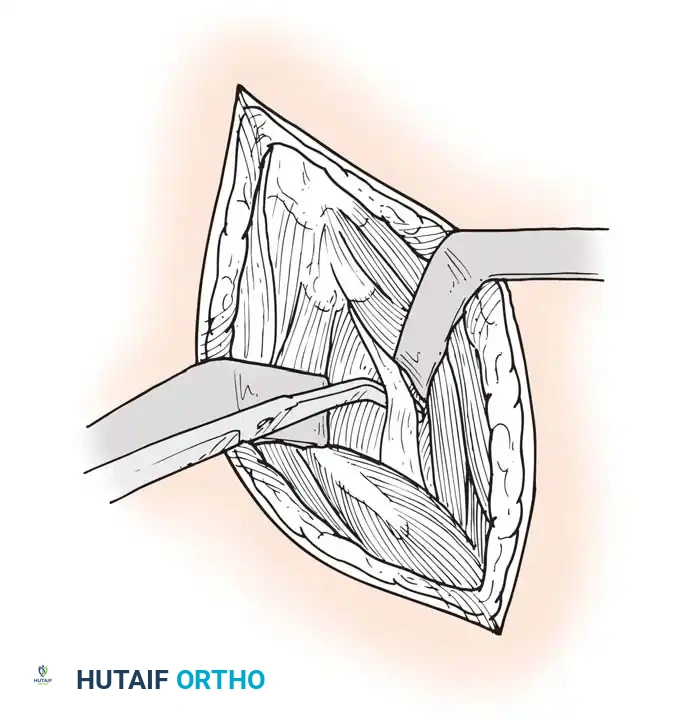
Isolate the tendinous portion of the psoas from the underlying muscle belly. Transect the tendon under direct vision, leaving the underlying muscle fibers intact to maintain continuity and preserve active hip flexion strength.
Bony Reconstruction: The Pericapsular Pelvic Osteotomy (Dega/San Diego)
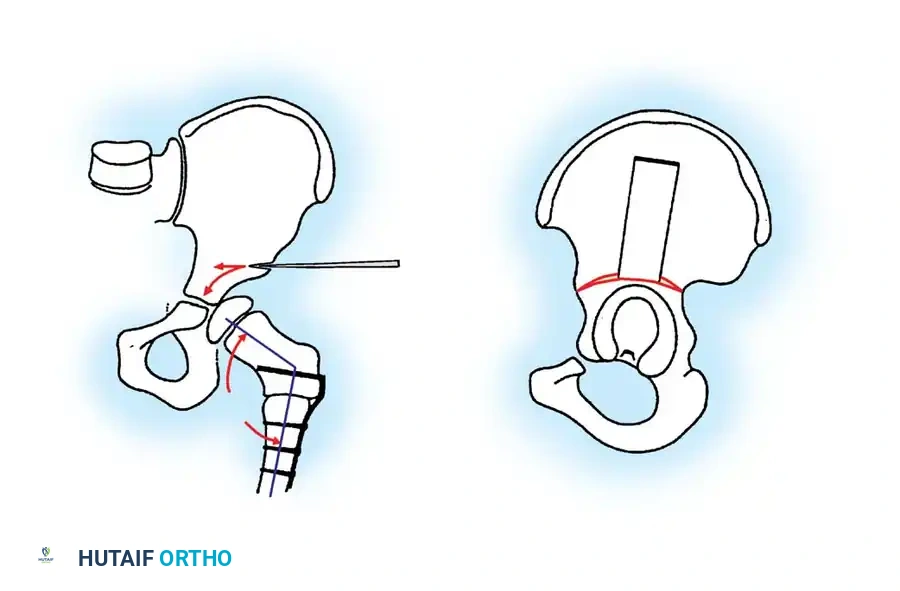
When soft-tissue releases fail, or a child presents late with an MP > 50%, bony reconstruction is mandatory. The Dega or San Diego Pericapsular Osteotomy is the workhorse procedure. It is an incomplete transiliac osteotomy that hinges on the triradiate cartilage, allowing for multidirectional (anterior, lateral, and posterior) coverage of the femoral head.
The Iliac Cut:
Following a standard anterior Smith-Petersen approach to the hip, the inner and outer tables of the ilium are exposed subperiosteally. An incomplete osteotomy is initiated just above the AIIS and directed posteriorly toward the greater sciatic notch.
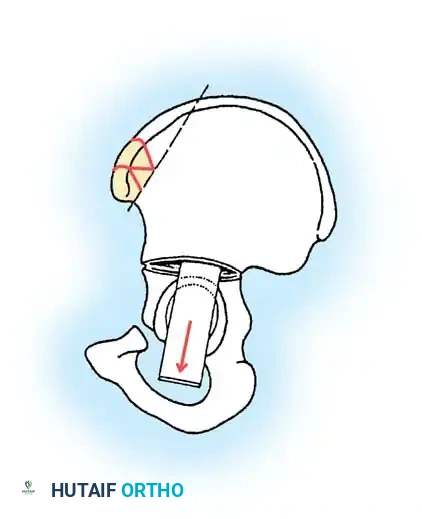
Hinging the Osteotomy:
The osteotomy is carefully advanced using curved osteotomes. It is critical to leave the medial cortex near the sciatic notch and the thick periosteum over the triradiate cartilage intact. This intact medial hinge is the biomechanical crux of the procedure, providing inherent stability.
