Dupuytren Contracture: Comprehensive Pathoanatomy and Surgical Management

Key Takeaway
Dupuytren contracture is a progressive fibroproliferative disorder of the palmar fascia, characterized by the formation of nodules and cords that lead to irreversible flexion contractures of the digits. Surgical intervention, typically regional fasciectomy, is indicated for metacarpophalangeal joint contractures exceeding 30 degrees or any functional proximal interphalangeal joint contracture. Understanding the complex pathoanatomy, particularly the displacement of neurovascular bundles by the spiral cord, is critical for safe surgical execution.
Introduction to Dupuytren Disease
Dupuytren disease is a progressive, proliferative fibroplasia of the subcutaneous palmar tissue. It manifests primarily through the formation of palpable nodules and hypertrophic cords, which ultimately result in secondary, progressive, and irreversible flexion contractures of the finger joints. Beyond the mechanical contracture of the digits, secondary changes to the integumentary system are prominent. These include the thinning of the overlying subcutaneous fat, dense adhesion of the fibrotic tissue to the dermis, and subsequent pitting or dimpling of the palmar skin.
The clinical behavior of the lesion and the ensuing rate of deformity are highly variable. In a minority of cases, a digit may become markedly flexed within a few weeks or months; however, the development of a severe, functionally limiting deformity typically requires several years. The natural history of the disease is unpredictable. In some patients, the lesion progresses steadily and relentlessly, whereas in others, it is characterized by distinct exacerbations and prolonged remissions. Spontaneous regression of established cords is exceedingly rare.
Epidemiology and Risk Factors
Dupuytren contracture predominantly affects adults in their fourth to sixth decades of life and exhibits a striking gender disparity, occurring up to ten times more frequently in men than in women. Furthermore, the onset of the disease occurs significantly earlier in men (typically between 33 and 63 years of age) compared to women (46 to 70 years of age).
The condition is most prevalent in individuals of Northern European descent, particularly those of Scandinavian and Celtic origin, leading to its historical moniker, the "Viking disease." While it has been reported occasionally in populations of African descent and rarely in Asian populations, the genetic predisposition remains strongly linked to Caucasian ethnicity.
Several systemic conditions and lifestyle factors have been implicated in the pathogenesis or exacerbation of Dupuytren disease:
* Diabetes Mellitus: The lesion is reported to be more frequent and often more severe in diabetic patients, though it frequently presents with a milder, more diffuse palmar fascial thickening rather than discrete, aggressive cords.
* Epilepsy: Historically, up to 42% of institutionalized patients with epilepsy were noted to have Dupuytren-like changes, though this may be confounded by the long-term use of certain antiepileptic medications (e.g., phenobarbital).
* Substance Use: Conflicting reports exist regarding the association with alcoholism, but cigarette smoking and microvascular insufficiency have been strongly linked as causative or exacerbating factors.
* Trauma: While the exact etiology remains idiopathic, trauma to the hand and repetitive manual labor may contribute. The presence of hemosiderin in excised lesions suggests micro-hemorrhage from fascial tears. However, because the nondominant hand is affected as frequently as the dominant hand, mechanical trauma alone is insufficient to cause the disease. A single focal injury may precipitate the onset in genetically susceptible individuals (McFarlane's criteria).
Clinical Pearl: In patients with bilateral disease, if trauma is the suspected precipitating factor, the disease typically develops in the uninjured hand after age 40 in men and age 50 in women.
The Dupuytren Diathesis
Ectopic deposits of fibromatosis may occur in a variety of extra-palmar anatomical areas. Patients presenting with these associated findings are considered to have a "Dupuytren diathesis." This diathesis indicates a highly aggressive, genetically driven form of the disease, characterized by an earlier age of onset, rapid progression, and a significantly higher rate of postoperative recurrence.
The classic components of the Dupuytren diathesis include:
1. Knuckle Pads (Garrod's Nodes)
These are benign, fibrous thickenings found on the dorsum of the proximal interphalangeal (PIP) joints. They are a hallmark of aggressive systemic fibroplasia.
2. Ledderhose Disease (Plantar Fibromatosis)
Approximately 5% of patients with Dupuytren contractures develop similar nodular lesions in the medial plantar fascia of one or both feet. Unlike palmar disease, plantar fibromatosis rarely causes toe contractures but can be locally painful during weight-bearing.

Bilateral involvement is common in severe diathesis, presenting as firm, fixed masses in the medial arch of the foot.

3. Peyronie Disease
Occurring in approximately 3% of patients with Dupuytren disease, Peyronie disease involves plastic induration and fibrosis of the tunica albuginea of the penis, leading to penile curvature and painful erections.
