Surgical Management of Foot Deformities in Cerebral Palsy
Key Takeaway
Foot deformities, particularly ankle equinus, affect up to 90% of patients with cerebral palsy. Driven by spasticity and muscle imbalance, these deformities severely compromise ambulation. Surgical management, including Achilles tendon lengthening and gastrocnemius-soleus recession, is indicated when conservative measures fail. This guide details the biomechanics, indications, and step-by-step operative techniques required to restore plantigrade alignment and optimize gait kinematics in the spastic foot.
Pathophysiology and Biomechanics of the Spastic Foot
Foot deformities driven by altered, abnormal, or asymmetric muscle forces are ubiquitous in patients with cerebral palsy (CP), affecting approximately 70% to 90% of this pediatric population. The most frequently encountered deformity is ankle equinus, with equinovarus and equinovalgus deformities presenting with near-equal frequency depending on the anatomic distribution of neurologic involvement.
In a landmark series of 306 children with cerebral palsy, Ruda and Frost demonstrated that approximately 50% of patients maintained normal “side-to-side” coronal plane balance, while 25% developed valgus deformities and 23% developed varus deformities. The presence of a foot deformity exerts a profound effect on the patient’s overall ambulatory capacity and energy expenditure. O’Connell et al. established that in diplegic patients, the presence of a bilateral foot deformity—regardless of its specific morphological type—had a statistically significant deleterious effect on the overall level of ambulation compared to unilateral involvement.
A patient’s deformity is rarely static; it evolves dynamically over time, particularly during periods of rapid skeletal growth. For example, in a very young child presenting with a flexible valgus foot deformity, the persistence of tonic reflexes and unremitting abnormal muscle forces may progressively invert the biomechanical axis, ultimately causing a rigid varus foot position to develop. Furthermore, spasticity of the intrinsic musculature of the foot can precipitate secondary forefoot and midfoot deformities, including hallux valgus, claw toes, and forefoot adduction. While these can occur in isolation, they are most frequently associated with primary deformities related to abnormal extrinsic foot musculature.
Equinus Deformity: Clinical Evaluation and Decision Making
Equinus deformity remains the hallmark foot deformity in cerebral palsy, affecting up to 70% of children. Basset and Baker reported that approximately 25% of all patients with CP develop an equinus contracture severe enough to necessitate operative intervention.
Etiology and Progression
The deformity is primarily driven by spasticity of the gastrocnemius-soleus complex. This dynamic contracture often exacerbates during periods of rapid physiological growth due to the longitudinal overgrowth of the tibia relative to the spastic, non-compliant gastrocnemius-soleus muscle-tendon unit. Animal models have corroborated this clinical observation, demonstrating that muscles in mice with hereditary spasticity grow at a significantly slower rate than normal, healthy muscle tissue.
Non-Operative Management
Conservative management remains the first-line treatment and serves as a critical means of delaying operative intervention until the child is older, thereby reducing the risk of recurrence. Modalities include:
* Aggressive Physical Therapy: Focused on passive stretching. Tardieu and Tardieu demonstrated that soleus stretching for a minimum of 6 hours a day is required to prevent contractures from developing—a threshold often difficult to achieve clinically.
* Orthotic Management: Ankle-foot orthoses (AFOs), particularly rigid night splints, are essential to maintain the foot in a neutral position and counteract nocturnal spasticity.
* Serial Casting and Chemodenervation: Botulinum toxin type A (Botox) injections combined with serial short-leg casting can provide temporary relief of dynamic spasticity and improve muscle length.

Indications for Surgery
The exact indications for surgical intervention remain nuanced given the highly variable phenotypic expression of cerebral palsy. However, consensus indications include:
1. Ambulatory Children: Inability to achieve a neutral ankle position (0 degrees of dorsiflexion) with the knee extended during the stance phase of gait, leading to toe-walking, knee hyperextension (genu recurvatum), or early heel rise.
2. Non-Ambulatory Children: Severe contractures that preclude proper shoe wear, interfere with standing frame programs, or cause skin breakdown and hygiene difficulties.
⚠️ Surgical Warning: The Risk of Overlengthening
Overlengthening of the gastrocnemius-soleus complex must be strictly avoided, particularly in the ambulatory child. Excessive lengthening destroys the plantarflexion-knee extension couple, leading to profound push-off weakness and the development of a debilitating iatrogenic crouch gait. Once established, crouch gait is biomechanically disastrous, leading to rapid quadriceps exhaustion and loss of independent ambulation.
