Unraveling Foot & Ankle Lumps: Is it Clear Cell Sarcoma?
Introduction & Epidemiology
Clear Cell Sarcoma (CCS), also known historically as malignant melanoma of soft parts, is a rare but aggressive soft tissue sarcoma. It accounts for less than 1% of all soft tissue sarcomas. Despite its histological resemblance to melanoma, its behavior and genetic signature are distinct. CCS is characterized by a specific recurrent chromosomal translocation, t(12;22)(q13;q12), resulting in the EWSR1-ATF1 fusion gene, which is critical for its diagnosis and pathogenesis.
The foot and ankle region represents a common primary site for CCS, accounting for approximately 40-60% of cases, often with a predilection for tendons, aponeuroses, and deep fascia. This anatomical preference, coupled with its often indolent clinical presentation as a slowly growing, painless mass, frequently leads to delayed diagnosis. Misdiagnosis as a benign entity such as a ganglion cyst, fibroma, or tenosynovitis is common, underscoring the importance of vigilance in evaluating any persistent soft tissue mass in this region, particularly in younger adults.
Epidemiologically, CCS typically affects adolescents and young adults, with a median age at diagnosis in the third decade of life. There is a slight female predilection reported in some series. Despite aggressive local therapy, CCS has a high propensity for local recurrence and distant metastasis, primarily to regional lymph nodes, lung, bone, and brain. The metastatic rate can exceed 50% within five years, contributing to its poor prognosis. The median survival typically ranges from 2-5 years post-diagnosis, making early, accurate diagnosis and aggressive management paramount.
Surgical Anatomy & Biomechanics
The intricate anatomy of the foot and ankle presents unique challenges in the surgical management of CCS. This region is characterized by a dense conglomeration of vital structures within confined fascial compartments:
*
Neurovascular Bundles:
The proximity of major arteries (anterior and posterior tibial, dorsalis pedis, peroneal) and their associated nerves (deep and superficial peroneal, tibial, sural, saphenous) demands meticulous dissection and often necessitates sacrifice of non-essential structures to achieve adequate oncologic margins.
*
Tendons and Aponeuroses:
CCS frequently arises within or in close association with tendons (e.g., Achilles, tibialis posterior, peroneals, extensors, flexors) and the plantar aponeurosis. These structures are crucial for foot mechanics, gait, and stability. Resection of affected tendons requires complex reconstruction or stabilization procedures to preserve function.
*
Articular Structures:
The numerous joints of the foot and ankle (tibiotalar, subtalar, midtarsal, tarsometatarsal, metatarsophalangeal, interphalangeal) can be involved, necessitating arthrodesis, partial joint resection, or amputation.
*
Bony Architecture:
While primarily a soft tissue sarcoma, CCS can invade adjacent bone, requiring en bloc osteotomy and reconstruction or local bone resection.
*
Skin and Soft Tissue Coverage:
The limited soft tissue envelope, particularly on the dorsal and plantar aspects of the foot, often results in significant soft tissue defects after wide resection, demanding advanced reconstructive techniques such as local, regional, or free flap coverage.
Biomechanically, the foot and ankle are critical for weight-bearing, propulsion, balance, and shock absorption. Any significant loss of muscle function, joint stability, or structural integrity due to tumor resection can severely compromise gait and functional independence. Surgical planning must therefore balance oncologic imperatives with reconstructive feasibility and functional preservation, recognizing that achieving adequate oncologic margins often takes precedence and may necessitate functional compromise or amputation. The goal is always to achieve the widest possible negative margins while minimizing functional morbidity to an acceptable level.
Indications & Contraindications
The management of clear cell sarcoma of the foot and ankle is dictated by the principles of sarcoma surgery, emphasizing en bloc resection with negative margins.
