General Treatment of Nonunions: A Comprehensive Surgical Guide
Key Takeaway
The successful treatment of fracture nonunions requires a meticulous balance of biomechanical stability and biological vitality. This comprehensive guide details the evidence-based management of hypertrophic and atrophic nonunions, exploring advanced classification systems, orthobiologic adjuncts, and step-by-step surgical techniques. From closed intramedullary nailing to complex Ilizarov bone transport, orthopedic surgeons will find essential protocols to optimize patient outcomes and achieve definitive bony union.
INTRODUCTION TO NONUNION MANAGEMENT
The management of fracture nonunions represents one of the most formidable challenges in orthopedic surgery. Orthopaedic surgeons can choose from numerous surgical and nonsurgical methods that vary greatly in their invasiveness and propensity for minor and catastrophic complications. The U.S. Food and Drug Administration (FDA) classically defines a nonunion as a fracture that is at least nine months old and has shown no radiographic signs of healing for three consecutive months. However, clinically, a nonunion is declared when the surgeon determines that the fracture has no potential to heal without further intervention.
The treatment of nonunions has advanced significantly with improvements in electrical and electromagnetic stimulation, low-intensity pulsed ultrasound (LIPUS), and advanced bone grafting techniques. The Ilizarov external fixator continues to be an effective and versatile method for the treatment of difficult nonunions complicated by complex deformity, infection, and bone loss. Improvements in internal fixation systems—particularly locking plate technology and advanced intramedullary nails—have provided sufficiently stable fixation to allow active and passive range of motion of adjacent joints, promoting complete functional recovery in addition to bony union.
Research also continues to expand the armamentarium of orthobiologics, including bone grafts, bone graft substitutes, bone morphogenetic proteins (BMPs), and novel biomaterials for bone regeneration.
Clinical Pearl: In a situation with equal risks and benefits, the simplest, most easily tolerated method should be chosen. Successful treatment of a nonunion rarely consists of only one method or surgical technique, and the surgeon must anticipate the next step that may be necessary. Generally, the method chosen should allow for the potential use of as many other methods as possible.
Operations for nonunions are relatively extensive and should be recommended only after nonunion has been shown clinically and radiographically, and when union is improbable or obviously impossible without a change in treatment.
CLASSIFICATION OF NONUNIONS
In general, the treatment of nonunions increases in complexity as the components of the nonunion (infection, deformity, shortening, bony defect) increase. The increasing severity of nonunions outlined in the classification systems of Judet and Judet; Müller, Weber, and Cech; and Paley et al. dictate more extensive surgical methods.
Weber and Cech Classification (Biological Viability)
Weber and Cech classified nonunions based on the biological vitality and vascularity of the fracture ends. This system fundamentally dictates whether the nonunion requires mechanical stabilization alone or a combination of biological augmentation and stabilization.
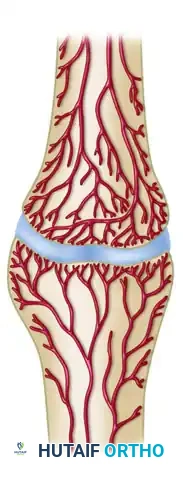
1. Hypervascular (Hypertrophic) Nonunions
These nonunions possess excellent biological healing potential but lack adequate mechanical stability. They are highly vascularized and capable of biological reaction.
-
"Elephant Foot" Nonunions: Characterized by abundant, hypertrophic callus formation. They typically occur after premature weight-bearing or in the presence of unstable fixation.
-
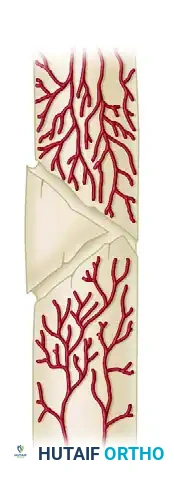
"Horse Hoof" Nonunions: Exhibit mild hypertrophic callus, often occurring after moderately unstable fixation with plates and screws. The ends of the fragments show some callus, insufficient for union, and possibly a little sclerosis.

-
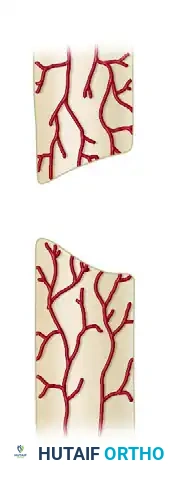
Oligotrophic Nonunions: These are not hypertrophic but are vascular, and callus is absent. They typically occur after major displacement of a fracture, severe distraction of the fragments, or internal fixation without accurate apposition of the fragments.

