Displaced Talar Neck Fractures: Comprehensive Management, Anatomy, and Outcomes

Key Takeaway
Displaced talar neck fractures, categorized by Hawkins classification (Types II-IV), are high-energy injuries with significant risks of avascular necrosis (AVN) and post-traumatic arthritis. Optimal treatment necessitates anatomic reduction and stable internal fixation to restore joint congruity, critical for mitigating severe long-term complications given the talus's precarious blood supply.
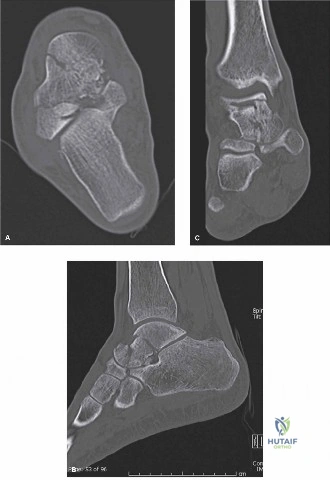
A 32-year-old male presents to the Emergency Department following a high-energy motorcycle collision. He has a deformed, painful ankle. On examination, there is tense swelling and skin tenting over the medial aspect of the ankle. Radiographs are obtained. Describe your findings and initial management.

Candidate: The radiograph shows a displaced talar neck fracture. Based on the associated subtalar dislocation, I would classify this as a Hawkins Type II fracture. My immediate management would be an urgent closed reduction under sedation to relieve pressure on the skin, followed by neurovascular assessment and limb splinting. If reduction is unsuccessful or the skin is threatened, I would proceed to emergent open reduction.
Failure to immediately recognize the emergency of the skin tenting and neurovascular status. Candidates often jump straight to "I will book for ORIF" without addressing the immediate threat to the soft tissues (impending skin necrosis) and the potential for a closed reduction to act as a "damage control" procedure.
A systematic approach: 1. Assessment: Confirm the neurovascular status (dorsalis pedis/PT pulses, sensation). 2. Recognition: Identify it as a Hawkins Type II (subtalar subluxation/dislocation). 3. Immediate Action: Recognize that the medial skin tenting is a surgical emergency; if irreducible by immediate closed reduction, the patient requires emergent open reduction to prevent skin necrosis. 4. Imaging: Mention the necessity of a CT scan for 3D mapping once the soft tissue envelope is stable/reduced.
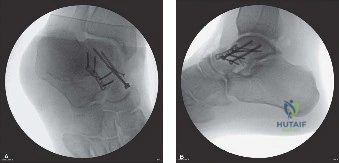
You have decided to proceed with open reduction and internal fixation. Describe your preferred surgical approach and the rationale for your choice of incision to minimize complications.
Candidate: I would use an anteromedial approach, as it allows direct visualization of the talar neck and minimizes damage to the lateral vascular supply. If there is significant comminution or displacement that remains irreducible, I would add an anterolateral approach as a second window to allow for a cross-screw construct.
Forgetting the "danger" of over-stripping soft tissues. Failing to mention the saphenous nerve and vein in the medial approach or the superficial peroneal nerve in the lateral approach marks the candidate as lacking anatomical rigor.
State that the anteromedial approach is the workhorse. Emphasize the importance of protecting the deltoid branch of the posterior tibial artery to preserve blood supply. Mention that using dual incisions (medial and lateral) is often necessary for complex fractures to achieve an anatomic, convergent, crossed-screw construct without relying on a single, suboptimal screw trajectory.
The surgery was completed successfully. Six weeks post-operatively, you review the patient in clinic. The patient is pain-free, but you notice a specific radiographic sign on the plain films. What is it, and what does it tell you about the prognosis for avascular necrosis (AVN)?
Candidate: I am looking for the Hawkins sign, which is a subchondral lucency in the talar dome. Its presence at 6-8 weeks suggests that the talus is revascularizing, which significantly decreases the concern for AVN.
Confusing the Hawkins sign with a fracture line or failing to realize that the sign must be viewed on a weight-bearing or neutral AP ankle view to be accurately assessed.
Correctly identify this as the Hawkins sign. Explain the pathophysiology: it represents subchondral atrophy occurring in viable bone; therefore, its presence confirms an intact vascular supply to the talar body. Conversely, emphasize that absence of the sign is not diagnostic of AVN, but necessitates continued vigilance for collapse.