Table 1: Operative vs. Non-Operative Indications for Clear Cell Sarcoma
| Category | Operative Indications | Non-Operative Indications (Relative/Absolute) |
|---|---|---|
| Primary Disease | - Biopsy-proven Clear Cell Sarcoma. | - Unresectable local disease (e.g., encasing critical neurovascular structures where resection would cause unacceptable morbidity without achieving negative margins). |
| - Resectable disease with the potential to achieve wide or marginal negative surgical margins. | - Widespread, rapidly progressive metastatic disease limiting life expectancy where local control offers minimal benefit. | |
| - Local recurrence after initial therapy, if amenable to re-resection. | - Significant patient comorbidities precluding major surgery. | |
| - Symptomatic local disease (e.g., pain, impending fracture) in select cases, even if unresectable, for palliation. | - Patient refusal of surgical intervention. | |
| Metastatic Disease | - Oligometastatic disease (e.g., isolated lung or bone metastasis) in highly selected patients, combined with systemic therapy, for improved survival or palliation. | - Diffuse, widespread metastatic disease. |
| Adjuvant/Neoadjuvant | - Pre-surgical biopsy and staging are always indicated to confirm diagnosis and plan surgery. | - Neoadjuvant chemotherapy or radiation may be considered to downstage a tumor or sterilize margins, but is not a substitute for definitive surgical resection. |
| Reconstruction | - Reconstruction of defects following oncologic resection is an integral part of operative management. |
Key Considerations:
*
Biopsy:
A definitive diagnosis via biopsy is a prerequisite for any definitive surgical intervention. The biopsy tract must be planned carefully to allow its complete excision with the definitive resection.
*
Multidisciplinary Approach:
All cases of CCS, particularly those in anatomically challenging locations like the foot and ankle, should be discussed at a dedicated multidisciplinary tumor board involving orthopedic oncologists, surgical oncologists, radiation oncologists, medical oncologists, radiologists, and pathologists.
*
Limb Salvage vs. Amputation:
The primary goal is oncologic control. If wide negative margins cannot be achieved with limb salvage, or if limb salvage would result in a non-functional or painful extremity, amputation is indicated. This decision is complex and requires thorough pre-operative counseling regarding functional outcomes.
Pre-Operative Planning & Patient Positioning
Comprehensive pre-operative planning is crucial for optimizing oncologic and functional outcomes in CCS of the foot and ankle.
Diagnostic Workup and Staging
- Clinical Evaluation: Thorough history and physical examination, focusing on the character of the mass (size, consistency, mobility, tenderness), neurological status (sensory/motor deficits), and vascular integrity distal to the mass. Regional lymph node examination is essential due to the propensity for lymphatic spread.
-
Imaging:
- Magnetic Resonance Imaging (MRI): The gold standard for local staging. It provides detailed information on tumor size, exact anatomical location, relationship to neurovascular bundles, bone, joints, and adjacent soft tissue compartments. T1-weighted, T2-weighted with fat suppression, and post-contrast T1-weighted sequences are typically utilized. MRI helps delineate the extent of peritumoral edema and identify skip lesions.
-

Figure 1: Pre-operative MRI depicting a soft tissue mass in the foot/ankle, illustrating its anatomical relationship to surrounding structures. High-resolution imaging is crucial for accurate staging and surgical planning in clear cell sarcoma. -
Computed Tomography (CT) Scan:
- Chest: Essential for evaluating pulmonary metastases, which are common in CCS.
- Local (with contrast): Can be complementary to MRI, particularly for assessing bone involvement and cortical integrity.
- Abdomen/Pelvis: Considered for complete metastatic workup, though less common sites for CCS metastases compared to lung.
- Positron Emission Tomography (PET-CT): Useful for detecting occult distant metastases and assessing regional lymph node involvement, aiding in overall staging.
- Biopsy: A percutaneous core needle biopsy (CNB) performed by an experienced musculoskeletal radiologist or orthopedic oncologist is often sufficient for diagnosis. For larger or diagnostically challenging lesions, an incisional biopsy may be required. Crucially, the biopsy tract must be placed such that it can be completely excised en bloc with the definitive tumor resection. Poorly planned biopsies can compromise subsequent limb salvage efforts or necessitate a more extensive resection.