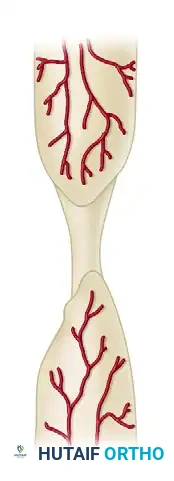
2. Avascular (Atrophic) Nonunions
Avascular or inert nonunions are incapable of biological reaction. Studies of strontium-85 uptake in these nonunions indicate a poor blood supply in the ends of the fragments. They require both biological augmentation (decortication, bone grafting) and rigid mechanical stability.
-
Torsion Wedge Nonunions: Characterized by the presence of an intermediate fragment in which the blood supply is decreased or absent. The intermediate fragment has healed to one main fragment but not to the other. These typically are seen in tibial fractures treated by plate and screws.

-
Comminuted Nonunions: Characterized by the presence of one or more necrotic intermediate fragments.
-
Defect Nonunions: Characterized by a significant gap between the fracture ends, often due to severe trauma, bone loss, or surgical debridement of infected bone.
-
Atrophic Nonunions: The end stage of avascular nonunions, where the bone ends are osteoporotic, resorbed, and completely lack osteogenic potential.
Paley Classification (Bone Loss and Deformity)
According to the classification of Paley et al., nonunions are categorized based on the presence of bone loss, mobility, and deformity. This system is particularly useful when planning treatment with circular external fixation (Ilizarov).
Type A Nonunions (< 1 cm of bone loss)
Most Type A nonunions can be treated with restoration of alignment, followed by compression.
* Type A1: Lax (mobile) nonunion.

* Type A2-1: Stiff (nonmobile) nonunion without deformity.

* Type A2-2: Stiff (nonmobile) nonunion with a fixed deformity.

Type B Nonunions (> 1 cm of bone loss)
Type B nonunions may require additional cortical osteotomy and either internal bone transport or overall lengthening to obtain the original bone length.
* Type B1: Bony defect present, but no shortening.

* Type B2: Shortening present, but no bony defect (ends are in contact).
* Type B3: Both bony defect and shortening are present.

