Unlock Easier Access: Dorsal Approach for Phalanges and Interphalangeal Joints

Key Takeaway
Your ultimate guide to Unlock Easier Access: Dorsal Approach for Phalanges and Interphalangeal Joints starts here. The dorsal approach to the **phalanges and interphalangeal** joints is a surgical technique primarily for open reduction and internal fixation of fractures and dislocations in these structures. It provides easier bone access compared to volar or lateral approaches, as only the extensor mechanism lies between the skin and bone. Incisions are tailored to the specific pathology, allowing direct exposure.
Introduction and Epidemiology
The dorsal approach to the phalanges and interphalangeal joints remains the fundamental workhorse exposure for hand surgeons, orthopedic surgeons, and traumatologists. It is almost exclusively utilized for the open reduction and internal fixation (ORIF) of fractures, fracture-dislocations, and the management of complex extensor mechanism disruptions. Access to the osseous structures of the hand is markedly facilitated through the dorsal approach compared to volar or lateral exposures because the only deep anatomical structure interposed between the integument and the osseous architecture is the extensor mechanism.
Phalangeal and metacarpal fractures are among the most common skeletal injuries, accounting for approximately 10% of all fractures presenting to emergency departments. The proximal phalanx is particularly vulnerable to torsional and bending forces during athletic activities and industrial labor, frequently resulting in oblique, spiral, or comminuted fracture patterns. Interphalangeal joint dislocations, particularly of the proximal interphalangeal (PIP) joint, often involve intra-articular shear or avulsion fractures that demand precise anatomical reduction to prevent catastrophic post-traumatic arthrosis and stiffness.

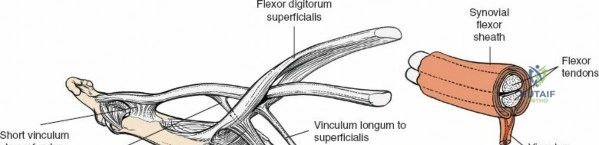
The primary advantage of the dorsal approach lies in its direct trajectory to the tension side of the bone, which is biomechanically advantageous for the application of tension band constructs, dorsal plating, and lag screw osteosynthesis. Furthermore, avoiding the volar aspect of the digit mitigates the risk of iatrogenic injury to the critical flexor tendon apparatus (flexor digitorum superficialis and profundus) and the delicate volar neurovascular bundles. Mastery of this surgical approach requires a comprehensive understanding of the dorsal soft tissue envelope, the intricate biomechanics of the extensor apparatus, and meticulous handling of the peritendinous structures to prevent postoperative adhesions.
Surgical Anatomy and Biomechanics
Integument and Subcutaneous Tissues
The skin overlying the dorsum of the hand and digits is uniquely adapted to accommodate the full excursion of digital flexion. It is thin, highly pliable, and relatively devoid of dense subcutaneous adipose tissue. The subcutaneous layer contains a robust network of dorsal veins and lymphatics. Preservation of these longitudinal venous channels during superficial dissection is paramount to prevent postoperative venous congestion, profound digital edema, and subsequent joint stiffness.
Neurovascular Anatomy
The sensory innervation to the dorsum of the digits is supplied by the terminal dorsal sensory branches of the radial and ulnar nerves. The radial nerve supplies the dorsal aspect of the radial three and a half digits, while the ulnar nerve supplies the ulnar one and a half digits. Notably, the dorsal branches typically only extend to the level of the PIP joint; distal to this, the dorsal skin receives its sensory innervation from dorsal branches of the proper volar digital nerves.
There is no true internervous plane available for use in the dorsal approach to the digits. Because the skin of the dorsum of the fingers receives a rich, overlapping sensory nerve supply from both the radial and ulnar aspects, clinically significant sensory denervation rarely occurs following midline or slightly curved dorsal longitudinal incisions.

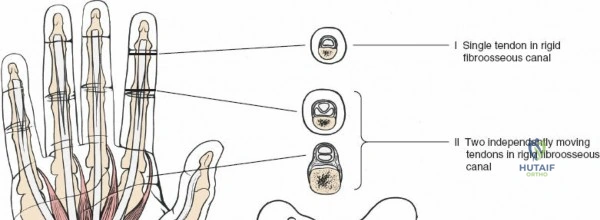
The Extensor Mechanism
The extensor mechanism is a highly complex, interconnected aponeurotic expansion that dictates the kinematics of the interphalangeal joints. Understanding its components is critical when performing a dorsal approach:
* Sagittal Bands: Stabilize the extensor digitorum communis (EDC) tendon centrally over the metacarpophalangeal (MCP) joint and facilitate MCP joint extension.