- Multidisciplinary Tumor Board (MDTB) Review: All findings should be presented at a dedicated MDTB to formulate the optimal treatment strategy, considering neo-adjuvant or adjuvant therapies (radiation, chemotherapy) in addition to surgery.
Surgical Planning
- Margin Assessment: Based on imaging and biopsy results, a detailed plan for achieving wide (or at least marginal) negative surgical margins is developed. This often involves sacrificing adjacent structures (muscle, tendon, nerve, vessel, bone) to ensure complete tumor excision. The Enneking staging system guides surgical margin determination.
-
Reconstruction Strategy:
Given the potential for large soft tissue or bony defects, a reconstructive plan must be in place. This may involve:
- Soft Tissue: Primary closure (rare for wide resections), local or regional flaps (e.g., reverse sural flap, posterior tibial artery perforator flap), or free tissue transfer (e.g., anterolateral thigh flap, latissimus dorsi flap) for large defects. Plastic surgery consultation is often essential.
- Bone/Joint: Allografts, autografts, cement spacers, prosthetic replacement, or arthrodesis.
- Patient Education: Comprehensive discussion with the patient regarding the extent of resection, potential functional deficits, reconstructive options, and the possibility of amputation.
Patient Positioning
- Supine, Prone, or Lateral Decubitus: Position depends on the tumor's location (e.g., plantar lesion typically prone, dorsal lesion supine).
- Tourniquet: A pneumatic tourniquet applied proximally on the thigh is essential for a bloodless field, which is critical for precise dissection and identification of tumor margins.
- Anesthesia: General anesthesia is typically employed. Regional nerve blocks can be beneficial for post-operative pain control.
- Pre-operative Imaging/Marking: The tumor may be marked on the skin pre-operatively, and fluoroscopy or ultrasound can be used intra-operatively to confirm position for deeper lesions.
Detailed Surgical Approach / Technique
The cornerstone of CCS management in the foot and ankle is wide en bloc surgical resection with the goal of achieving negative microscopic margins. This often requires aggressive removal of surrounding normal tissue due to the infiltrative nature of the tumor.
General Principles
- En Bloc Resection: The tumor, along with a cuff of normal surrounding tissue, and the entire biopsy tract must be removed as a single specimen.
- Wide Margins: The target is a wide margin (typically >2 cm of uninvolved tissue in all planes). In the anatomically constrained foot and ankle, achieving true wide margins can be challenging, and marginal margins (tumor adjacent to but not violating the pseudocapsule, excised with a narrow cuff of normal tissue) may be accepted if further resection would cause unacceptable morbidity or amputation. However, narrow or positive margins significantly increase the risk of local recurrence.
- Bloodless Field: Tourniquet use is mandatory to ensure clear visualization of fascial planes, neurovascular structures, and tumor boundaries.
- Avoid Tumor Spillage: Meticulous technique to prevent capsular violation or tumor cell dissemination.
- Reconstruction: Planning for defect reconstruction must be concurrent with the resection plan.
Step-by-Step Dissection and Resection
-
Incision:
An elliptical incision is designed to encompass the biopsy scar and the planned wide margins around the tumor. The long axis of the ellipse should generally be longitudinal to respect tension lines and facilitate closure or flap reconstruction.
- The skin incision should extend beyond the anticipated deep margins to allow adequate soft tissue mobilization.
-
Initial Dissection and Exposure:
- Subcutaneous dissection proceeds carefully to raise skin flaps, exposing the deep fascia while maintaining the planned margin of subcutaneous tissue overlying the tumor.
- Identify and ligate or clip superficial neurovascular structures that are within the planned resection zone.
- Carefully expose the tumor, making sure never to directly touch or dissect on the tumor pseudocapsule. All dissection should proceed through normal, uninvolved tissue.