Surgical Correction of Equinus Deformity
Due to the heterogeneous nature of CP and the myriad of procedures utilized, comparing success rates across the literature is challenging. Recurrence rates range from 0% to 50%, heavily dependent on the patient's age at the time of surgery, anatomic involvement (hemiplegia vs. diplegia), and length of follow-up.
Rattey et al. reviewed 57 patients undergoing 77 open heel cord lengthenings. At a 10-year follow-up, 50% of children aged 3 years or younger at the time of surgery experienced a recurrence, compared to zero recurrences in children who were at least 6 years old. Furthermore, hemiplegic patients demonstrated a higher propensity for recurrence than diplegic patients.
The gastrocnemius-soleus complex can be lengthened at two primary levels:
1. Musculotendinous Junction: Via an aponeurotic recession (e.g., Strayer, Vulpius, Baker). Preferred in ambulatory children due to a significantly lower risk of overlengthening.
2. Achilles Tendon Level: Via open or percutaneous lengthening. Reserved for severe, rigid deformities unresponsive to recession, or for non-ambulatory patients.
Open Lengthening of the Achilles Tendon
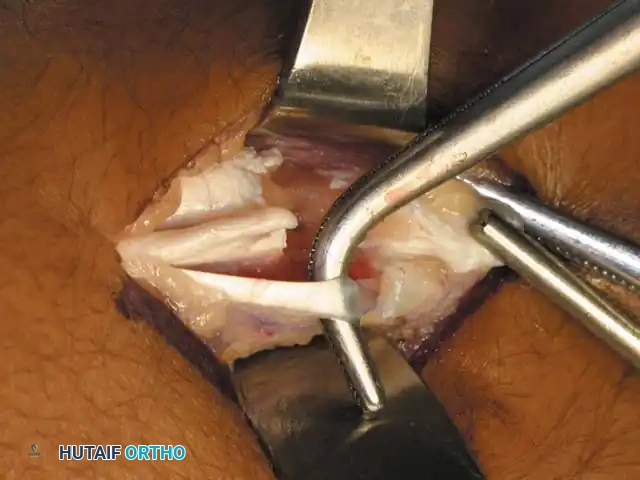
🔪 Surgical Technique 30-11: White Modification
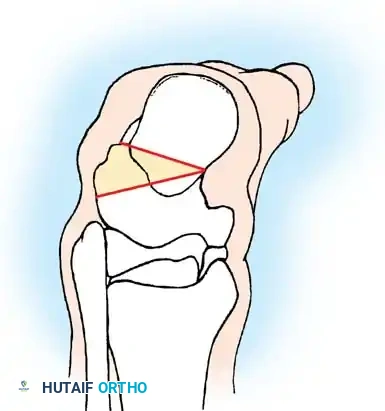
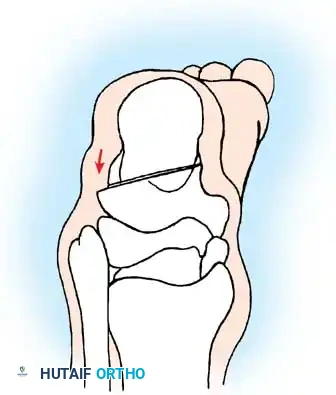
The White modification of the Achilles tendon lengthening utilizes a sliding technique that relies on the natural rotation of the Achilles tendon fibers (which rotate approximately 90 degrees from proximal to distal).
