Introduction and Epidemiology
Chronic foot and ankle pain is a ubiquitous presenting complaint in orthopedic practice, often posing diagnostic and therapeutic challenges. While myriad pathologies can contribute, conditions affecting the flexor digitorum longus tendon and its surrounding synovial sheath represent a distinct subset that, when appropriately identified, can benefit from targeted surgical intervention. Debridement of the flexor digitorum longus tendon or its surrounding synovium is a procedure indicated for refractory tenosynovitis, tendinopathy, longitudinal split tears, or specific instances of tendon involvement in complex hindfoot and midfoot deformities.
Flexor digitorum longus tenosynovitis, characterized by acute or chronic inflammation of the tendon sheath, typically presents with insidious onset pain along the posteromedial ankle and medial midfoot. This pain is classically exacerbated by weight-bearing activity, single-limb heel rise, and resisted lesser toe flexion. Tendinopathy, encompassing intrinsic degenerative changes within the tendon substance (tendinosis) without necessarily involving the sheath, can manifest with similar clinical symptoms but frequently includes palpable nodularity, fusiform thickening, or crepitus along the tendon course.
The incidence of isolated flexor digitorum longus pathology is not as well-defined in the orthopedic literature as more prevalent conditions such as Achilles tendinopathy, plantar fasciitis, or posterior tibial tendon dysfunction. Isolated flexor digitorum longus tears or severe tendinopathy are considered rare clinical entities. More commonly, flexor digitorum longus pathology is a concurrent finding or a secondary complaint in the context of advanced posterior tibial tendon dysfunction, accessory navicular syndrome, flexor hallucis longus tenosynovitis, or tarsal tunnel syndrome.
Epidemiologically, this pathology is most frequently observed in highly active cohorts. Ballet dancers, gymnasts, and endurance runners are particularly susceptible due to the extreme ranges of motion and repetitive mechanical overload placed on the medial ankle structures during toe-off and en pointe positioning. Furthermore, anatomical variations leading to mechanical impingement, inflammatory arthropathies such as rheumatoid arthritis or seronegative spondyloarthropathies, and systemic metabolic conditions including diabetes mellitus can predispose individuals to flexor digitorum longus degeneration. A meticulous differential diagnosis is critical, requiring the clinician to distinguish flexor digitorum longus related pain from posterior tibial nerve entrapment, medial talar osteochondral lesions, spring ligament attenuation, or medial calcaneal nerve neuritis.
Surgical Anatomy and Biomechanics
A precise understanding of the flexor digitorum longus anatomy and its biomechanical role is paramount for surgical success, adequate decompression, and the avoidance of iatrogenic neurovascular injury.
Musculotendinous Anatomy
The flexor digitorum longus muscle originates from the posterior surface of the tibia, immediately distal to the soleal line, and medial to the vertical fascial septum separating it from the tibialis posterior muscle. Its robust tendon forms distally in the lower third of the leg, descending to pass through the tarsal tunnel posterior to the medial malleolus and deep to the flexor retinaculum (laciniate ligament).
Within the fibro-osseous tarsal tunnel, the flexor digitorum longus tendon lies anterior to the posterior tibial neurovascular bundle (comprising the posterior tibial artery, posterior tibial nerve, and venae comitantes) and posterior to the tibialis posterior tendon. The course of the flexor digitorum longus within this tunnel is often deep and immediately adjacent to the medial aspect of the sustentaculum tali of the calcaneus, a critical impingement zone where the tendon is subject to increased friction and mechanical compression.
Distal to the tarsal tunnel, the flexor digitorum longus tendon courses obliquely across the plantar aspect of the foot. It crosses superficial (plantar) to the flexor hallucis longus tendon in a highly consistent anatomical configuration known as the Master Knot of Henry, typically located deep to the navicular tuberosity or the medial cuneiform. At this intersection, a communicating tendinous slip often transfers from the flexor hallucis longus to the flexor digitorum longus, or vice versa, contributing to synergistic digital flexion.