-
Delineating Deep Margins:
- The most challenging aspect is often achieving deep and circumferential margins in the foot and ankle due to complex anatomy.
- Internervous Planes: While these are ideal for dissection in other contexts, CCS often invades along fascial planes, tendons, and neurovascular bundles, necessitating sacrifice of these structures if they are in close proximity or involved.
- Neurovascular Bundles: Major nerves and vessels that are directly involved by the tumor or lie within the necessary resection margin must be sacrificed. For critical vessels, pre-operative angiography and planning for vascular reconstruction (e.g., vein graft) may be required. For critical nerves, primary repair, nerve grafting, or acceptance of sensory/motor deficit is necessary.
- Tendons: If a tendon is involved, the entire segment (or the entire tendon if critical for function and difficult to reconstruct partially) within the margin is resected. Tendon reconstruction (graft, transfer, arthrodesis for stabilization) is often required.
- Bone Involvement: If imaging suggests cortical erosion or medullary invasion, an en bloc osteotomy of the affected bone segment is performed. This may involve partial bone resection, segmentectomy, or joint resection.
-
En Bloc Excision:
Once all margins are delineated, the specimen is carefully removed as a single unit. The orientation of the specimen should be marked (e.g., with sutures, clips, or ink) for the pathologist to accurately assess margins.
-
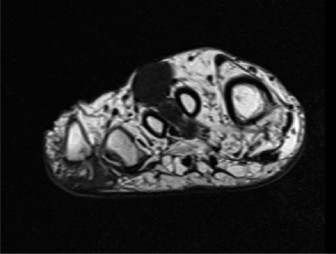
Figure 2: Intraoperative view during wide en bloc resection of a clear cell sarcoma from the foot. Note the careful dissection around the tumor, ensuring a generous cuff of normal tissue is maintained to achieve negative margins. The biopsy tract is also clearly visible within the resected specimen.
-
- Frozen Section Analysis (Optional but Recommended): While definitive margins are histological, intraoperative frozen section analysis can be valuable, particularly for critical margins (e.g., close to neurovascular structures, bone). If positive margins are identified, further resection is performed.
-
Defect Management and Reconstruction:
- After tumor removal, the defect is assessed.
-
Soft Tissue Reconstruction:
- Primary Closure: Rarely possible for wide resections.
- Skin Grafts: Only for superficial defects with a well-vascularized bed, but often unsuitable for complex foot and ankle defects needing robust soft tissue coverage.
- Local Flaps: (e.g., fasciocutaneous flaps) can cover smaller defects but may be limited by tissue availability and vascularity in previously irradiated or compromised areas.
- Regional Flaps: (e.g., reverse sural artery flap for posterior ankle/heel defects, posterior tibial artery perforator flap) offer more robust coverage and better vascularity.
- Free Flaps: (e.g., anterolateral thigh (ALT), latissimus dorsi) are often necessary for large, complex defects, especially those involving bone, tendon, or critical neurovascular structures, or when local tissue is inadequate. This often involves microvascular anastomoses.
-
Bone/Joint Reconstruction:
- Arthrodesis: Fusion of joints after intra-articular resection provides stability but sacrifices motion (e.g., tibiotalar, subtalar, or midtarsal fusion).
- Allografts/Autografts: Used to reconstruct bony defects, often combined with internal fixation.
- Prosthetic Implants: Rarely used for primary reconstruction in oncology due to infection risk and poor long-term integration in heavily irradiated fields.
- Amputation: If limb salvage is not oncologically feasible (positive margins, extensive involvement of critical structures) or would result in a non-functional, painful limb, amputation (e.g., transtibial, ankle disarticulation) is the most appropriate option for definitive local control and functional outcome.
-
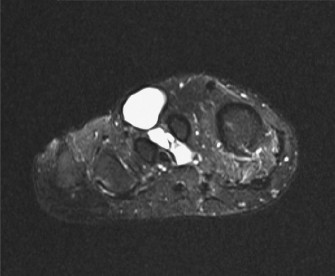
Figure 3: Post-operative imaging (e.g., plain radiograph or CT) demonstrating the reconstructed foot/ankle following wide resection of a clear cell sarcoma. This example shows an arthrodesis performed after resection of bony involvement, ensuring structural stability.