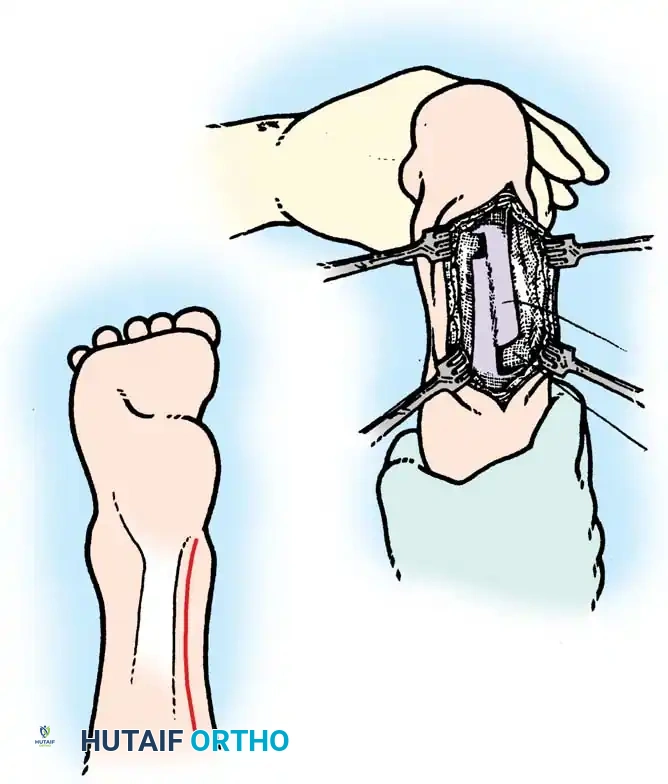
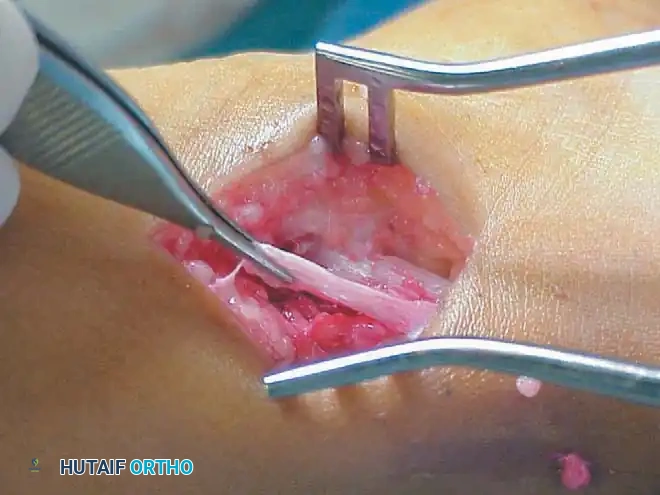
Fig. 30-29 Sliding lengthening of Achilles tendon. A, Posteromedial incision. B, Two cuts are made through one half of the tendon in opposite directions. As the foot is placed in dorsiflexion, tendon fibers separate and slide.
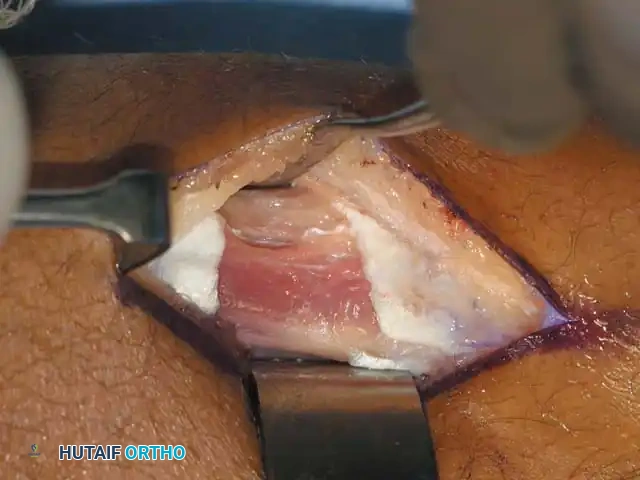
- Positioning and Incision: Place the patient prone or supine with the leg externally rotated. Utilize a 5 to 7 cm posteromedial longitudinal incision to expose the Achilles tendon from its calcaneal insertion to approximately 10 cm proximally.
- Sheath Preservation: Carefully incise the paratenon longitudinally. Preserving the sheath is critical to prevent postoperative adhesions and preserve the mesotenon blood supply.
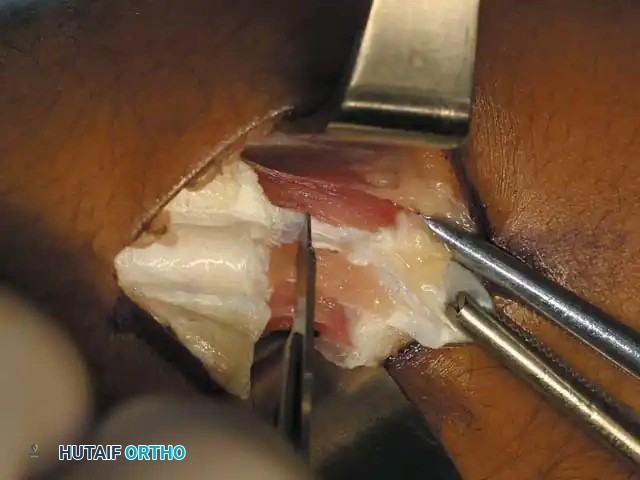
- Distal Tenotomy: Divide the posteromedial two-thirds of the tendon transversely, approximately 1 to 2 cm proximal to its insertion on the calcaneus.