PREOPERATIVE EVALUATION AND OPTIMIZATION
The requirements common to all successful techniques are biomechanical stability and biological vitality of the bone. These can be obtained through good reduction, sufficient bone grafting, and firm stabilization of the fragments. Many techniques or combinations of techniques meet these requirements, and some general guidelines apply to all techniques.
Before any surgical intervention, the host biology must be optimized. The "Diamond Concept" of fracture healing dictates that successful union requires osteogenic cells, an osteoconductive scaffold, osteoinductive growth factors, and a mechanically stable environment, all supported by adequate vascularity.
- Metabolic Optimization: Evaluate Vitamin D levels, parathyroid hormone (PTH), thyroid function, and nutritional markers (albumin, prealbumin). Correct any deficiencies.
- Infection Rule-Out: Occult infection is a leading cause of nonunion. Obtain Erythrocyte Sedimentation Rate (ESR), C-Reactive Protein (CRP), and a complete blood count (CBC). If inflammatory markers are elevated, preoperative aspiration or intraoperative tissue cultures (minimum of 5 samples) are mandatory.
- Smoking Cessation: Nicotine is a potent vasoconstrictor that severely impairs osteogenesis. Strict smoking cessation must be enforced, ideally confirmed via cotinine testing prior to elective nonunion surgery.
SURGICAL PRINCIPLES AND TECHNIQUES
Reduction of Fragments
When the fragments are in good position but are separated by fibrous tissue, extensive dissection usually is undesirable. Leaving the periosteum, callus, and fibrous tissue intact around the major fragments preserves their vascularity and stability. Using a bridging graft, the intervening fibrous tissue and callus ossify, resulting in union of the fracture.
Displaced, and especially bayonet, nonunions of any long bone can be approximately reduced by gradual traction using a simple pin fixator before closed intramedullary nailing. In cooperative patients, posttraumatic shortening usually can be corrected rapidly.
Surgical Warning: Acute correction of severe shortening (>3 cm) intraoperatively can lead to neurovascular traction injuries. Gradual restoration is preferred.
The external fixator is applied for a few days to restore length, the fixator is removed, and closed intramedullary nailing is performed. We have had no problems with infections after a brief period of external fixation. Alternatively, an Ilizarov frame can be used to restore length, appose fragments, and stabilize the fragments until union.
Plating and bone grafting of displaced nonunions of most long bones require a more extensive operation. Scar tissue around the nonunion must be excised so that the grafts can be covered by relatively normal tissue. The fragments are mobilized, preserving their normal soft tissue attachments as much as possible; their rounded ends are resected so that contact is maximal; their medullary canals are cleared of fibrous tissue to aid in medullary osteogenesis (recanalization); and they are apposed as closely as possible.
Bone Grafting and Orthobiologics
For many years, the most frequently used method of treatment of nonunions has been bone grafting. Numerous techniques have been described. Autogenous bone graft, allograft bone, or synthetic bone substitutes, used alone or in conjunction with internal fixation, may help to stimulate bone formation.
Autogenous Bone Graft
Autogenous cancellous bone, although limited in quantity and associated with significant donor site morbidity, remains the “gold standard” in grafting material. Its osteoconductive (matrix) and osteoinductive (protein) properties and its osteoprogenitor cells make it an ideal substance for nonstructural grafting. Cancellous autogenous grafts are obtained from the proximal tibia, distal radius, and ilium.
Additionally, reaming of long bones using a Reamer-Irrigator-Aspirator (RIA) (Synthes, Paoli, PA) can provide a massive volume of highly osteogenic autologous bone graft material from the femoral or tibial canal, significantly reducing the need for iliac crest harvest.
Allograft Bone
Allogenic bone for grafting can be used when the source of fresh autogenous bone is inadequate or inaccessible. Clinical and experimental data show, however, that the osteogenic properties of allogenic bone are inferior to the osteogenic properties of fresh autogenous bone. If mixed with autogenous bone or host bone marrow, cancellous allograft can be used in nonstructural applications with excellent results to increase the volume of bone graft available.
For structural applications, autologous cortical grafts, except from the fibula, are now rarely used because of donor site morbidity. Frozen or freeze-dried cortical allografts provide the greatest structural strength, but their osteogenic properties are limited. Good results, however, have been reported with a composite allograft cortical strut consisting of allogenic cortical bone combined with human bone morphogenetic protein (BMP) in the treatment of femoral nonunions. Newer techniques, such as nonirradiated terminal sterilization and genetic screening, have made allogenic grafts stronger and safer.
Synthetic Bone Substitutes and Ceramics
Ceramics (hydroxyapatite, tricalcium phosphate, or some combination of the two) have osteoconductive properties and avoid problems with donor site morbidity but are extremely brittle, and the results of their use at our institution have been disappointing when used in isolation. Combining ceramics with bone morphogenetic protein (BMP-2 or BMP-7) or other osteoinductive proteins is highly helpful. Particulate ceramic also can be mixed with bone marrow aspirate concentrate (BMAC) to add osteoprogenitor cells or with a limited volume of cancellous autograft to improve its osteoinductive capability.
Free vascularized bone grafts (e.g., free vascularized fibular graft) have been used successfully for bridging long defects (>6 cm) in nonunions, providing immediate structural support and biological viability.
Historical Context: Onlay Bone Grafts
Massive cortical grafts combine fixation and osteogenesis in treating nonunions of the long bones. In the past, the onlay graft and the massive sliding graft were most frequently used. The massive sliding graft was described by Gill. Campbell originated the term onlay graft, but his technique is a modification of Henderson’s technique. The onlay bone graft was used for nonunions of the shaft of any long bone, and the technique was similar for all; only the size of the graft and the number of screws were modified to suit the individual bones.