Distal to the Master Knot of Henry, the flexor digitorum longus tendon bifurcates into four distinct slips directed toward the plantar aspects of the distal phalanges of the second through fifth digits. Each terminal slip is enclosed within its own synovial sheath and fibrous flexor pulley system. The quadratus plantae muscle, originating from the calcaneus, inserts directly into the posterolateral margin of the flexor digitorum longus tendon prior to its bifurcation, serving a critical role in modifying the tendon's vector of pull.
Key Anatomical Relationships
- Posterior Tibial Tendon: The flexor digitorum longus is deep and slightly posterior to the posterior tibial tendon at the level of the medial malleolus. The posterior tibial tendon lies most anterior within the tarsal tunnel.
- Flexor Hallucis Longus: The flexor digitorum longus crosses superficial to the flexor hallucis longus at the Master Knot of Henry. The flexor hallucis longus is the most posterior and lateral tendon within the tarsal tunnel.
- Neurovascular Bundle: The posterior tibial nerve and artery are superficial and posterior to the flexor digitorum longus within the retromalleolar space, making them highly susceptible to iatrogenic injury during a posteromedial surgical approach. The saphenous nerve and great saphenous vein are located more superficially and anteriorly in the subcutaneous tissues near the standard incision site.
Biomechanical Function
The flexor digitorum longus primarily functions to flex the distal interphalangeal, proximal interphalangeal, and metatarsophalangeal joints of the second through fifth digits. Secondary biomechanical actions include weak plantarflexion of the ankle joint and inversion of the subtalar joint.
Because the flexor digitorum longus tendon enters the foot from a posteromedial direction, its isolated contraction would theoretically result in oblique, medial deviation of the lesser toes during flexion. The quadratus plantae muscle corrects this oblique vector. By pulling the flexor digitorum longus tendon laterally, the quadratus plantae aligns the force vector along the longitudinal axis of the digits, enabling straight sagittal plane flexion. During the terminal stance and toe-off phases of the gait cycle, the flexor digitorum longus contributes to dynamic stabilization of the longitudinal arch, pressing the toe pads against the ground to expand the weight-bearing surface area and assist in forward propulsion.
Indications and Contraindications
Surgical intervention for flexor digitorum longus pathology is generally reserved for patients who have failed an exhaustive course of conservative management or those presenting with acute, high-grade traumatic ruptures requiring primary repair.
Operative vs Non Operative Management
| Clinical Scenario | Non Operative Management | Operative Management |
|---|---|---|
| Acute Tenosynovitis | First-line: Immobilization (CAM boot), NSAIDs, physical therapy, targeted corticosteroid injection (use with caution). | Indicated only if refractory to 3-6 months of conservative care. |
| Chronic Tendinosis | Eccentric strengthening, orthoses to correct hindfoot valgus, shockwave therapy. | Debridement of degenerative tissue, tubularization, synovectomy. |
| Longitudinal Split Tears | Immobilization, activity modification. | Surgical debridement, excision of the torn slip, primary repair or tubularization. |
| Complete Rupture | Conservative in low-demand, elderly patients. | Primary end-to-end repair or tenodesis to adjacent tendons in active patients. |
| Rheumatoid Nodules | Systemic DMARD therapy, local modalities. | Excisional debridement if causing mechanical block or severe pain. |
| Infection within Sheath | Suppressive antibiotics (rarely successful alone). | Emergent surgical irrigation and extensive debridement. |
| Concomitant Tarsal Tunnel | Orthoses, gabapentinoids, injections. | Tarsal tunnel release with concurrent flexor digitorum longus tenosynovectomy. |
Contraindications to Surgery
Absolute contraindications include active localized soft tissue infection (unless the procedure is explicitly an irrigation and debridement for infectious tenosynovitis) and severe peripheral arterial disease compromising surgical wound healing. Relative contraindications include poorly controlled diabetes mellitus, heavy tobacco use, complex regional pain syndrome, and medically unfit patients unable to tolerate anesthesia or comply with strict postoperative non-weight-bearing rehabilitation protocols. Operating on asymptomatic or incidentally discovered MRI pathology is strictly contraindicated.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning relies on a combination of detailed clinical examination and advanced imaging modalities to precisely localize the pathology and rule out concomitant medial ankle disorders.