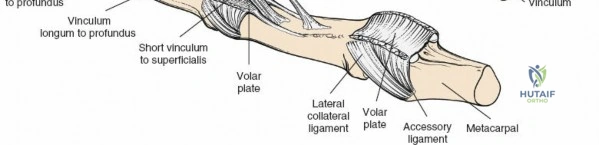
* Central Slip: The primary extensor of the PIP joint, inserting broadly onto the dorsal base of the middle phalanx.
* Lateral Bands: Formed by the bifurcation of the EDC and contributions from the intrinsic muscles (lumbricals and interossei). They bypass the PIP joint to converge distally.
* Terminal Tendon: The convergence of the lateral bands, inserting onto the dorsal base of the distal phalanx to extend the distal interphalangeal (DIP) joint.
* Triangular Ligament: Prevents volar subluxation of the lateral bands during PIP flexion.
* Transverse and Oblique Retinacular Ligaments: Coordinate the simultaneous extension of the PIP and DIP joints (Landsmeer's ligaments).
Osseous Biomechanics
The phalanges exhibit a distinct geometry, with a convex dorsal surface and a flat or slightly concave volar surface. This geometry means that the dorsal cortex is under tension during active grasp and pinch, making it the biomechanically ideal surface for the application of rigid internal fixation (e.g., plates and screws). The condylar shape of the phalangeal heads dictates a "cam effect," wherein the collateral ligaments are lax in extension and taut in flexion. This principle dictates that digits should be splinted in MCP flexion and IP extension to prevent collateral ligament contracture.
Indications and Contraindications
The decision to utilize a dorsal approach is dictated by the specific fracture pattern, the location of the pathology, and the required fixation construct. The approach is highly versatile but must be carefully selected to avoid unnecessary morbidity to the extensor apparatus.
Operative Indications
The dorsal approach is indicated for a wide array of traumatic and reconstructive procedures. Intra-articular fractures of the PIP joint, particularly those involving the dorsal lip (e.g., central slip avulsions) or complex pilon-type fractures, are optimally visualized dorsally. Diaphyseal fractures of the proximal and middle phalanges that are irreducible, unstable, or demonstrate rotational malalignment also necessitate this exposure. Furthermore, the approach is utilized for extensor tenolysis, capsulotomies for joint contractures, arthrodesis of the PIP or DIP joints, and the excision of dorsal osseous or soft tissue neoplasms (e.g., enchondromas, ganglion cysts).
Contraindications
Absolute contraindications are rare but include active superficial dorsal skin infections or severe dorsal soft tissue crush injuries where an incision would precipitate skin necrosis. Relative contraindications include isolated volar shear fractures of the phalangeal bases, which are better addressed via a volar approach to allow for direct buttress plating. Additionally, fractures requiring complex volar flexor tendon repair simultaneously may be better served by a mid-lateral or volar exposure to access both compartments without creating excessive circumferential dissection.
Operative Versus Non Operative Management Parameters
| Pathology Classification | Operative Indication Parameters | Non Operative Indication Parameters |
|---|---|---|
| Proximal Phalanx Diaphyseal Fracture | > 2mm shortening, > 10 degrees angulation, any rotational deformity, multiple concurrent fractures | Nondisplaced, stable post-closed reduction, no rotational malalignment |
| Middle Phalanx Fracture | Intra-articular step-off > 1mm, unstable oblique/spiral patterns | Transverse midshaft fractures stable in functional splinting |
| PIP Joint Fracture Dislocation | > 30% articular surface involvement, persistent subluxation, V-sign on lateral radiograph | < 30% articular surface, concentrically reduced and stable in active arc of motion |
| Metacarpal Head/Neck Fracture | Intra-articular displacement, severe volar comminution, unacceptable angulation | Acceptable angulation (varies by digit: up to 40-50 degrees in 5th digit) |

Pre Operative Planning and Patient Positioning
Imaging Modalities
Meticulous preoperative planning begins with high-quality, orthogonal radiographs of the specific digit involved. A true anteroposterior (AP), true lateral, and oblique view are mandatory. The true lateral is particularly critical for assessing the concentricity of the interphalangeal joints and the degree of volar or dorsal comminution. In cases of complex intra-articular fractures (e.g., PIP joint pilon fractures), a fine-cut computed tomography (CT) scan with 3D reconstructions is highly recommended to map the articular fragments and plan the trajectory of interfragmentary lag screws or the placement of a condylar plate.