- Proximal Tenotomy: Apply a moderate, sustained dorsiflexion force to the foot. Divide the anteromedial (or medial) two-thirds of the tendon approximately 5 to 8 cm proximal to the site of the distal division.
- Sliding Lengthening: Forcefully dorsiflex the foot to neutral or a maximum of 5 degrees of dorsiflexion. The tendon fibers will slide upon themselves, lengthening to the desired position.
- Closure: While side-to-side suturing with absorbable suture can be performed, it is biomechanically unnecessary in a true sliding technique. However, many surgeons prefer to place a few stabilizing sutures. Meticulously close the paratenon and subcutaneous tissues to prevent skin adherence.

Postoperative Protocol (White Modification)
The patient is placed in a short leg cast with the ankle in the corrected position (neutral to slight dorsiflexion) and is allowed to bear full weight postoperatively. The cast is maintained for 4 weeks. During this period, active knee extension is heavily encouraged to maintain the relative lengthening of the gastrocnemius-soleus complex. Following cast removal, a custom-molded solid Ankle-Foot Orthosis (AFO) is fitted.
Z-Plasty Lengthening of the Achilles Tendon
Z-plasty provides precise, measured control over the amount of lengthening achieved, making it highly reliable for severe, rigid contractures. However, Rattey et al. reported recurrence rates of 18% in diplegic and 41% in hemiplegic patients at 10 years following open Z-plasty, strongly correlated with surgery performed before age 4.
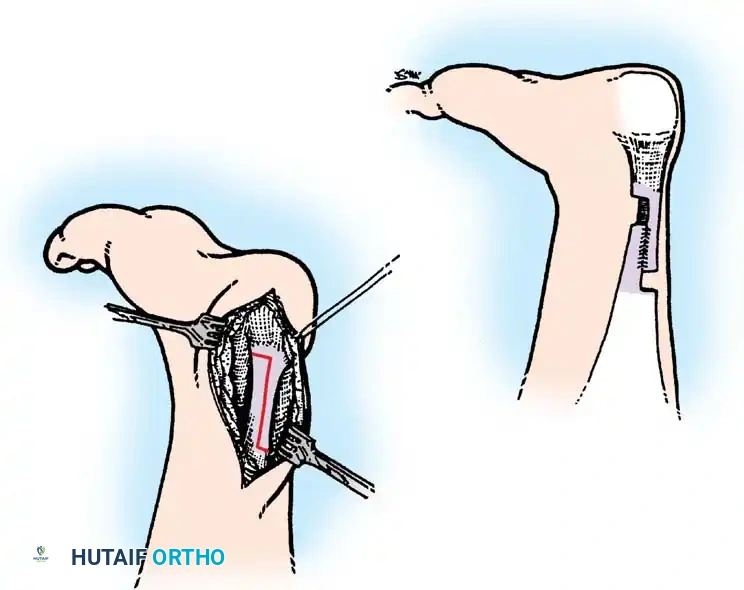
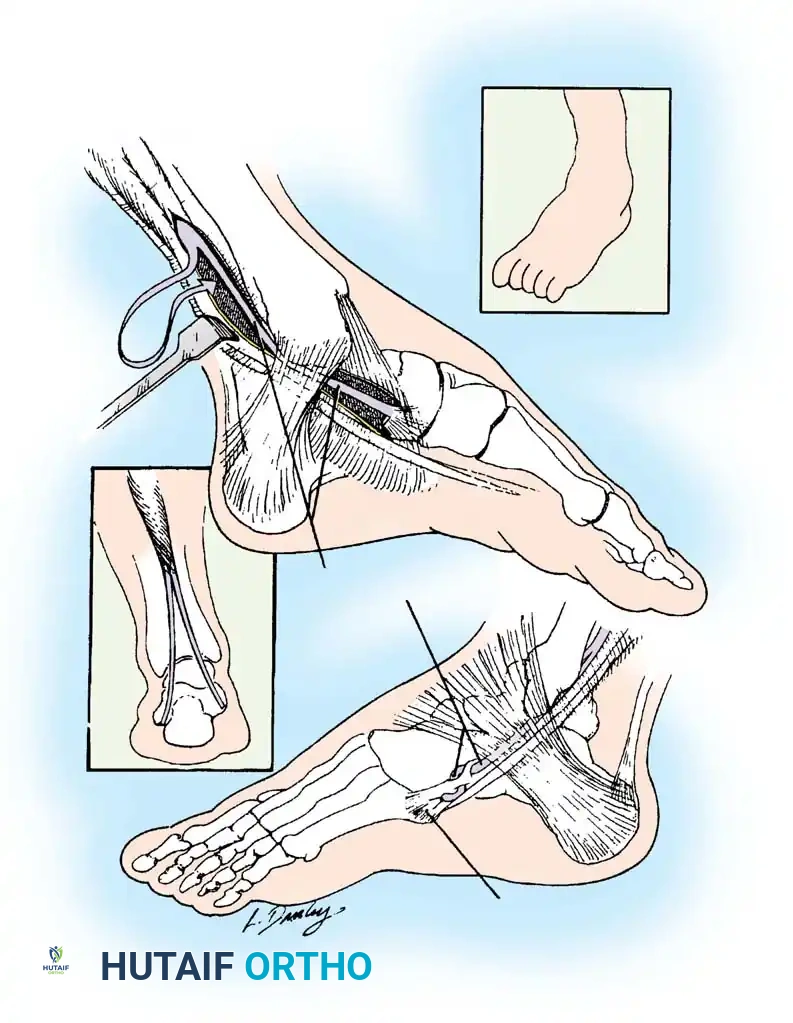
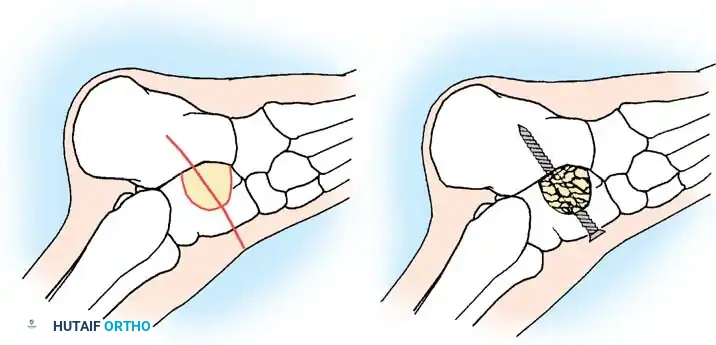
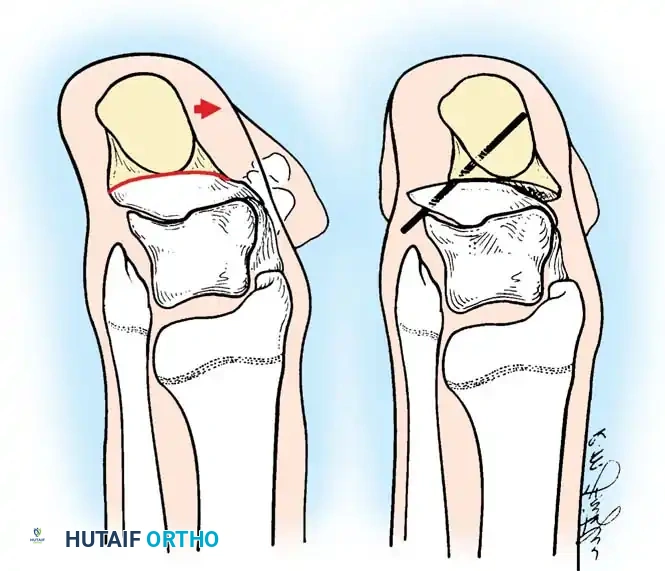
Fig. 30-30 Z-plasty lengthening of Achilles tendon. A, Longitudinal incision. B, Ends are sutured to repair the tendon after controlled lengthening.
🔪 Surgical Technique 30-12: Open Z-Plasty
- Incision: Make a posteromedial incision midway between the Achilles tendon and the posterior aspect of the medial malleolus, beginning at the superior border of the calcaneus and extending cephalad for 4 to 5 cm.
- Exposure: Deepen the dissection sharply through the subcutaneous tissue. Identify and protect the sural nerve laterally. Incise the paratenon longitudinally and free the tendon circumferentially.
- Longitudinal Split: Make a precise longitudinal incision in the exact center of the Achilles tendon, extending from proximal to distal over a length of 4 to 6 cm.
- Distal Hemisection: Turn the scalpel 90 degrees distally.
- Clinical Pearl: Make the distal cut toward the medial side for a varus deformity (to weaken the medial inverting force) and toward the lateral side for a valgus deformity.