Clinical Evaluation
Physical examination must evaluate the entire medial column and hindfoot. Palpation along the course of the flexor digitorum longus—from the retromalleolar space to the plantar midfoot—often elicits focal tenderness. The clinician should perform resisted lesser toe flexion with the ankle held in a neutral or slightly dorsiflexed position to isolate the flexor digitorum longus and provoke symptoms. Assessment of posterior tibial tendon strength (resisted inversion) and flexor hallucis longus strength (resisted hallux flexion) is mandatory to rule out combined pathology. Tinel's sign over the tarsal tunnel should be evaluated to assess for concurrent posterior tibial nerve entrapment secondary to space-occupying tenosynovitis.
Imaging Modalities
- Radiographs: Standard weight-bearing anteroposterior, lateral, and mortise views of the foot and ankle are obtained to assess overall foot morphotype (e.g., pes planovalgus), rule out medial malleolar or talar osseous pathology, and evaluate for accessory ossicles.
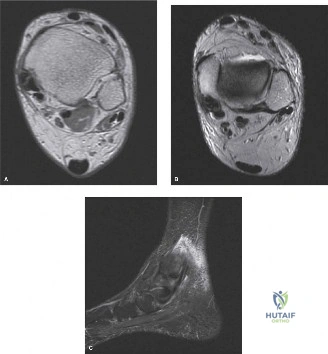
- Magnetic Resonance Imaging: MRI is the gold standard for evaluating tendon integrity. Axial and sagittal T2-weighted fluid-sensitive sequences are optimal for identifying tenosynovitis (circumferential fluid within the tendon sheath), tendinosis (intrasubstance signal alteration and tendon thickening), and longitudinal split tears.
- Ultrasound: High-resolution dynamic ultrasonography is highly sensitive for detecting tenosynovitis and allows for dynamic assessment of tendon gliding, subluxation, and localized impingement.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia or regional anesthesia (popliteal block) combined with intravenous sedation. The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to allow the leg to externally rotate naturally, providing optimal exposure to the medial ankle and hindfoot. A well-padded thigh tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying fine neurovascular structures. The operative extremity is prepped and draped in standard sterile fashion. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation.
Detailed Surgical Approach and Technique
The surgical approach for flexor digitorum longus debridement requires meticulous dissection through the posteromedial ankle, respecting the intricate fascial layers and the proximity of the posterior tibial neurovascular bundle.
Superficial Dissection and Exposure
A curvilinear longitudinal incision is made starting approximately 2 to 3 centimeters proximal to the tip of the medial malleolus, positioned midway between the posterior border of the medial malleolus and the medial border of the Achilles tendon. The incision is extended distally, curving gently following the course of the flexor tendons toward the navicular tuberosity.
Subcutaneous tissues are sharply divided. Care must be taken at the proximal and distal extents of the incision to identify and protect the terminal branches of the saphenous nerve and the great saphenous vein. The deep fascia of the leg is identified and incised in line with the skin incision.
Deep Dissection and Tarsal Tunnel Release
The flexor retinaculum (laciniate ligament) forms the roof of the tarsal tunnel. It is carefully incised longitudinally. It is critical to maintain the integrity of the posterior tibial neurovascular bundle, which lies immediately deep to the retinaculum and posterior to the flexor digitorum longus tendon.
Once the retinaculum is open, the posterior tibial tendon is identified as the most anterior and largest tendon. Immediately posterior to the posterior tibial tendon lies the flexor digitorum longus tendon. The neurovascular bundle is identified posterior to the flexor digitorum longus and gently retracted posteriorly using vessel loops or a delicate blunt retractor (e.g., a mini-Hohmann or Senn retractor).

Tendon Debridement and Synovectomy
The flexor digitorum longus tendon is systematically inspected from its musculotendinous junction proximally to its disappearance deep to the abductor hallucis muscle distally.