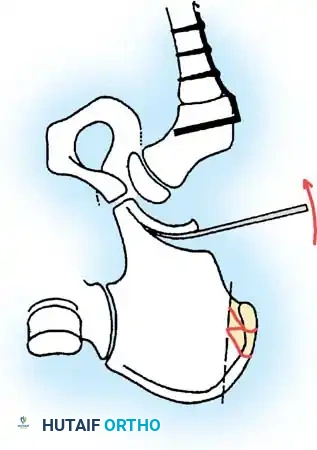
Levering and Down-Grafting:
Using a lamina spreader or a broad osteotome, the distal fragment (the acetabular roof) is levered laterally, anteriorly, and inferiorly to cover the femoral head. The degree of correction is titrated under live fluoroscopy until the sourcil is horizontal and the femoral head is fully contained.
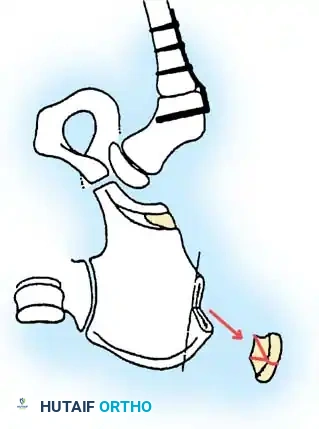
Graft Preparation and Placement:
Triangular or trapezoidal structural bone grafts are harvested from the proximal iliac crest.
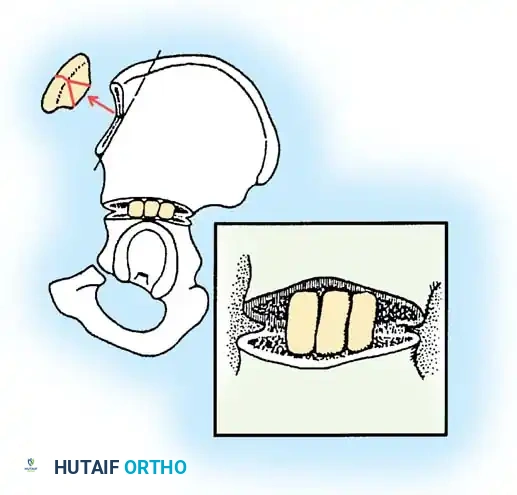
These structural grafts are impacted tightly into the osteotomy gap. Because the osteotomy hinges on the flexible triradiate cartilage, the grafts are held firmly in place under immense compressive forces without the need for internal hardware fixation (K-wires or plates).
Final Assessment:
The final construct provides robust, stable anterolateral and posterior coverage of the femoral head, dramatically improving the sourcil angle, normalizing the Migration Percentage, and restoring the biomechanical fulcrum of the hip joint.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of the spastic hip is fraught with potential complications, driven by the patient's underlying osteopenia, poor nutritional status, and relentless spasticity. The complication profile must be discussed extensively with the family during the informed consent process.
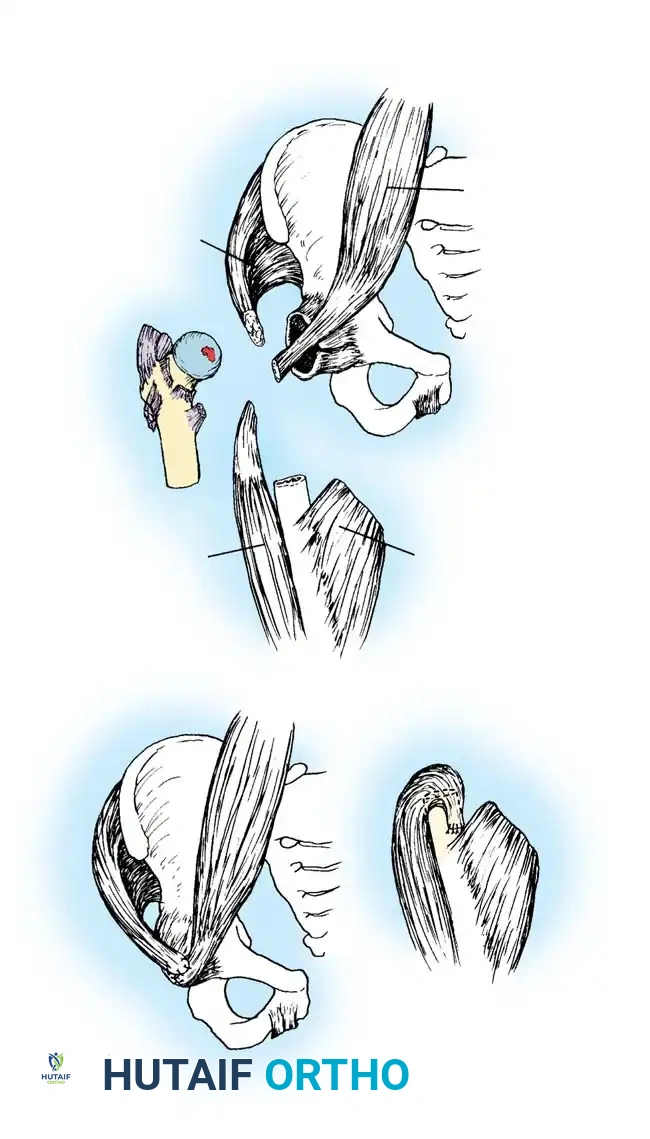
Avascular necrosis (AVN) of the femoral head is the most devastating complication following reconstructive surgery, occurring in up to 5-10% of cases involving open reduction and VDRO. It is typically caused by excessive tension on the medial circumflex femoral artery when reducing a chronically dislocated hip or by direct injury to the retinacular vessels during the femoral osteotomy. To mitigate this risk, aggressive femoral shortening (often 1-2 cm) is mandatory during the VDRO to decompress the joint and allow a tension-free reduction.