Patient Positioning and Anesthesia
Place the patient in a supine position on the operating table. The operative upper extremity is extended onto a radiolucent hand table or arm board. The forearm is pronated to bring the dorsum of the hand into the optimal viewing field of the surgeon.
Anesthesia can be tailored to the patient and the complexity of the procedure. Regional anesthesia, such as an axillary or supraclavicular brachial plexus block, provides excellent intraoperative operating conditions and prolonged postoperative analgesia. Alternatively, the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique, utilizing a mixture of lidocaine and epinephrine, is increasingly utilized. WALANT allows for intraoperative active motion testing to assess the stability of the fracture fixation and the excursion of the extensor mechanism.
Tourniquet Application
If WALANT is not utilized, exsanguinate the arm using an Esmarch or soft rubber bandage. Inflate a pneumatic tourniquet applied to the proximal arm or forearm (depending on surgeon preference and the anticipated length of the procedure). The standard tourniquet pressure is typically set to 250 mmHg or 100 mmHg above the patient's systolic blood pressure. Strict adherence to tourniquet time limits (ideally less than 120 minutes) is imperative to prevent ischemic neuropraxia and reperfusion injury to the intrinsic musculature.
Detailed Surgical Approach and Technique
Landmarks Identification
Precise identification of the osseous landmarks is the first step in the surgical execution. Passively flex and extend the metacarpophalangeal (MCP), proximal interphalangeal (PIP), and distal interphalangeal (DIP) joints to dynamically identify their exact joint lines. The dorsal joint lines are palpable as distinct depressions just distal to the condylar heads of the metacarpals and phalanges. Mark the planned incision with a sterile surgical marker prior to exsanguination.
Selection of Incisions
The choice of incision is highly dependent on the specific pathology to be treated, the required exposure, and the anticipated hardware.
Metacarpophalangeal Joint Exposure
Make a gently curved incision over the dorsal aspect of the MCP joint. The incision can be curved in either direction; however, as a biomechanical rule, a radially curved incision is preferred over the second MCP joint (index finger) to avoid the ulnar drift forces, and a dorsoulnar curved incision is preferred over the fifth MCP joint (small finger). This curving prevents the resulting scar from lying directly over the central axis of the extensor tendon, thereby minimizing tethering.

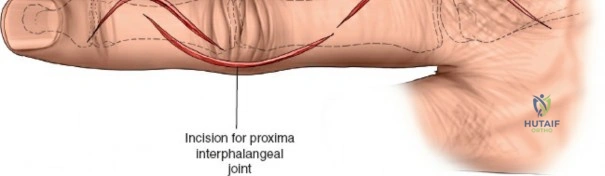
Proximal Interphalangeal Joint Exposure
For the PIP joint, two primary incision types are utilized. The first is a straight longitudinal incision placed directly over the midline of the joint. The second is a curved or lazy-S incision at the same site.
* The Straight Incision: The primary advantage of the straight incision is that it avoids the creation of a skin flap, thereby preserving the delicate microvascular supply to the dorsal skin edges and reducing the risk of marginal necrosis.
* The Curved Incision: The curve should be designed to avoid the radial border of the index finger and the ulnar border of the little finger (the contact surfaces during pinch and grasp). The curved incision avoids the complication of a linear scar contracture directly over the joint and prevents the skin scar and the underlying tendon repair from adhering in the same longitudinal line.
Middle Phalanx Exposure
Make either a gently curved incision centered over the fracture apex or a straight incision at the same site. The position and length of the incision will depend entirely on the pathology to be treated and the length of the planned fixation plate. The advantages and disadvantages of these incisions are identical to those described for the PIP joint approach.
Superficial Surgical Dissection
Deepen the skin incision through the dermis using a scalpel, then transition to blunt dissection utilizing tenotomy scissors or a hemostat. Extreme care must be taken to identify and avoid dividing the longitudinal branches of the dorsal venous network. Ligation of too many dorsal veins will result in profound postoperative digital swelling. Retract and elevate the skin and subcutaneous tissue as a single, full-thickness layer to expose the underlying paratenon and the extensor mechanism. Do not dissect between the skin and the subcutaneous fat, as this will devascularize the skin flaps.