Surgical Warning: Patients exhibiting a strong Dupuytren diathesis (early onset, bilateral involvement, ectopic lesions, strong family history) must be counseled extensively regarding the high likelihood of recurrence following any surgical intervention. Dermofasciectomy with full-thickness skin grafting may be indicated in these high-risk patients to reduce recurrence rates.
Pathoanatomy and Biomechanics
Understanding the transformation of normal palmar fascia into pathological cords is the cornerstone of safe surgical management. The disease process typically begins in line with the ring finger at the distal palmar crease and progresses to involve the ring and little fingers. These two digits are affected more frequently than all other digits combined.
Normal Fascia vs. Pathological Cords
Dupuytren disease does not create new anatomical structures; rather, it hypertrophies and contracts existing normal fascial bands.
- Pretendinous Band $\rightarrow$ Central Cord: The normal pretendinous band hypertrophies to form the central cord. Contraction of this cord causes isolated flexion contracture of the metacarpophalangeal (MCP) joint.
- Natatory Ligament $\rightarrow$ Natatory Cord: Hypertrophy of the natatory ligaments creates the natatory cord, which restricts digital abduction, leading to web space contractures.
- Lateral Digital Sheet $\rightarrow$ Lateral Cord: This cord can contribute to PIP joint contracture and is often intimately involved with the neurovascular bundle.
- The Spiral Cord: This is the most surgically critical structure. It is formed by the confluence of four normal structures: the pretendinous band, the spiral band, the lateral digital sheet, and Grayson's ligament.
Surgical Warning: The Spiral Cord and Neurovascular Displacement
As the spiral cord contracts, it produces a severe PIP joint contracture. More importantly, its biomechanical shortening pulls the neurovascular bundle centrally, superficially, and proximally. During surgical approach to the PIP joint, the neurovascular bundle may lie directly beneath the skin and is at extreme risk of iatrogenic transection if the surgeon expects it to be in its normal volar-lateral anatomical position.
Histopathology and Disease Stages
The pathogenesis of Dupuytren contracture is driven by the myofibroblast, a specialized cell exhibiting characteristics of both fibroblasts and smooth muscle cells. The disease progresses through three distinct histological stages, originally described by Luck:
1. Proliferative Stage
This stage is characterized by intense cellularity. Young, non-stress-aligned fibroblasts and myofibroblasts proliferate rapidly, expanding and displacing the subcutaneous tissues. These cells fuse to the overlying dermis, creating the classic palmar nodule. Nodules typically appear around the distal palmar crease over the MCP joint and distally over the PIP joint, but never over the distal interphalangeal (DIP) joint. Discomfort is rare but may consist of mild itching or aching pain during this highly active phase.
2. Involutional Stage
The nodules cease their rapid growth and begin to contract. Stress alignment of the myofibroblasts occurs along the lines of tension, and abundant Type III collagen is deposited (replacing the normal Type I collagen of the palmar fascia). The contraction of the nodule places immense tension on the normal fascia proximally, inducing fascial hypertrophy and the formation of distinct nodule-cord units.
3. Residual Phase
In the final stage, the cellularity decreases dramatically. The nodules shrink in size, leaving behind dense, acellular, and highly contracted fibrous cords. The clinical deformity is maximized and fixed during this stage.
Clinical Evaluation and Indications for Treatment
Physical Examination
Evaluation begins with a thorough inspection of both hands, noting skin pitting, nodules, and the presence of cords. The "tabletop test" (Hueston's test) is a simple screening tool: the patient is asked to place their hand flat on a hard surface. If the hand cannot be placed completely flat due to MCP or PIP flexion, the test is positive, indicating a functional contracture.
Precise goniometric measurement of the MCP, PIP, and DIP joints in both active and passive extension is mandatory to establish a baseline and guide treatment decisions.
Indications for Intervention
Observation is appropriate for painless nodules or mild contractures that do not impair function. Intervention is generally indicated when the disease interferes with activities of daily living. Specific biomechanical thresholds include:
1. MCP Joint Contracture: Greater than 30 degrees.
2. PIP Joint Contracture: Any degree of progressive contracture, as PIP joint contractures are notoriously difficult to correct once established and rapidly lead to secondary joint capsular contractures.
Surgical Management: Regional Fasciectomy
While minimally invasive options such as Needle Aponeurotomy (NA) and Collagenase Clostridium histolyticum (CCH) injections exist for specific, well-defined cords, Regional Fasciectomy remains the gold standard for extensive, multi-digit disease or severe PIP contractures.
Preoperative Preparation and Positioning
- The patient is positioned supine with the operative arm extended on a radiolucent hand table.
- General anesthesia or regional brachial plexus block is administered.
- A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is absolute paramount for the safe identification of displaced neurovascular bundles.
- Surgical loupe magnification (minimum 2.5x to 3.5x) is mandatory.