- Tenosynovectomy: If hypertrophic tenosynovitis is present, a radical synovectomy is performed. The inflamed synovial tissue is meticulously excised using a combination of sharp dissection, rongeurs, and electrocautery, taking care not to damage the underlying tendon epitenon or the delicate vincula supplying blood to the tendon.
- Debridement of Tendinosis: Areas of focal tendinosis (myxoid degeneration) presenting as fusiform swelling or discoloration are addressed. A longitudinal tenotomy may be performed in the center of the diseased segment to excise central necrotic or degenerative tissue.
- Management of Longitudinal Tears: If a longitudinal split tear is identified, the edges of the tear are debrided back to healthy, viable collagen. If the tear involves less than 50% of the tendon cross-sectional area, the diseased slip is excised. If the remaining tendon is substantial, it is tubularized using a running locking suture of 4-0 non-absorbable or slowly absorbable monofilament (e.g., Prolene or PDS) to restore a smooth gliding surface and prevent further propagation of the tear.
- Master Knot of Henry Exploration: If preoperative imaging or clinical examination suggests distal pathology, the incision is extended plantarly. The abductor hallucis fascia is released, and the muscle belly is retracted inferiorly to expose the plantar midfoot. The intersection of the flexor digitorum longus and flexor hallucis longus is identified. Fibrous adhesions or tenosynovitis at this intersection are sharply debrided.
Closure
Following thorough irrigation of the surgical site with sterile saline, the tourniquet is deflated to ensure meticulous hemostasis. The flexor retinaculum is loosely reapproximated using interrupted 2-0 or 3-0 absorbable sutures. Complete, tight closure of the retinaculum is avoided to prevent iatrogenic tarsal tunnel syndrome, but sufficient repair is necessary to prevent postoperative tendon bowstringing. The subcutaneous tissue is closed in a layered fashion using 3-0 absorbable sutures, and the skin is closed with a running subcuticular stitch or interrupted nylon sutures according to surgeon preference. A sterile, bulky, mildly compressive posterior splint is applied with the ankle in neutral dorsiflexion.
Complications and Management
While generally safe and effective, flexor digitorum longus debridement carries inherent risks, primarily related to the complex regional anatomy.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology and Pathomechanism | Management and Salvage Strategy |
|---|---|---|---|
| Posterior Tibial Nerve Injury | 1% - 3% | Iatrogenic laceration, traction neuropraxia, or entrapment in postoperative scar tissue. | Prevention is key. If neuropraxia occurs, observe with gabapentinoids. If lacerated, requires microsurgical primary repair or nerve grafting. |
| Medial Calcaneal Nerve Neuritis | 2% - 5% | Injury to small sensory branches during the distal extent of the surgical exposure. | Desensitization therapy, topical analgesics, targeted corticosteroid injections. Surgical excision of neuroma if refractory. |
| Tendon Rupture | < 1% | Over-aggressive debridement compromising >50% of tendon cross-section, or failure of tubularization. | Conservative management if asymptomatic. Tenodesis to flexor hallucis longus or posterior tibial tendon if symptomatic lesser toe dysfunction occurs. |
| Tendon Bowstringing | 1% - 2% | Complete failure to repair the flexor retinaculum, allowing the tendon to subluxate anteriorly during dorsiflexion. | Surgical revision with reconstruction of the flexor retinaculum using local tissue flaps or allograft. |
| Wound Dehiscence / Infection | 2% - 4% | Poor vascular supply to the medial ankle skin, excessive retraction, or hematoma formation. | Local wound care, oral or IV antibiotics. Surgical debridement and vacuum-assisted closure for deep space infections. |
| Recurrent Tenosynovitis | 5% - 10% | Incomplete synovectomy, failure to address underlying biomechanical overload (e.g., uncorrected pes planus). | Re-evaluation of foot biomechanics, orthotic management. Revision synovectomy is rarely required but may be considered. |
Post Operative Rehabilitation Protocols
A structured, phased rehabilitation protocol is essential to optimize tendon healing, restore normal glide, and prevent the formation of restrictive peritendinous adhesions.