- Proximal Hemisection: Hold the cut portion with forceps. Bring the scalpel to the proximal extent of the longitudinal split, turn it in the opposite direction of the distal cut, and divide the remaining half of the tendon transversely.
- Plantaris Release: Identify the plantaris tendon on the medial aspect of the Achilles and divide it transversely.
- Tensioning and Repair: Evaluate the passive excursion of the triceps surae. Pull the proximal stump distally to its maximal stretched length using a Kocher clamp. Allow the tendon to retract exactly halfway back to its resting length. Suture the proximal and distal stumps at this precise overlap using heavy absorbable sutures (e.g., #1 Vicryl) in a side-to-side or figure-of-eight fashion.
- Positional Adjustment: Fine-tune the tension based on spasticity severity: neutral for mild spasticity, 10 degrees of dorsiflexion for moderate involvement, and up to 20 degrees for severe, rigid deformities.



Postoperative Protocol (Z-Plasty)
Apply a long leg or short leg cast depending on concomitant procedures. Ambulation is permitted as soon as pain subsides (typically 5 to 10 days). Cast immobilization is maintained for a total of 6 weeks. Post-casting bracing is mandatory. If the anterior tibialis muscle lacks volitional control, full-time AFO bracing is required to prevent foot drop and recurrent equinus.
Percutaneous Lengthening of the Achilles Tendon
Percutaneous lengthening (often referred to as the Hoke technique) is a rapid, minimally invasive, and highly effective outpatient procedure. Moreau and Lake reported that 97% of 90 treated limbs showed significant improvement in gait function with minimal complications.
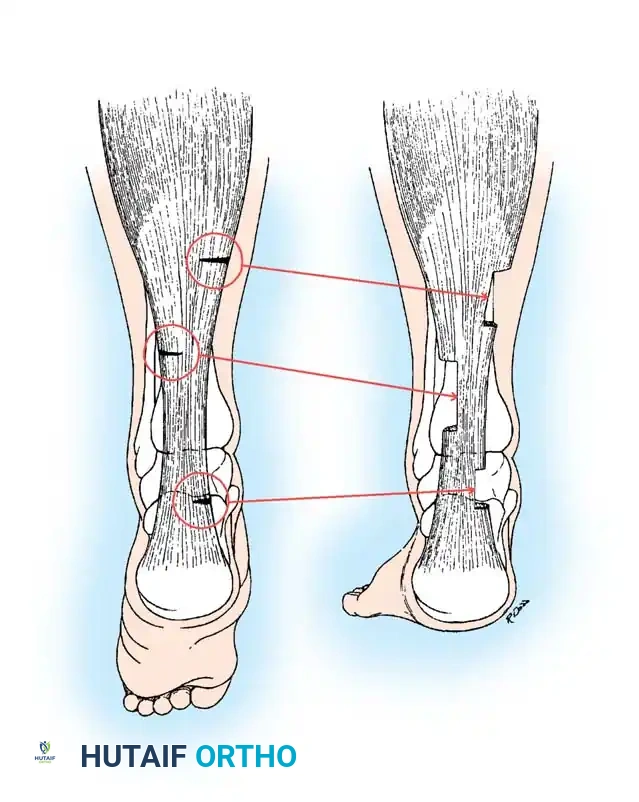
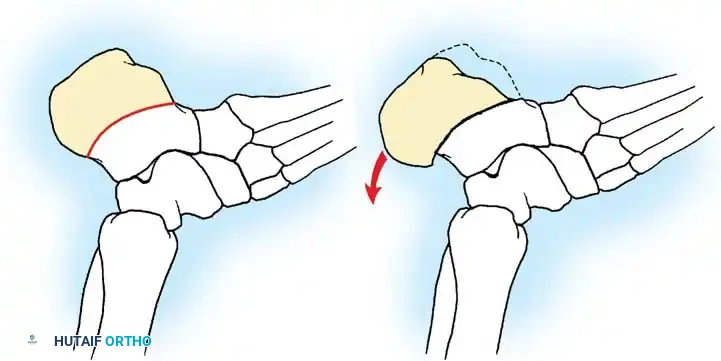
Fig. 30-31 Incisions for percutaneous Achilles tendon lengthening. Cut ends slide on themselves with forceful dorsiflexion of the foot.
🔪 Surgical Technique 30-13: Percutaneous Approach
- Positioning: Place the patient prone. Extend the knee and forcefully dorsiflex the ankle to place the Achilles tendon under maximal tension. This makes the tendon prominent, subcutaneous, and safely displaces the anterior neurovascular bundle.