Recurrence of subluxation is another major concern, particularly in younger children (under 5 years) and those with GMFCS Level V involvement. Recurrence rates can approach 15-20% at 10-year follow-up, necessitating ongoing radiographic surveillance until skeletal maturity. In cases of severe recurrence or presentation of a painful, rigid, dislocated hip in a mature patient, salvage procedures are indicated. The McHale procedure (proximal femoral resection combined with a valgus osteotomy) or the Castle procedure (extensive proximal femoral resection and interposition arthroplasty) are utilized to eliminate bone-on-bone contact and restore sitting tolerance. Total Hip Arthroplasty (THA) is an option in high-functioning adults but carries a significantly elevated risk of dislocation and aseptic loosening compared to the non-CP population.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Management Strategy |
|---|---|---|---|
| Avascular Necrosis (AVN) | 5% – 10% | Excessive joint tension; Vascular injury during VDRO. | Perform adequate femoral shortening; Avoid extreme internal rotation casting. |
| Recurrent Subluxation | 10% – 20% | Unrelenting spasticity; Inadequate initial correction; Young age at surgery. | Ensure robust pelvic osteotomy; Maintain postoperative abduction bracing; Consider botulinum toxin. |
| Iatrogenic Abduction Contracture | 2% – 5% | Overzealous adductor release; Obturator neurectomy. | Avoid obturator neurectomy; Preserve posterior adductor magnus. |
| Hardware Failure / Non-union | 3% – 7% | Severe osteopenia; Uncontrolled seizures; Inadequate fixation. | Use locking blade plates; Supplement with spica casting; Optimize Vitamin D/Calcium preoperatively. |
| Worsening Crouch Gait | Variable | Isolated psoas tenotomy without addressing distal knee/ankle contractures. | Perform comprehensive 3D gait analysis; Execute multi-level surgery (SEMLS) concurrently. |
Phased Post-Operative Rehabilitation Protocols
Postoperative management is entirely dictated by the extent of the surgical intervention, the stability of the fixation, and the patient's baseline functional status. The rehabilitation protocol must be a multidisciplinary effort involving the orthopedic surgeon, physical therapists, orthotists, and the patient's family.
For isolated soft-tissue releases (adductor tenotomy and iliopsoas recession), patients are typically placed in a removable abduction pillow or a custom A-frame orthosis immediately postoperatively. Rigid casting is avoided to prevent muscle atrophy and joint stiffness. The primary goal in the first 4 weeks is to maintain the newly acquired range of motion. Physical therapy is initiated on postoperative day one, focusing on gentle, passive range of motion, particularly hip abduction and extension. Patients are encouraged to use standing frames as soon as tolerated to stretch the flexors and provide weight-bearing stimulus to the long bones.
For patients undergoing extensive bony reconstruction (pelvic osteotomies combined with femoral varus derotational osteotomies), immobilization is mandatory. A 1.5-spica cast is usually applied in the operating room, positioning the hips in 20-30 degrees of abduction, neutral rotation, and slight flexion. This cast remains in place for 4 to 6 weeks to ensure rigid immobilization, protect the osteotomy sites, and facilitate graft incorporation.
Following cast removal, clinical and radiographic evaluation is performed to confirm early bony union. The patient is then transitioned to an abduction orthosis (worn primarily at night) and aggressive physical therapy commences. Therapy focuses on restoring baseline mobility, maximizing the newly acquired joint mechanics, and integrating the patient back into their functional ambulatory or sitting orthoses. Hydrotherapy is highly beneficial during this phase, as the buoyancy allows for early mobilization with reduced joint loading. Routine radiographic surveillance (AP pelvis) must continue every 6 to 12 months