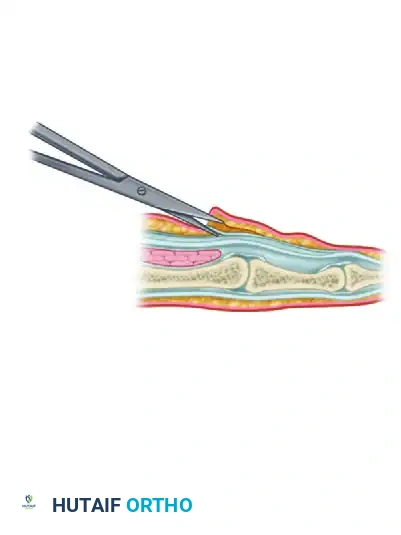
Surgical Approach and Incision
The choice of incision is critical to prevent postoperative scar contracture. Straight longitudinal incisions must be avoided as they will inevitably lead to secondary scar contractures.
* Bruner Zig-Zag Incision: Volar zig-zag incisions are made with the apices of the flaps ending at the mid-lateral lines of the digits, avoiding the flexion creases.
* Longitudinal Incision with Z-Plasties: A longitudinal incision is made directly over the palpable cord, and multiple Z-plasties are designed and executed during closure to lengthen the volar skin.
Step-by-Step Dissection
- Flap Elevation: The skin flaps are elevated meticulously. The dissection must remain superficial to the cord but deep to the subdermal vascular plexus to prevent flap necrosis. In areas of severe skin pitting, the skin must be sharply dissected off the underlying nodule.
- Identification of Neurovascular Bundles: This is the most critical step. The neurovascular bundles must be identified in normal, unscarred tissue proximal to the disease (in the palm) and distal to the disease (in the digit).
- Tracing the Bundle: Once identified, the neurovascular bundle is traced through the diseased tissue. If a spiral cord is present, the surgeon must anticipate the bundle being pulled superficially and toward the midline at the level of the PIP joint.
- Excision of the Cord: The diseased fascia (central, spiral, lateral, and natatory cords) is systematically excised. The goal is a regional fasciectomy (removing only the grossly diseased fascia), not a radical fasciectomy (removing all palmar fascia), as the latter carries an unacceptably high complication rate without improving outcomes.
- Joint Release: If the PIP joint does not fully extend after complete cord excision, a secondary joint contracture has occurred. This may require a step-cut lengthening of the volar plate or release of the accessory collateral ligaments.
Closure Techniques
- Primary Closure: Achieved if skin tension is minimal.
- Z-Plasty: Utilized to recruit lateral skin and lengthen the volar surface.
- McCash Open Palm Technique: In cases of severe contracture or older patients with poor skin quality, a transverse palmar incision is left completely open to heal by secondary intention. This dramatically reduces the risk of hematoma and allows for immediate mobilization, with excellent long-term functional results.
- Full-Thickness Skin Grafting (Dermofasciectomy): Indicated for recurrent disease or severe Dupuytren diathesis. The diseased skin and fascia are excised en bloc, and a full-thickness graft (often harvested from the groin or inner arm) is applied. This creates a "firebreak" that highly resists disease recurrence.
Postoperative Protocol and Rehabilitation
The success of a fasciectomy is heavily dependent on rigorous postoperative hand therapy.
1. Immediate Post-Op: The hand is placed in a bulky, non-compressive dressing with a volar plaster splint maintaining the digits in maximum safe extension.
2. Days 3-5: The initial dressing is removed. A custom thermoplastic extension splint is fabricated by a certified hand therapist.
3. Weeks 1-6: The patient begins active and active-assisted range of motion exercises to prevent tendon adhesions and joint stiffness. The extension splint is worn strictly at night and intermittently during the day.
4. Long-Term: Night splinting may be continued for 3 to 6 months to counteract the physiological forces of scar contraction.
Complications
Surgeons must be prepared to manage several potential complications:
* Hematoma: The most common complication, which can lead to flap necrosis and severe stiffness. Meticulous hemostasis upon tourniquet deflation is mandatory.
* Nerve Injury: Iatrogenic digital nerve transection occurs in 1-3% of primary cases and up to 10% of recurrent cases. Immediate microsurgical epineural repair is required if recognized intraoperatively.
* Flare Reaction: A hyperactive inflammatory response characterized by diffuse swelling, redness, and stiffness. Treated with aggressive therapy, NSAIDs, and occasionally short-course oral corticosteroids.
* Recurrence: Recurrence of the disease (in the same operative field) or disease extension (in previously uninvolved areas) is common, particularly in patients with a strong Dupuytren diathesis. Long-term patient follow-up and expectation management are essential.
===
You Might Also Like