- Triple Hemisection (Tenotomies): Utilize a #11 blade to make three distinct partial tenotomies through stab incisions:
- Distal Cut: Placed just proximal to the calcaneal insertion, cutting through exactly half the width of the tendon.
- Proximal Cut: Placed medially, just distal to the musculotendinous junction, cutting through half the width.
- Middle Cut: Placed laterally, exactly midway between the proximal and distal cuts, cutting through the lateral half of the tendon.
- Deformity Specificity: Place the two ipsilateral incisions on the medial side if the heel is in varus, and on the lateral side if the heel is in valgus.
- Correction: Forcefully dorsiflex the ankle. A palpable and audible "pop" will occur as the tendon fibers slide and yield to the desired angle of dorsiflexion.
- Wound Care: No sutures are required. Apply sterile steri-strips and a short or long leg cast with the knee in full extension.
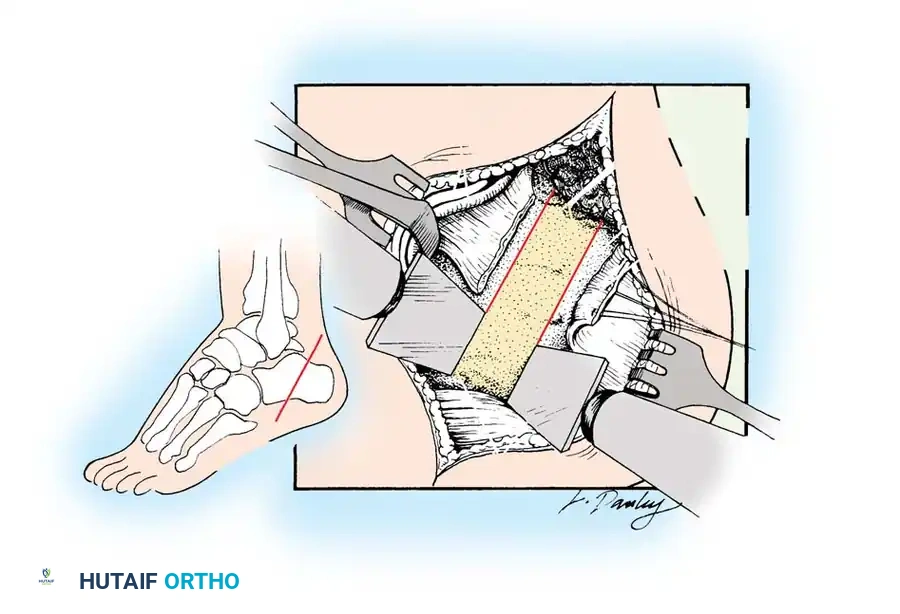
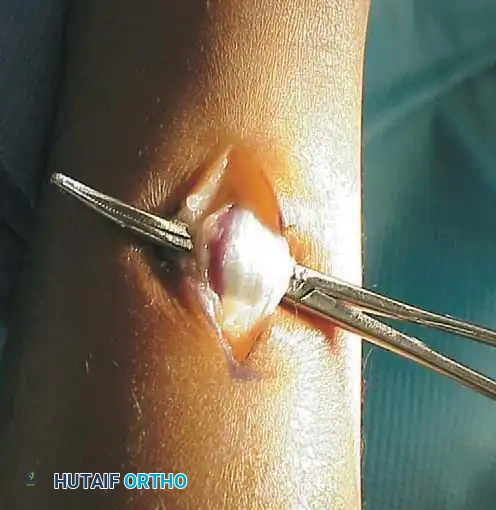
Lengthening of the Gastrocnemius-Soleus Muscle (Aponeurotic Recession)
When the Silfverskiöld test indicates isolated gastrocnemius contracture (equinus corrects with knee flexion but is present with knee extension), or when attempting to minimize the risk of overlengthening in an ambulatory child, an aponeurotic recession is the procedure of choice.