Phase 1: Maximum Protection (Weeks 0 to 2)
The patient is placed in a well-padded posterior splint or short leg cast immediately postoperatively. The ankle is maintained in a neutral position to minimize tension on the debrided tendon. The patient is strictly non-weight-bearing on the operative extremity, utilizing crutches or a knee scooter. Strict elevation above the level of the heart is encouraged to minimize edema and promote wound healing. At two weeks, sutures are removed, and the wound is evaluated.
Phase 2: Early Mobilization and Progressive Weight Bearing (Weeks 2 to 6)
Following suture removal, the patient is transitioned to a controlled ankle motion (CAM) boot. Weight-bearing is progressively advanced from partial to full weight-bearing as tolerated over the next four weeks.
Physical therapy is initiated with a focus on:
* Active and passive range of motion of the ankle joint (sagittal plane only initially).
* Passive range of motion of the lesser toes to promote flexor digitorum longus tendon gliding and prevent adhesions.
* Crucial restriction: Active, resisted flexion of the lesser toes is strictly prohibited during this phase to protect the healing tendon substance and tubularization sutures.
* Isometric strengthening of the intrinsic foot musculature.
Phase 3: Strengthening and Proprioception (Weeks 6 to 12)
The CAM boot is discontinued, and the patient transitions to supportive athletic footwear, often supplemented with a custom orthotic to support the medial longitudinal arch if underlying valgus alignment exists.
Therapy progresses to include:
* Gentle, progressive active resisted flexion of the lesser toes.
* Eccentric strengthening of the flexor digitorum longus and posterior tibial tendons.
* Closed kinetic chain exercises (e.g., double-leg heel raises progressing to single-leg heel raises).
* Proprioceptive training utilizing wobble boards and uneven surfaces.
Phase 4: Return to Sport and Advanced Activity (Weeks 12+)
Patients are cleared to gradually resume high-impact activities, running, and sport-specific drills. Return to sport is contingent upon achieving symmetric ankle and toe strength, full pain-free range of motion, and the absence of swelling after activity. Dancers and gymnasts may require a more prolonged phase of sport-specific rehabilitation to safely return to extreme plantarflexion and en pointe maneuvers without reproducing tendinopathic symptoms.
Summary of Key Literature and Guidelines
The academic literature regarding isolated flexor digitorum longus pathology is relatively sparse compared to other foot and ankle tendinopathies, largely consisting of anatomical studies, case reports, and small retrospective case series.
Classical anatomical studies by Sarrafian and later by various anatomical researchers have meticulously documented the variable anatomy of the Master Knot of Henry and the intricate interconnections between the flexor digitorum longus and flexor hallucis longus. These studies underscore the necessity of exploring this distal intersection in cases of chronic medial midfoot pain, as isolated tenosynovitis can localize strictly to this chiasm.
Literature evaluating the surgical outcomes of tenosynovectomy for flexor digitorum longus pathology generally reports favorable results. Retrospective series have demonstrated that in patients with chronic, MRI-confirmed tenosynovitis who fail conservative care, surgical debridement yields high rates of pain relief and return to pre-injury activity levels. However, these studies consistently emphasize that the success of the procedure is highly dependent on accurately ruling out concomitant posterior tibial tendon dysfunction. If early-stage posterior tibial tendon dysfunction is missed and only the flexor digitorum longus is debrided, clinical failure and progressive arch collapse are inevitable.
Current surgical guidelines and expert consensus recommend a conservative-first approach for all non-traumatic flexor digitorum longus tendinopathies. Operative intervention is strictly reserved for those with persistent symptoms beyond three to six months, or those with imaging evidence of significant structural tendon tearing that threatens the biomechanical integrity of lesser toe flexion. Advanced imaging, particularly MRI, remains the gold standard guideline recommendation for preoperative surgical planning to delineate the extent of tendinosis and map the precise anatomical zones requiring debridement.