- Wound Closure: Careful layered closure of remaining tissues, ensuring no undue tension. Drains are often placed.
Complications & Management
Clear cell sarcoma, especially in the foot and ankle, is associated with a high rate of complications due to its aggressive nature, the complexity of local anatomy, and the extent of required surgical intervention.
Table 2: Common Complications, Incidence, and Salvage Strategies
| Complication | Incidence (Approx.) | Salvage Strategies |
|---|---|---|
| Local Recurrence | 30-50% | - Re-resection with wider margins (if feasible). |
| - Amputation (if re-resection fails or if margins are consistently positive/unachievable). | ||
| - Adjuvant radiation therapy (if not previously given). | ||
| - Consideration for systemic therapy. | ||
| Distant Metastasis | 50-70% (5-yr) | - Systemic therapy (chemotherapy, targeted agents, immunotherapy). |
| (Lungs, Bone, Lymph Nodes) | - Metastasectomy (for oligometastatic disease, especially pulmonary). | |
| - Palliative radiation for symptomatic bone/brain mets. | ||
| Wound Complications | 10-30% | - Debridement and secondary closure. |
| (Dehiscence, Infection, | - Antibiotic therapy for infection. | |
| Hematoma, Seroma) | - Flap coverage (local, regional, free) for dehiscence or necrosis. | |
| Flap/Graft Failure | 5-15% (for complex | - Revision surgery, debridement, re-exploration for vascular compromise. |
| reconstructions) | - Alternative flap options or amputation if salvage not possible. | |
| Functional Deficit | Highly variable | - Intensive physical and occupational therapy. |
| (Pain, Instability, Gait | (depends on extent | - Orthotics, bracing, custom footwear. |
| Disturbance, Nerve Palsy) | of resection) | - Nerve repair/grafting (if nerve sacrificed). |
| - Arthrodesis for instability. | ||
| - Pain management specialists, nerve blocks. | ||
| Lymphedema | 5-10% | - Compression therapy, manual lymphatic drainage. |
| - Lymphaticovenous anastomosis (LVA) or lymph node transfer (rare). | ||
| Amputation-Related | N/A (if amputation) | - Prosthetic fitting, gait training, stump care. |
| (Phantom Pain, Stump | - Medical/surgical management for phantom limb pain. | |
| Issues) | - Revision amputation for stump problems. | |
| Adjuvant Therapy Side Effects | Common | - Symptomatic management, dose adjustments. |
| (Radiation dermatitis, | - Nutritional support. | |
| myelosuppression from chemo) | - Referrals to specialists (dermatology, palliative care). |
Management Principles
- Proactive Surveillance: Lifelong follow-up with clinical examination, cross-sectional imaging (MRI of primary site, CT chest/abdomen/pelvis), and potentially PET-CT, is crucial for early detection of recurrence or metastasis.
- Multidisciplinary Team: Continued involvement of the MDTB is essential for guiding management strategies for complications, especially for metastatic disease or complex recurrences.
- Rehabilitation: Aggressive and tailored rehabilitation programs are vital to maximize functional recovery and adapt to any residual deficits.
- Patient Support: Psychological support is important given the aggressive nature of the disease and potential for significant morbidity.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following CCS resection in the foot and ankle is highly individualized, depending on the extent of resection, type of reconstruction, and the presence of adjuvant therapies. The primary goals are wound healing, pain control, restoration of range of motion (ROM), strengthening, gait training, and eventual return to functional activities.
Immediate Post-Operative Phase (Weeks 0-2/4)
- Pain Management: Multimodal analgesia, including regional nerve blocks, oral analgesics, and often NSAIDs/acetaminophen.