Historical Context and Techniques
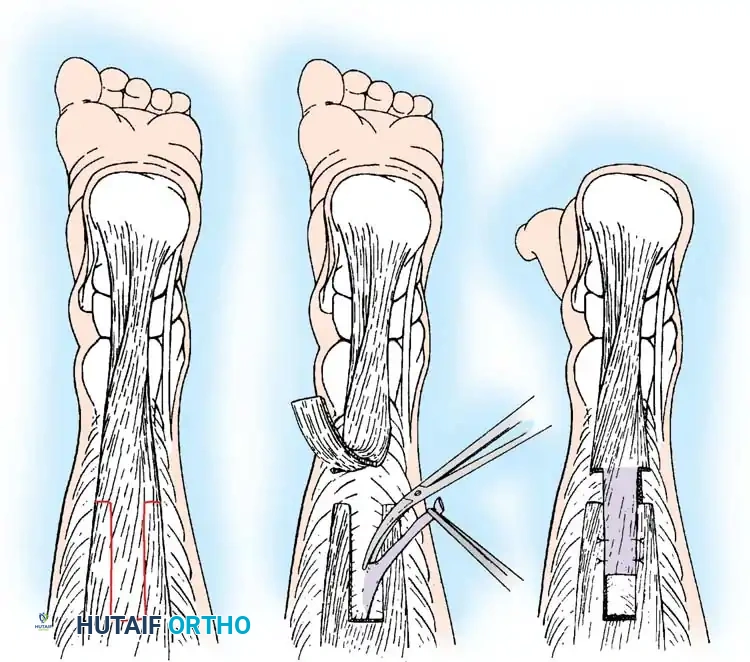
- Strayer Procedure (1950): The aponeurotic tendon of the gastrocnemius is divided transversely near its junction with the soleus. The ankle is dorsiflexed, and the retracted proximal tendon is sutured to the underlying soleus fascia. Strayer postulated this altered proprioceptive feedback, inhibiting abnormal stretch reflexes.
- Vulpius Procedure: The gastrocnemius aponeurosis is divided (often in a V-shape) and allowed to retract distally without being sutured to the soleus.
- Baker Procedure: Utilizes a “tongue-in-groove” (U-shaped) modification of the Vulpius operation, allowing for controlled sliding and suturing.
Clinical Outcomes
Basset and Baker compared neurectomy, proximal gastrocnemius recession, and the Baker aponeurotic lengthening. The aponeurotic lengthening yielded dramatically superior results, with a recurrence rate of only 4%. Craig and van Vuren demonstrated radiographically that a Strayer-type recession provides the greatest degree of equinus correction because the soleus origin extends distally to the mid-tibia, tethering the gastrocnemius and limiting excursion if not properly released.
💡 Clinical Pearl: Neurectomy
Historically, partial neurectomy of the tibial nerve branches to the gastrocnemius was performed to reduce spasticity. This is no longer indicated in modern orthopedic practice. Spasticity is better managed via targeted aponeurotic lengthening, Botox, or selective dorsal rhizotomy (SDR).
Postoperative Protocol (Gastrocnemius Recession)
Patients are immobilized in a short leg cast for 4 weeks and permitted weight-bearing as tolerated. Strict adherence to knee extension bracing or casting is encouraged to maximize the stretch on the gastrocnemius. Following cast removal, aggressive physical therapy is initiated to maintain dorsiflexion, and patients are transitioned to a solid AFO for nighttime use for a minimum of 6 months.

Management of Varus and Valgus Deformities
While equinus is the primary sagittal plane deformity, coronal plane malalignment (varus or valgus) frequently coexists and complicates management. The direction of the deformity is dictated by the specific subtype of cerebral palsy and the resultant vector of spastic muscle imbalance.
In a comprehensive biomechanical study of 230 children, Bennett et al. established that in hemiplegic CP, the foot deformity is almost exclusively equinus or equinovarus (driven by a spastic posterior tibialis and anterior tibialis). Conversely, in diplegic and quadriplegic CP, valgus deformities predominate (64%), driven by spastic peroneals and a contracted Achilles tendon acting as an evertor due to lateral displacement of the calcaneal axis.
Surgical Principles for Coronal Deformities
Although statistically less common than valgus, varus deformities are significantly more functionally disabling. They create a rigid, unstable lateral border weight-bearing pattern that is highly recalcitrant to orthotic management. Consequently, operative intervention is pursued more aggressively.
Surgical correction of varus/valgus deformities must address both the dynamic muscle imbalance and any fixed bony deformity:
1. Dynamic Deformity: Managed via tendon transfers or lengthenings. For varus, a Split Anterior Tibial Tendon Transfer (SPLATT) or posterior tibialis lengthening/transfer is highly effective.
2. Fixed Bony Deformity: Requires osseous intervention. Calcaneal sliding osteotomies (e.g., medial displacement for valgus, lateral displacement for varus) or lateral column lengthening (Evans osteotomy) are utilized to restore a plantigrade, braceable foot.

.