Deep Surgical Dissection and Extensor Mechanism Management
Once the extensor mechanism is exposed, access to the underlying bone requires mobilizing or splitting the tendon. Several techniques exist, and the choice depends on the fracture location.
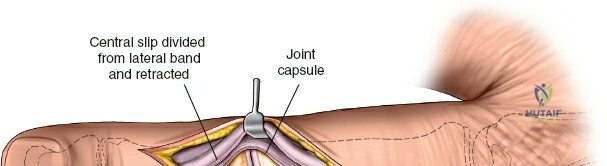
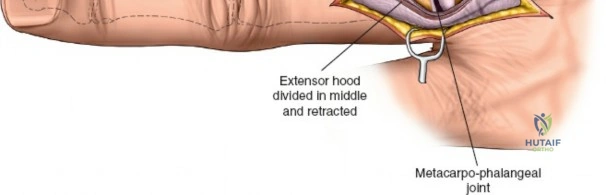
Midline Tendon Splitting
For diaphyseal fractures of the proximal phalanx, a longitudinal midline split of the extensor tendon can be performed. The tendon is incised sharply in the midline, and the two halves are retracted radially and ulnarly. This provides direct access to the dorsal periosteum. However, this technique must be used with caution near the PIP joint to avoid damaging the central slip insertion.
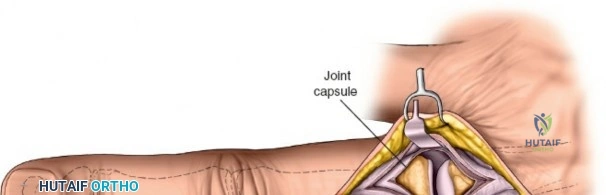
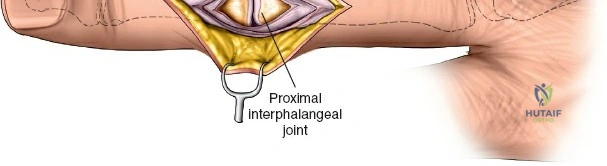
The Chamay Approach
For exposure of the distal third of the proximal phalanx and the PIP joint, a Chamay approach is highly effective. This involves a distally based, V-shaped incision through the central slip of the extensor mechanism. The apex of the V is placed proximally in the diaphysis, and the limbs extend distally toward the lateral bands. This flap is elevated distally, providing excellent visualization of the PIP joint articular surface. During closure, the V is repaired with non-absorbable sutures.
Paratendinous Approaches
Alternatively, the extensor mechanism can be mobilized in its entirety and retracted either radially or ulnarly. This requires incising the sagittal bands or the transverse retinacular ligaments. While this spares the tendon substance, it requires meticulous repair of the stabilizing ligaments to prevent postoperative tendon subluxation.
Fracture Reduction and Osteosynthesis
Following exposure, the fracture hematoma is evacuated, and the fracture ends are debrided of interposed soft tissue. Anatomical reduction is achieved using pointed reduction forceps or dental picks.
* Lag Screw Fixation: For long oblique or spiral fractures, interfragmentary lag screws (typically 1.0mm to 1.5mm) provide absolute stability. The glide hole is drilled in the near cortex, the thread hole in the far cortex, and the screw is inserted to compress the fracture.
* Plate Osteosynthesis: For transverse, short oblique, or comminuted fractures, a dorsal mini-fragment plate (1.2mm, 1.5mm, or 2.0mm system) is applied. The plate functions as a tension band on the dorsal surface. Care must be taken to ensure the plate is low-profile to prevent subsequent extensor tendon irritation.
* Kirschner Wires: For highly comminuted intra-articular fractures where hardware prominence is a concern, fine K-wires (0.8mm or 1.0mm) can be utilized, often buried beneath the skin.
Closure
Following fluoroscopic confirmation of reduction and hardware placement, the surgical site is copiously irrigated. The extensor mechanism must be meticulously repaired using a continuous or interrupted technique with 4-0 or 5-0 non-absorbable or slowly absorbable sutures. A precise repair is critical to prevent extensor lag. The skin is closed with interrupted nylon or prolene sutures. A sterile, non-adherent dressing is applied, followed by a compressive wrap and a plaster splint immobilizing the digit in the intrinsic-plus position (MCP joints flexed to 70-90 degrees, IP joints fully extended).