- Wound Care: Meticulous wound checks. Elevation of the limb to reduce swelling. Dressing changes as prescribed. Management of drains.
- Immobilization: The foot and ankle are typically immobilized in a splint, cast, or controlled ankle motion (CAM) boot to protect the surgical site and any reconstructions (flaps, tendon repairs, fusions).
- Weight-Bearing Status: Strictly non-weight-bearing (NWB) is generally mandated to protect the surgical site, especially if bone grafts, fusions, or extensive soft tissue repairs/flaps have been utilized.
- Early ROM: If safe and approved by the surgeon, gentle passive or active-assisted ROM of unaffected joints (e.g., knee, hip) may begin. For the ankle, protected ROM may start very cautiously, often passive, to prevent stiffness, but only if the reconstruction allows.
Intermediate Rehabilitation Phase (Weeks 4-12)
- Transition to Cast/Boot: Depending on wound healing and stability, the splint may be transitioned to a removable cast or CAM boot.
- Gradual Weight-Bearing: Under strict guidance, progressive weight-bearing (PWB) is initiated, typically with crutches or a walker. This is often guided by radiographic evidence of healing for bone reconstructions/fusions.
- ROM and Flexibility: Active and active-assisted ROM exercises for the ankle and foot, focusing on regaining dorsiflexion, plantarflexion, inversion, and eversion, as allowed by the specific reconstruction. Gentle stretching exercises.
- Strengthening: Isometrics of surrounding musculature. As pain permits, resistive exercises with bands or light weights for intrinsic foot muscles and ankle stabilizers.
- Proprioception and Balance: Begin with simple balance exercises (e.g., single leg stance on stable surface) once sufficient weight-bearing and stability are achieved.
- Scar Management: Desensitization, massage, and silicone sheeting to improve scar mobility and reduce hypersensitivity.
Advanced Rehabilitation Phase (Weeks 12+)
- Full Weight-Bearing (FWB): Progression to FWB as tolerated and indicated by healing.
- Functional Strengthening: Advanced strengthening exercises targeting specific muscle groups, including eccentric loading and plyometrics where appropriate.
- Gait Training: Intensive gait retraining to normalize walking patterns, reduce compensatory movements, and improve efficiency. May include treadmill walking, obstacle courses.
- Activity-Specific Training: For patients returning to higher-level activities or sports, sport-specific drills, agility training, and progressive impact loading exercises.
- Orthotics/Bracing: Prescription of custom orthotics or braces to support the foot and ankle, distribute pressure, or compensate for muscle weakness/instability.
- Long-Term Monitoring: Continued focus on maintaining ROM, strength, and preventing stiffness or pain. Regular follow-up with the surgeon and therapist.
Specific Considerations
- Adjuvant Radiation Therapy: If post-operative radiation is administered, rehabilitation may be paused or modified during the acute phase of treatment due to skin reactions, fatigue, and potential for delayed wound healing. Exercises will focus on maintaining ROM and preventing contractures without stressing radiated tissues.
- Chemotherapy: The systemic side effects of chemotherapy (fatigue, myelosuppression, neuropathy) can impact participation and progression in rehabilitation.
- Nerve Injury: If significant nerve sacrifice was required, specific nerve rehabilitation protocols, nerve gliding exercises, and sensory re-education are incorporated. Patients must be educated on protective sensation deficits.
- Amputee Rehabilitation: For patients undergoing amputation, rehabilitation focuses on stump care, prosthetic fitting, training in prosthetic use, and advanced gait training to maximize functional independence.
Throughout all phases, a close collaboration between the orthopedic oncologist, physical therapist, occupational therapist, and prosthetist (if applicable) is paramount to tailor the rehabilitation program to the individual's needs and optimize long-term functional outcomes.
Summary of Key Literature / Guidelines
The management of clear cell sarcoma, particularly in anatomically challenging areas like the foot and ankle, is guided by a combination of established sarcoma treatment principles and insights from a growing body of specialized literature. Given its rarity, evidence is often derived from retrospective series, case reports, and expert consensus.
