Navicular Fractures: Comprehensive Guide to Etiology, Anatomy, Biomechanics & Diagnosis

Key Takeaway
Navicular fractures are critical foot injuries, often caused by high-energy trauma or stress, threatening midfoot stability. Diagnosis relies on plain radiographs, revealing cortical disruptions or alignment changes, often supplemented by CT scans for detailed fracture morphology. Understanding the navicular's precarious blood supply and biomechanical role is crucial for managing AVN risk and preventing long-term morbidity.
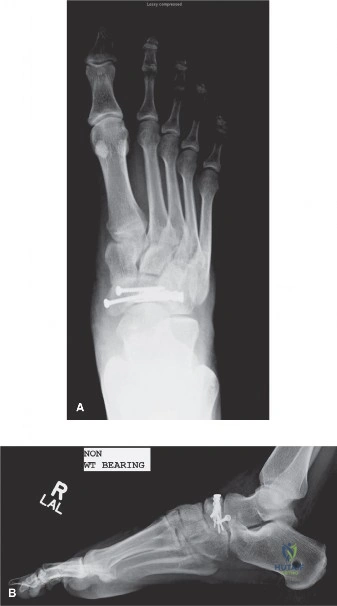
A 28-year-old male presents following a high-energy fall from a height. He has significant swelling over the dorsomedial aspect of the midfoot. Examination shows skin tenting and tenderness over the navicular. This is his initial AP radiograph.
Describe your assessment of this patient and the immediate next steps.
Candidate: I would perform a primary survey (ATLS) to rule out associated injuries. I note the cortical irregularity and potential midfoot malalignment on the X-ray. I would order a CT scan of the foot to classify the fracture, specifically looking for articular involvement, and manage the patient with elevation and a splint to protect the soft tissue envelope.
Failure to comment on the specific "medial column" integrity, neglecting to mention the soft tissue assessment (the "wrinkle sign"), or jumping straight to "I would operate" without confirming the Sangeorzan classification or the patient's physiological suitability for surgery.
Systematically address: 1. Hemodynamic/polytrauma clearance. 2. Neurovascular status of the foot. 3. Soft tissue status (checking for blistering/tenting). 4. Radiological assessment (Meary's angle/medial column collapse). 5. Definitive imaging (CT scan is mandatory for Sangeorzan classification). 6. Staged management (elevation until soft tissues are fit for surgery). Always emphasize "respecting the soft tissue envelope."
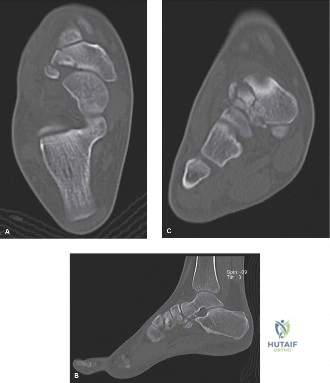
The CT scan confirms a Sangeorzan Type 2 fracture. Here is the patient's lateral radiograph following the trauma.
Explain the significance of the medial column in this context and how you would surgically approach this fixation.
Candidate: The navicular is the keystone of the medial longitudinal arch. Loss of its integrity leads to midfoot sag and collapse. I would utilize a dorsomedial approach, perform indirect reduction using distraction to restore the medial column length, and fixate with a combination of headless compression screws and a low-profile dorsal locking plate.
Ignoring the blood supply (dorsal/plantar arcades). Candidates often forget to mention bone graft usage in comminuted fractures or fail to discuss the risks of AVN associated with aggressive periosteal stripping during the approach.
Clearly explain the biomechanics: The navicular as the 'keystone' and the risk of arch collapse. Discuss the Sangeorzan Type 2 as a compression/medial dislocation pattern. Detail the surgical plan: Dorsomedial incision, ligamentotaxis for reduction, headless screws for interfragmentary compression, and potentially locking plate fixation to bridge comminution. Mention the need for bone graft for metaphyseal voids and the absolute necessity of preserving the blood supply by minimizing periosteal stripping.
You are presented with this complex CT reconstruction during the viva.
What are the potential long-term complications you would counsel the patient about, and how would you manage a established post-traumatic arthritis in this joint?
Candidate: Long-term risks include avascular necrosis, nonunion, and post-traumatic arthritis. If arthritis becomes symptomatic, I would initially manage conservatively with orthotics. If this fails, I would recommend a talonavicular or naviculocuneiform arthrodesis.
Suggesting joint replacement for the navicular. Total joint replacement in the midfoot is not a standard, evidence-based procedure. Candidates must recognize that arthrodesis is the gold standard for symptomatic post-traumatic arthritis in this region.
Structure the answer: 1. Complications (AVN, Nonunion, Arthritis). 2. Pathophysiology (Watershed zone vascularity). 3. Salvage (Arthrodesis: describe the joints targeted—talonavicular and naviculocuneiform). 4. Acknowledge the functional impact of stiffening these joints on foot biomechanics, showing an understanding of the long-term clinical picture.