Complications and Management
Despite meticulous surgical technique, the dorsal approach to the phalanges carries specific risks, primarily related to the intimate relationship between the osseous structures and the extensor mechanism. The extensor apparatus is highly unforgiving of scarring, shortening, or disruption.
Extensor Lag and Adhesions
The most frequent complication following a dorsal approach is the development of an extensor lag at the PIP or DIP joint. This occurs due to relative lengthening of the central slip or terminal tendon, or secondary to dense adhesions between the extensor tendon, the dorsal hardware, and the underlying healing callus. A prominent dorsal plate acts as a mechanical block to tendon excursion.
Joint Stiffness
Interphalangeal joint stiffness is a ubiquitous risk in hand trauma. It can manifest as a loss of flexion (due to dorsal capsular contracture or extensor adhesions) or a loss of extension (due to volar plate contracture). Prolonged immobilization exacerbates this risk exponentially.
Hardware Prominence and Tendon Rupture
Due to the paucity of dorsal soft tissue, plates and screws are frequently palpable and can cause mechanical irritation to the overlying tendon. In severe cases, chronic attrition over a prominent screw head can lead to delayed rupture of the extensor tendon.
Infection and Wound Dehiscence
Marginal skin necrosis can occur if full-thickness flaps are not maintained or if the incision design compromises the vascular supply. This can progress to deep infection, potentially compromising the osteosynthesis and leading to osteomyelitis.

Complications Incidence and Salvage Strategies
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy |
|---|---|---|---|
| Extensor Tendon Adhesions | 20 - 40% | Prolonged immobilization, prominent hardware, excessive periosteal stripping | Aggressive hand therapy, surgical tenolysis, hardware removal after fracture consolidation |
| Extensor Lag (PIP Joint) | 15 - 30% | Central slip attenuation, inadequate repair, premature active flexion | Splinting (static progressive), secondary central slip reconstruction |
| Joint Stiffness (Loss of Flexion) | 25 - 50% | Capsular contracture, intra-articular step-off, edema | Dorsal capsulectomy, manipulation under anesthesia (MUA), hardware removal |
| Hardware Prominence | 30 - 40% | Use of thick plates on the middle/distal phalanx, inadequate screw countersinking | Elective hardware removal at 4-6 months post-operatively |
| Superficial Infection / Dehiscence | 2 - 5% | Poor flap handling, excessive tourniquet time, smoking | Oral or IV antibiotics, local wound care, rarely requires flap coverage |
Post Operative Rehabilitation Protocols
The ultimate functional outcome following surgical intervention via the dorsal approach is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. The paradigm in modern hand trauma surgery has shifted heavily toward Early Active Motion (EAM) to prevent the devastating complication of tendon adhesions.
Phase 1 Protection and Early Motion (Days 3 to 14)
If rigid internal fixation (e.g., lag screws or stable plating) has been achieved, early active motion is initiated within 3 to 5 days postoperatively, once the initial inflammatory edema has subsided. The patient is fitted with a custom thermoplastic splint. For proximal phalangeal fractures, a hand-based splint holding the MCP joints in 70 degrees of flexion and allowing full IP joint motion is utilized. Therapy focuses on isolated PIP and DIP joint active flexion and extension to facilitate extensor tendon gliding over the hardware. Passive stretching is strictly contraindicated at this stage to prevent hardware failure or tendon rupture.
Phase 2 Intermediate Rehabilitation (Weeks 2 to 6)
Sutures are typically removed between days 10 and 14. Scar massage and desensitization techniques are initiated to prevent the skin from adhering to the underlying tendon. Dynamic splinting may be introduced if a specific motion deficit is identified (e.g., a dynamic extension splint for a developing PIP flexion contracture). Radiographic evaluation is performed at 2, 4, and 6 weeks to monitor for maintenance of reduction and early callus formation.
Phase 3 Strengthening and Return to Function (Weeks 6 to 12)
Once clinical and radiographic union is confirmed (typically around 6 weeks), splinting is discontinued. Progressive strengthening exercises, utilizing putty and grip strengtheners, are initiated. If significant stiffness persists despite conservative therapy, surgical interventions such as tenolysis or capsulectomy are generally delayed until at least
Clinical & Radiographic Imaging