-
NCCN Guidelines (National Comprehensive Cancer Network):
- The NCCN Clinical Practice Guidelines in Oncology for Soft Tissue Sarcoma are the most widely recognized and frequently updated comprehensive guidelines.
- They emphasize the importance of multidisciplinary tumor board evaluation for all sarcoma patients, ensuring input from orthopedic oncologists, surgical oncologists, radiation oncologists, medical oncologists, pathologists, and radiologists.
- Biopsy by an experienced individual (musculoskeletal radiologist or surgeon) is critical for diagnosis and should be performed prior to definitive treatment planning. The biopsy tract must be excisable.
- Surgical resection with wide, negative margins remains the cornerstone of curative treatment for localized CCS. Achieving R0 resection (no residual microscopic tumor) is the most significant prognostic factor for local control and survival.
- Adjuvant radiation therapy is generally recommended for high-grade sarcomas (which CCS typically is) or those with close/positive margins, or large size (>5 cm), to reduce local recurrence risk, especially in the foot/ankle where achieving wide margins can be difficult. The role of neoadjuvant radiation is also considered for large, borderline resectable tumors.
- The role of adjuvant chemotherapy in CCS is debated. While some studies suggest a benefit, particularly for metastatic disease or high-risk features, others have not shown a clear survival advantage. It is often considered in the metastatic setting or as part of a clinical trial.
- Systemic therapy for metastatic CCS is evolving, with traditional chemotherapies (e.g., doxorubicin, ifosfamide) having limited efficacy. Newer approaches target the EWSR1-ATF1 fusion protein, and clinical trials investigating molecularly targeted agents and immunotherapies are ongoing.
-
Orthopedic Oncology Consensus:
- Centralization of Care: Patients with CCS, particularly in the foot and ankle, should be managed at specialized high-volume sarcoma centers by orthopedic oncologists and their multidisciplinary teams. This specialization has been shown to improve outcomes.
- Limb Salvage vs. Amputation: The primary determinant is oncologic safety (achieving negative margins). Functional outcome is secondary but important. Amputation is a valid and often necessary procedure to achieve definitive local control when limb salvage compromises margins or results in a non-functional limb.
- Margin Assessment: The difficulty of achieving adequate margins in the foot and ankle due to anatomical constraints necessitates careful pre-operative planning, intraoperative assessment (including frozen sections), and potentially more aggressive resection (e.g., ray amputation, ankle disarticulation).
- Reconstruction: Complex soft tissue and bony reconstructions are often required. Collaboration with plastic surgeons and microvascular specialists is essential for limb salvage success.
-
Key Literature & Evolving Concepts:
- Numerous retrospective series highlight the aggressive nature of CCS, its high metastatic potential, and the prognostic significance of tumor size, depth, presence of necrosis, and most importantly, surgical margin status.
- The identification of the EWSR1-ATF1 fusion gene is not only diagnostic but also a potential target for novel therapies. Research into kinase inhibitors and other targeted agents is a rapidly evolving field.
- Immunotherapy: Given its historical link to melanoma, there is interest in checkpoint inhibitors, though current data for CCS specifically are limited to case reports and small series, suggesting potential but not yet established widespread efficacy.
- Lymph Node Management: CCS has a relatively high rate of regional lymph node metastasis. Consideration for sentinel lymph node biopsy, or therapeutic lymphadenectomy for clinically involved nodes, is important in staging and management.
- Surveillance: Long-term follow-up protocols are crucial due to the potential for late local recurrence and distant metastasis, necessitating regular clinical examinations, MRI of the primary site, and CT scans of the chest.
In summary, the optimal management of clear cell sarcoma of the foot and ankle requires a rigorous, multidisciplinary approach, with surgical extirpation aiming for wide, negative margins remaining the cornerstone of treatment, often complemented by adjuvant radiation therapy and evolving systemic therapies for advanced disease.
Clinical & Radiographic Imaging