Phemister, almost 100 years ago, described a technique of onlay bone grafting for established nonunions in which the graft is placed subperiosteally across the fragments without mobilizing the fragments. Besides being simple to do, its advantages were that the blood supply of the fragments and the normal impacting forces of the fracture were not disturbed.
Although these techniques were useful for delayed unions and nonunions of long bones historically, they are now rarely, if ever, used due to the advent of modern locking plates and intramedullary nails.
STEP-BY-STEP SURGICAL APPROACHES
1. Management of Hypertrophic Nonunions
The primary issue in hypertrophic nonunions is instability. The biological environment is already primed for healing.
* Step 1: Expose the nonunion site minimally to preserve the highly vascularized callus.
* Step 2: Remove the failed hardware (if present).
* Step 3: Apply rigid mechanical compression. This can be achieved via exchange nailing (reaming the canal 1-2 mm larger and inserting a larger diameter nail) or by applying a dynamic compression plate (DCP) or locking compression plate (LCP) with an articulated tension device.
* Step 4: Bone grafting is generally not required for hypertrophic nonunions, as the mechanical stabilization alone will allow the existing callus to consolidate.
2. Management of Atrophic Nonunions
Atrophic nonunions require a complete biological overhaul combined with rigid fixation.
* Step 1: Perform a generous surgical approach. Excise all avascular, sclerotic bone ends until punctate bleeding (the "paprika sign") is observed.
* Step 2: Open the medullary canals on both sides of the nonunion (recanalization) using drill bits or curettes to allow marrow elements to reach the fracture site.
* Step 3: Perform osteoperiosteal decortication (Judet technique) by elevating thin shims of cortical bone with attached periosteum to create a vascularized biological envelope.
* Step 4: Pack the defect with high-quality autogenous cancellous bone graft (e.g., RIA or iliac crest).
* Step 5: Apply absolute rigid internal fixation, typically utilizing a locking plate construct spanning the defect.
3. Management of Defect Nonunions (Bone Loss)
For defects greater than 2-3 cm, simple grafting is insufficient.
* Option A (Masquelet Technique): A two-stage procedure. Stage 1 involves radical debridement, placement of a PMMA cement spacer, and rigid fixation. After 6-8 weeks, an induced pseudo-synovial membrane forms. Stage 2 involves removing the spacer and packing the membrane-lined void with autograft/allograft mix.
* Option B (Bone Transport): Utilizing an Ilizarov circular frame, a corticotomy is performed in the healthy metaphyseal bone. The bone segment is gradually transported across the defect (distraction osteogenesis) at a rate of 1 mm per day until it docks with the opposing fragment.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
Postoperative management must be tailored to the specific bone, the type of fixation achieved, and the biological quality of the reconstruction.
- Weight-Bearing: For diaphyseal nonunions treated with exchange intramedullary nailing, immediate weight-bearing as tolerated is often encouraged to promote micromotion and secondary bone healing. For plate fixations, particularly in atrophic nonunions with structural grafting, strict non-weight-bearing or touch-down weight-bearing is maintained for 6 to 12 weeks until radiographic evidence of graft incorporation is visible.
- Range of Motion: Early active and passive range of motion of adjacent joints is critical to prevent stiffness and promote local blood flow. Modern rigid fixation allows for this without compromising the nonunion site.
- Pharmacologic Adjuncts: Non-steroidal anti-inflammatory drugs (NSAIDs) should be strictly avoided, as they inhibit prostaglandin synthesis necessary for bone healing. Deep vein thrombosis (DVT) prophylaxis should be administered per institutional protocols.
- Monitoring: Serial radiographs should be obtained at 4, 8, and 12 weeks postoperatively to assess callus formation, graft incorporation, and hardware integrity. If healing is sluggish, the addition of LIPUS or electrical bone stimulation may be considered as an adjunct.
📚 Medical References
- with pulsed electromagnetic fi elds, Clin Orthop Relat Res 161:58, 1981.
- Heppenstall RB: The present role of bone graft surgery in treating nonunion, Orthop Clin North Am 15:113, 1984.
- Jacobs RR, Luethi U, Dueland RT, et al: Electrical stimulation of experimental nonunions, Clin Orthop Relat Res 161:146, 1981.
- Johannes EJ, Kaulesar Sukul DM, Matura E: High-energy shock waves for the treatment of nonunions: an experiment on dogs, J Surg Res 57:246, 1994.
- Johnson EE, Urist MR, Finerman GAM: Bone morphogenetic protein augmentation grafting of resistant femoral nonunions, Clin Orthop Relat Res 230:256, 1988.
- Johnson EE, Urist MR, Finerman GAM: Repair of segmental defects of the tibia with cancellous bone grafts augmented with human bone morphogenetic protein, Clin Orthop Relat Res 236:249, 1988.
- Johnson EE, Urist MR, Finerman GAM: Distal metaphyseal tibial nonunion, Clin Orthop Relat Res 250:234, 1990.
- Johnson EE, Urist MR, Finerman GA: Resistant nonunions and partial or complete segmental defects of long bones: treatment with implants of a composite of human bone morphogenetic protein (BMP) and autolyzed, antigen-extracted, allogeneic (AAA) bone, Clin Orthop Relat Res 277:229, 1992.
- Jones CB, Mayo KA: Nonunion treatment: iliac crest bone graft techniques, J Orthop Trauma 19(10 suppl):S11, 2005.
- Judet J, Judet R: L’ostéogénèse et les retards de consolidation et les pseudarthroses des os longs, Huitième Congrès SICOT, 1960, p 315. Kawamura M, Urist MR: Induction of callus formation by implants of bone morphogenetic protein and associated bone matrix noncollagenous proteins, Clin Orthop Relat Res 236:240, 1988.
- Kirchner PT, Simon MA: Current concepts review: radioisotopic evaluation of skeletal disease, J Bone Joint Surg 63A:673, 1981.
- Kummer FJ, Meislin RJ, Pankovich A, et al: Closed treatment of canine nonunions by controlled compression and distraction using an Ilizarov fi xator: a preliminary study, Orthopedics 13:1379, 1990.
- Kwiatkowski TC, Hanley EN, Ramp WK: Cigarette smoking and its orthopaedic consequences, Am J Orthop 9:590, 1996.
- Kyro A, Usenius JP, Aarnio M, et al: Are smokers a risk group for delayed healing of
You Might Also Like
